Inflammatory | Synovitis | Deformity | Multijoint
NALEBUFF THUMB DEFORMITIES
Critical Must-Knows
- Ulnar drift from MCP radial collateral destruction + extensor subluxation
- Boutonniere = PIP flexion + DIP extension (central slip rupture)
- Swan-neck = PIP hyperextension + DIP flexion (volar plate laxity)
- Medical optimization before surgery - stop methotrexate 2 weeks pre-op
- Proximal-to-distal surgery - wrist before digits, correct deforming forces first
Clinical Pearls
- "RF positive 70%, anti-CCP more specific (95%) for RA diagnosis
- "Caput ulnae syndrome = dorsal ulnar head prominence from DRUJ destruction
- "Vaughan-Jackson lesion = EDM/EDC rupture from attrition on ulnar head
- "Synovectomy only effective if done under 6 months of synovitis onset
Clinical Imaging
Imaging Gallery



Critical RA Hand Exam Points
Ulnar Drift Mechanism
Radial collateral ligament destruction. Extensor tendon subluxates ulnarly. Intrinsics pull fingers into ulnar deviation. Progressive worsening with grip.
Deformity Recognition
Boutonniere vs Swan-neck. Boutonniere = PIP flexion from central slip rupture. Swan-neck = PIP hyperextension from volar plate laxity or FDS rupture.
Tendon Rupture Sequence
Vaughan-Jackson lesion. EDM ruptures first, then EDC ring, then EDC middle. Attrition on dorsal ulnar head (caput ulnae). Early Darrach or hemiresection.
Surgical Timing
Disease control first. Optimize medical management before reconstructive surgery. DMARDs within 2 years critical. Address proximal deformities before distal.
Quick Decision Guide - RA Hand Surgery
| Deformity | Stage | Treatment | Key Pearl |
|---|---|---|---|
| Early synovitis under 6 months | No deformity yet | Synovectomy + medical optimization | Window of opportunity - DMARDs critical |
| MCP ulnar drift, flexible | Passively correctable | MCP arthroplasty + soft tissue rebalancing | Silicone implants standard, 80% satisfaction |
| Boutonniere deformity, fixed | PIP flexion contracture over 40° | PIP arthrodesis in function | Arthroplasty fails in fixed contracture |
| Caput ulnae + tendon rupture | EDM/EDC rupture | Darrach + tendon transfer/graft | Prevent further ruptures with DRUJ excision |
BUTTONBoutonniere Deformity Pathomechanics
| B | Band (central slip) disruption Central slip ruptures or attenuates |
| U | Ulnar/radial bands migrate volar Lateral bands slide volar to PIP axis |
| T | Terminal extension preserved DIP extends (lateral bands intact) |
| T | Tight lateral bands Shortened lateral bands resist correction |
| O | Oblique retinacular ligament contracts ORL shortens, worsens deformity |
| N | No passive correction if chronic Fixed after 6-12 months, needs arthrodesis |
| B | Band (central slip) disruption Central slip ruptures or attenuates | T | Terminal extension preserved DIP extends (lateral bands intact) | O | Oblique retinacular ligament contracts ORL shortens, worsens deformity |
| U | Ulnar/radial bands migrate volar Lateral bands slide volar to PIP axis | T | Tight lateral bands Shortened lateral bands resist correction | N | No passive correction if chronic Fixed after 6-12 months, needs arthrodesis |
Hook:BUTTON yourself up wrong - PIP stuck flexed, can't extend like a buttonhole!
SWANSwan-Neck Deformity Causes
| S | Slip (central) hypertrophy Intrinsic tightness pulls PIP into extension |
| W | Weak volar plate Volar plate attenuation allows hyperextension |
| A | Attenuated FDS FDS rupture removes PIP flexion force |
| N | Nodules in flexor tendon Trigger finger causes MCP flexion, compensatory PIP extension |
| S | Slip (central) hypertrophy Intrinsic tightness pulls PIP into extension | A | Attenuated FDS FDS rupture removes PIP flexion force |
| W | Weak volar plate Volar plate attenuation allows hyperextension | N | Nodules in flexor tendon Trigger finger causes MCP flexion, compensatory PIP extension |
Hook:SWAN with elegant neck extended - PIP hyperextends while DIP flexes!
BMI-CSSNalebuff Thumb Classification
| B | Boutonniere (Type I) MCP flexion, IP extension - MCP synovitis |
| M | MCP unstable (Type II) MCP hyperextension, IP flexion - MCP ligament laxity |
| I | IP flexion (Type III) Swan-neck from CMC subluxation |
| C | CMC arthritis (Type IV) CMC joint destruction, adduction contracture |
| S | Swan-neck combination (Type V) MCP hyperextension + IP flexion, multiple joints |
| S | Stiff arthritis mutilans (Type VI) Global destruction, bone resorption |
| B | Boutonniere (Type I) MCP flexion, IP extension - MCP synovitis | I | IP flexion (Type III) Swan-neck from CMC subluxation | S | Swan-neck combination (Type V) MCP hyperextension + IP flexion, multiple joints |
| M | MCP unstable (Type II) MCP hyperextension, IP flexion - MCP ligament laxity | C | CMC arthritis (Type IV) CMC joint destruction, adduction contracture | S | Stiff arthritis mutilans (Type VI) Global destruction, bone resorption |
Hook:BMI-CSS classification - B (boutonniere) vs swan-neck types, CMC to catastrophic!
Overview and Epidemiology
Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease affecting approximately 1% of the population worldwide. The hand is involved in 90% of patients, making it the most common site of RA manifestation. Early diagnosis and treatment with disease-modifying antirheumatic drugs (DMARDs) within the first 2 years significantly impacts disease progression and outcomes.
Why RA Hand Management Matters
Hand involvement in RA causes progressive functional disability through synovitis, tendon rupture, and joint destruction. Modern biologic DMARDs have revolutionized medical management, but surgical intervention remains critical for correcting established deformities. The key is medical optimization before surgery and addressing deformities in a proximal-to-distal sequence to correct deforming forces.
Demographics
- Age: Peak onset 40-60 years
- Gender: 3:1 female predominance
- Genetics: HLA-DR4 association (70%)
- Smoking: Doubles RA risk, worsens severity
Hand Involvement Patterns
- MCP joints: Most commonly affected (95%)
- PIP joints: 80% involvement
- Wrist: 60-70% early in disease
- DIP joints: Rarely affected (under 10%)
- Thumb: Nalebuff deformities in 50%
Pathophysiology
Synovial Inflammation Cascade
RA begins with immune-mediated synovial inflammation driven by T cells, B cells, and inflammatory cytokines (TNF-alpha, IL-6). Synovial hypertrophy (pannus formation) invades cartilage and bone, causing progressive joint destruction. Unchecked inflammation leads to ligament destruction, tendon attrition, and bone erosion.
Pathophysiologic Sequence in RA Hand
Disease Progression
- Pannus formation: Synovial hypertrophy with inflammatory cells
- Cartilage invasion: Proteases degrade articular cartilage
- Bone erosion: Marginal erosions at joint edges
- Ligament weakening: Collateral and volar plate stretch
- Extensor subluxation: Radial collateral destruction allows ulnar drift
- Central slip attenuation: Boutonniere deformity develops
- Volar plate laxity: Swan-neck deformity from PIP hyperextension
- Tendon rupture: Attrition on roughened bone (Vaughan-Jackson, Mannerfelt)
- Joint destruction: Bone-on-bone arthritis
- Contractures: Soft tissue shortening prevents passive correction
- Ankylosis: Spontaneous fusion in some joints
- Arthritis mutilans: Severe bone resorption (opera-glass hand)
Specific Deformity Mechanisms
Deformity Pathomechanics
| Deformity | Primary Pathology | Secondary Changes | Result |
|---|---|---|---|
| Ulnar drift (MCP) | Radial collateral ligament destruction | Extensor subluxates ulnarly, intrinsics pull fingers ulnar | Progressive ulnar deviation, worst with grip |
| Boutonniere (PIP) | Central slip rupture/attenuation | Lateral bands migrate volar to PIP axis, ORL contracts | PIP flexion, DIP extension, fixed after 6-12 months |
| Swan-neck (PIP) | Volar plate laxity or FDS rupture | Intrinsic tightness extends PIP, lateral bands tighten | PIP hyperextension, DIP flexion, can't hook |
| Z-deformity (thumb) | CMC subluxation (Type III) or MCP hyperextension (Type II) | Compensatory IP flexion for pinch | Loss of opposition and pinch strength |
Classification Systems
Nalebuff Classification of RA Thumb Deformities
| Type | Deformity Pattern | Primary Pathology | Treatment |
|---|---|---|---|
| Type I (Boutonniere) | MCP flexion, IP extension | MCP synovitis → volar plate stretching | MCP arthroplasty or arthrodesis |
| Type II (Swan-neck) | MCP hyperextension, IP flexion | MCP ligament laxity → hyperextension | MCP fusion or volar capsulodesis |
| Type III (CMC swan-neck) | CMC subluxation, MCP hyperext, IP flex | CMC synovitis → adduction collapse | CMC stabilization + MCP fusion |
| Type IV (CMC arthritis) | CMC arthritis, adduction contracture | CMC joint destruction | CMC arthroplasty or arthrodesis |
| Type V (Combined) | Multiple joint involvement | Progressive pannus at all joints | Staged reconstruction, proximal to distal |
| Type VI (Arthritis mutilans) | Bone resorption, instability | Severe osteolysis | Fusion if salvageable, otherwise adaptive |
Type I vs Type II Distinction
Type I (Boutonniere): MCP is the problem joint (flexed from synovitis), IP compensates with extension. Type II (Swan-neck): MCP ligaments fail allowing hyperextension, IP compensates with flexion for pinch. Type III is swan-neck but driven by CMC subluxation proximally. Knowing the primary pathology determines surgical target.
2010 ACR/EULAR Classification Criteria (Diagnosis)
The 2010 ACR/EULAR criteria replaced the 1987 ACR criteria to enable earlier classification of RA, focusing on features predicting persistent and erosive disease rather than late deformity. A patient with synovitis in at least one joint and no better alternative diagnosis is classified as definite RA with a score of 6 or more out of 10 across four domains.
2010 ACR/EULAR Criteria - Scoring Domains
| Domain | Category | Score |
|---|---|---|
| Joint involvement | 1 large joint | 0 |
| Joint involvement | 2-10 large joints | 1 |
| Joint involvement | 1-3 small joints | 2 |
| Joint involvement | 4-10 small joints | 3 |
| Joint involvement | Over 10 joints (at least 1 small) | 5 |
| Serology | Negative RF and anti-CCP | 0 |
| Serology | Low-positive RF or anti-CCP | 2 |
| Serology | High-positive RF or anti-CCP | 3 |
| Acute-phase reactants | Normal CRP and ESR | 0 |
| Acute-phase reactants | Abnormal CRP or ESR | 1 |
| Symptom duration | Less than 6 weeks | 0 |
| Symptom duration | 6 weeks or more | 1 |
2010 ACR/EULAR Rheumatoid Arthritis Classification Criteria
- Joint ACR/EULAR initiative replacing the 1987 criteria, which lacked sensitivity in early disease
- Score of 6 or more of 10 across four domains (joints, serology, acute-phase reactants, symptom duration) classifies definite RA
- Requires at least one joint with definite clinical synovitis not better explained by another diagnosis
- Deliberately weights small-joint involvement and high-titre serology to capture patients at risk of persistent, erosive disease early
Clinical Presentation
History
- Morning stiffness: Over 1 hour (vs OA under 30 min)
- Symmetric involvement: Both hands, multiple joints
- Systemic symptoms: Fatigue, fever, weight loss
- Pain pattern: Worse with rest, improves with activity
- Functional loss: Difficulty with grip, pinch, fine motor
- Extra-articular: Nodules, lung involvement, vasculitis
Examination
- Look: Swelling (boggy, soft), deformities, nodules, skin thinning
- Feel: Warm, boggy MCP/PIP synovitis, ulnar head prominence
- Move: Reduced ROM, pain at end-range, crepitus
- Function: Pinch/grip strength, ulnar drift with grip
- Tendons: Trigger fingers, palpable ruptures
Key Physical Findings
Caput ulnae syndrome: Dorsal prominence of distal ulna from DRUJ destruction. Ulnar head becomes:
- Prominent dorsally
- Painful with forearm rotation
- Site of extensor tendon attrition (Vaughan-Jackson lesion)
Vaughan-Jackson lesion: Sequential rupture of ulnar-sided extensors:
- EDM (extensor digiti minimi) - first to rupture
- EDC ring finger - second
- EDC middle finger - third
- Pattern: ulnar to radial progression
Mannerfelt lesion: FPL rupture from attrition on volar scaphoid osteophyte. Less common than Vaughan-Jackson but causes complete loss of thumb IP flexion.
Distinguish RA from OA
RA features:
- Morning stiffness over 1 hour
- Soft, boggy swelling (synovitis)
- Symmetric involvement
- Spares DIP joints (unlike OA)
- Systemic features
- RF/anti-CCP positive
OA features:
- Morning stiffness under 30 minutes
- Hard, bony swelling (osteophytes = Heberden's/Bouchard's nodes)
- Asymmetric, wear pattern
- Affects DIP joints (Heberden's nodes)
- No systemic features
Differential Diagnosis of the Inflammatory or Deformed Hand
Differential Diagnosis - RA Hand vs Mimics
| Condition | Joint Pattern | Key Discriminators | Serology / Investigation |
|---|---|---|---|
| Rheumatoid arthritis | Symmetric MCP/PIP/wrist, spares DIP | Boggy synovitis, ulnar drift, marginal erosions, rheumatoid nodules | RF and anti-CCP positive; anti-CCP highly specific |
| Psoriatic arthritis | DIP involvement, asymmetric, ray/dactylitis | Nail pitting, dactylitis (sausage digit), skin psoriasis, enthesitis | RF and anti-CCP usually negative; pencil-in-cup erosions on XR |
| Erosive (inflammatory) osteoarthritis | DIP and PIP, asymmetric | Heberden/Bouchard nodes, gull-wing central erosions, bony hard swelling | Seronegative; normal or mildly raised CRP |
| Systemic lupus erythematosus (Jaccoud arthropathy) | MCP, reducible deformity | Deformity passively correctable, non-erosive on XR despite ulnar drift | ANA positive, anti-CCP usually negative (distinguishes from RA) |
| Gout / CPPD | Asymmetric, mono/oligoarticular | Tophi, acute attacks, chondrocalcinosis (CPPD) | Negatively (urate) or positively (CPPD) birefringent crystals |
The Anti-CCP Discriminator
Anti-CCP is the single most useful serological discriminator: it is approximately 96-98% specific for RA (Schellekens 2000) and is typically negative in psoriatic arthritis, erosive OA and Jaccoud arthropathy of SLE. A correctable (non-erosive) ulnar drift with positive ANA but negative anti-CCP points to lupus rather than RA.
Investigations
Diagnostic Workup
Rheumatoid factor (RF):
- Positive in 70% of RA patients
- Sensitivity 70%, specificity 85%
Anti-CCP antibodies:
- Positive in 70% of RA patients
- More specific (95%) than RF
- Predicts erosive disease
Inflammatory markers:
- ESR, CRP elevated during flares
- Track disease activity
Standard hand series: PA, lateral, oblique views
Early findings:
- Periarticular osteopenia
- Soft tissue swelling
- Joint space narrowing (symmetric)
Late findings:
- Marginal erosions (at joint edges)
- Subluxations and deformities
- Bone resorption (arthritis mutilans)
- Ankylosis
Indications:
- Early disease detection (synovitis before x-ray changes)
- Assess tendon integrity pre-operatively
- Monitor DMARD response
MRI findings:
- Synovial enhancement with contrast
- Bone marrow edema
- Tendon tenosynovitis
- Early erosions
Anti-CCP Specificity for RA
Anti-CCP antibodies are 95% specific for RA compared to RF at 85%. Presence of anti-CCP predicts more aggressive, erosive disease and guides earlier DMARD initiation. Patients with high anti-CCP titers benefit from biologic agents earlier in the disease course.
Management Algorithm
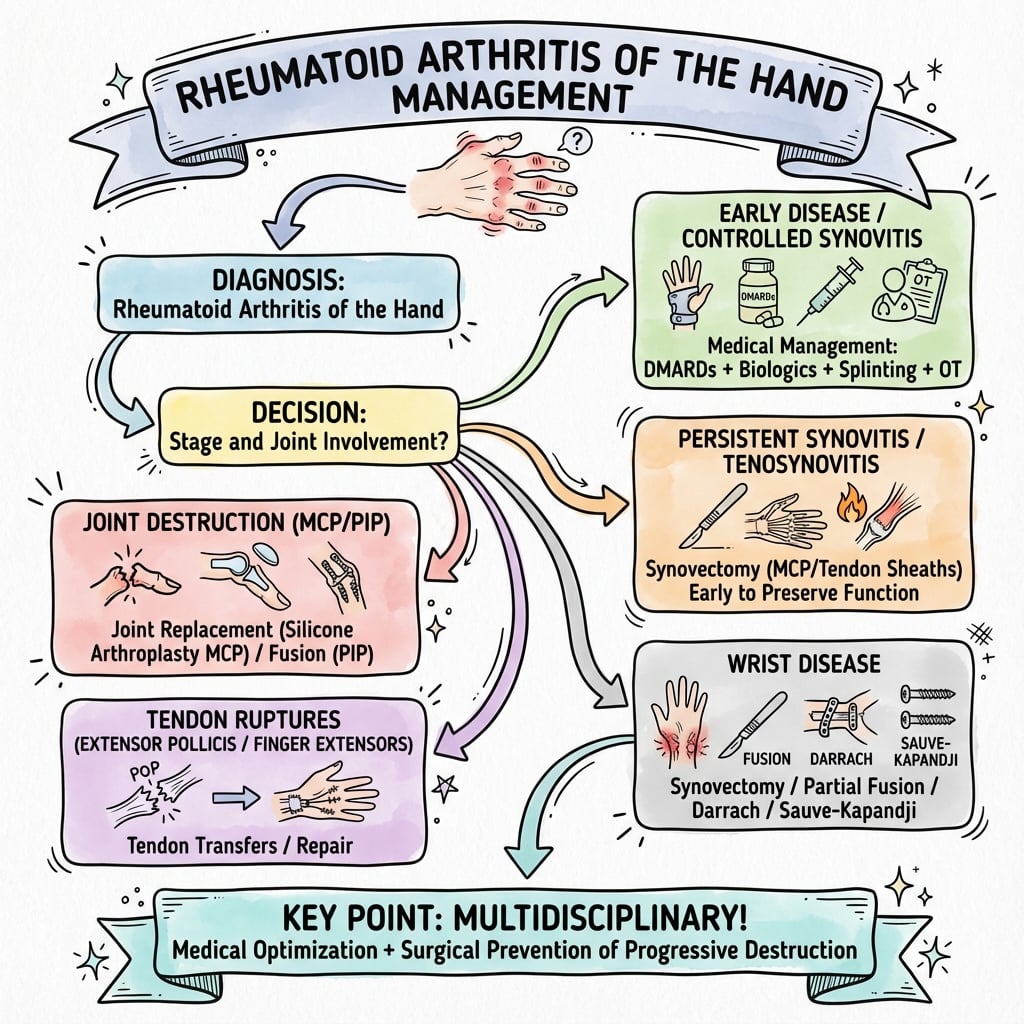
Medical Management (Primary)
RA Medical Management Protocol
Methotrexate:
- Gold standard DMARD
- 10-25mg weekly, oral or subcutaneous
- Add folic acid 5mg daily
- Monitor LFTs, FBC every 3 months
Alternative: Sulfasalazine, hydroxychloroquine
Add biologic DMARD:
- TNF-alpha inhibitors (adalimumab, etanercept)
- IL-6 inhibitors (tocilizumab)
- B-cell depletion (rituximab)
- JAK inhibitors (tofacitinib)
Target: Low disease activity or remission
NSAIDs: Short-term for pain/inflammation
Corticosteroids:
- Prednisolone 5-10mg daily during flares
- Intra-articular injection for single joint synovitis
- Bridge therapy while DMARDs take effect (6-12 weeks)
Window of Opportunity - First 2 Years
DMARD initiation within 2 years of symptom onset is critical. Early aggressive treatment prevents erosive disease, preserves joint function, and reduces need for surgery. Delay beyond 2 years results in irreversible joint damage.
Surgical Indications
Surgery indicated when:
- Persistent pain despite optimal medical management
- Functional impairment affecting ADLs or work
- Tendon rupture or impending rupture (tenosynovitis)
- Progressive deformity with joint destruction
- Nerve compression (carpal tunnel syndrome common in RA)
Surgical Technique
MCP Joint Arthroplasty with Soft Tissue Rebalancing
Consent Points
- Implant fracture/failure: 10-20% at 10 years
- Recurrent deformity: 10-15% ulnar drift recurrence
- Infection: 2-3% risk (higher in RA)
- Stiffness: ROM reduced from pre-op in 30%
- Sensory loss: Digital nerve injury rare (under 2%)
Equipment Checklist
- Silicone implants: Swanson or Sutter design, sizes 0-3
- Bone reamers: MCP head and base reamers
- Saw: Sagittal saw for bone resection
- Sutures: 3-0 and 4-0 for soft tissue repair
- K-wires: 0.045" for temporary fixation
Surgical Steps
MCP Arthroplasty Procedure
Dorsal longitudinal incision over MCP joints:
- Can do single incision for index through small (4 joints)
- Or individual incisions per digit
- Elevate skin flaps to expose extensor mechanism
Split extensor hood longitudinally:
- Incise between sagittal band and extensor tendon
- Reflect radial-sided hood ulnarly
- Expose MCP joint capsule
- Excise hypertrophic synovium completely
- Remove pannus from joint and tendon sheath
- Send specimen for culture (rule out infection)
Resect MCP joint:
- Remove metacarpal head with sagittal saw
- Ream intramedullary canal of metacarpal
- Ream proximal phalanx base
- Preserve collateral ligament origins if possible
- Trial silicone implant sizing
- Insert implant into metacarpal canal first
- Reduce MCP joint
- Insert distal stem into phalanx
- Confirm alignment and smooth ROM
Correct ulnar drift:
- Release ulnar sagittal band and intrinsics
- Tighten radial sagittal band (reef)
- Centralize extensor tendon over MCP
- Consider radial collateral ligament reconstruction
Extensor hood repair:
- Close hood with 3-0 braided suture
- Ensure tendon centralizes with finger flexion
- Close skin with 4-0 nylon
- Apply bulky dressing
- Dynamic extension splint with MCP extension, radial deviation
- Outrigger splint worn for 6 weeks
Soft Tissue Rebalancing is Key
Implant alone will fail without soft tissue rebalancing. The deforming forces (intrinsics pulling ulnar, sagittal band incompetent radially) persist after arthroplasty. Ulnar intrinsic release + radial sagittal band tightening prevents recurrent ulnar drift. 30% of recurrent deformity is from inadequate soft tissue balancing.
Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Infection | 2-5% | Immunosuppression (MTX, biologics), corticosteroids, diabetes | Aggressive antibiotics, consider implant removal if deep |
| Implant fracture (MCP arthroplasty) | 10-20% at 10 years | High-demand activities, poor bone quality | Observation if painless, revision arthroplasty or fusion if symptomatic |
| Recurrent ulnar drift | 10-15% | Inadequate soft tissue rebalancing, poor compliance with splinting | Revision soft tissue balancing, intrinsic release |
| Stiffness (worse ROM) | 20-30% | Prolonged immobilization, poor therapy compliance | Hand therapy, dynamic splinting, may need manipulation |
| Nonunion (arthrodesis) | 5-10% | Smoking, corticosteroids, poor bone quality | Revision fusion with bone graft if symptomatic |
| Tendon rupture (extensor) | 3-5% | Unaddressed caput ulnae, continued attrition | Tendon transfer or reconstruction, Darrach if not done |
Infection Risk in RA Patients
RA patients are immunosuppressed from disease and medications (methotrexate, biologics, corticosteroids). Infection risk is 2-5 times higher than non-RA patients. Strategies to reduce infection:
- Stop methotrexate 2 weeks pre-op, restart 2 weeks post-op
- Hold biologics 1 dosing cycle before surgery
- Prophylactic antibiotics (first-generation cephalosporin)
- Meticulous sterile technique
- Monitor closely post-op for signs of infection
Postoperative Care and Rehabilitation
Post-MCP Arthroplasty Rehabilitation
- Splinting: Dynamic extension splint with outrigger
- MCP held in extension and radial deviation
- Passive ROM exercises initiated day 3-5
- Critical: Maintain radial pull to prevent recurrent ulnar drift
- Continue dynamic splint full-time
- Active ROM exercises 5x daily (remove splint)
- Blocking exercises to isolate MCP motion
- Scar massage and edema control
- Wean from splint (nighttime only)
- Progressive grip strengthening
- Functional activities (ADLs)
- Assess for recurrent drift, adjust therapy
- Resume normal activities
- Continue nighttime splint for 3-6 months
- Monitor for implant fracture, recurrent deformity
- Annual follow-up indefinitely
Splinting Compliance is Critical
Recurrent ulnar drift occurs in 10-15%, mostly from poor splinting compliance. The dynamic extension splint provides radial-directed force to counteract ulnar pull during healing. Patients must understand that splint wear for 6 weeks full-time, then nighttime for 6 months, is essential to prevent recurrence.
Outcomes and Prognosis
Functional Outcomes by Procedure
| Procedure | Pain Relief | Function | Satisfaction | Revision Rate |
|---|---|---|---|---|
| MCP arthroplasty | 80-90% significant improvement | ROM improved in 60%, reduced in 30% | 80% satisfied | 10-20% at 10 years (implant fracture) |
| PIP arthrodesis | 90% complete relief | Stable grip platform, no motion | 85% satisfied | 5-10% (nonunion, malunion) |
| Wrist synovectomy | 70% relief if done early (under 6 months synovitis) | Preserves ROM, prevents tendon rupture | 75% satisfied | 30% require repeat synovectomy at 5-10 years |
| Darrach (distal ulna excision) | 90% relief of ulnar-sided wrist pain | Forearm rotation improves | 80% satisfied | 10% instability/convergence requiring revision |
Predictors of Poor Outcome
Factors associated with worse surgical outcomes in RA hand:
- Active disease at time of surgery (defer until remission)
- Poor medical compliance (methotrexate, biologics)
- Smoking (impairs wound healing, increases nonunion)
- Advanced age with poor bone quality (implant failure, nonunion)
- Inadequate soft tissue rebalancing (recurrent deformity)
- Poor rehabilitation compliance (stiffness, recurrent drift)
Evidence Base and Key Trials
Silicone MCP Arthroplasty vs Medical Treatment (Landmark Prospective Trial)
- Multicentre prospective controlled cohort across 3 referral centres (USA and England), 70 surgical and 93 non-surgical patients with severe ulnar drift or extensor lag
- One-year data analysed for 45 surgical cases and 72 non-surgical controls
- Surgical group: significant improvement in overall Michigan Hand Outcomes Questionnaire (MHQ) score despite worse baseline function; non-surgical group unchanged
- Ulnar deviation and extensor lag improved significantly after silicone MCP arthroplasty (SMPA); non-surgical group did not improve
- Grip strength, pinch strength and Arthritis Impact Measurement Scales showed no significant change in either group
TICORA: Tight Control (Treat-to-Target) in Rheumatoid Arthritis
- Single-blind RCT in 111 patients: intensive monthly tight-control management vs routine outpatient care
- Mean fall in disease activity score (DAS) greater with tight control: -3.5 vs -1.9 (difference 1.6, 95% CI 1.1-2.1, p less than 0.0001)
- Good response achieved in 82% of intensive group vs 44% routine; remission (DAS less than 1.6) in 65% vs 16%
- Tight control substantially reduced radiographic disease progression and improved physical function and quality of life at no additional cost
Anti-CCP Antibodies: Landmark Diagnostic Validation
- Defining study introducing the cyclic citrullinated peptide (anti-CCP) ELISA
- Anti-CCP highly specific for RA: 98% in prevalent sera and 96% in an early-arthritis clinic cohort, with moderate sensitivity (sensitivity 48-68% depending on cohort)
- Anti-CCP significantly more specific than IgM rheumatoid factor (96% vs 91%, p = 0.016)
- Combining anti-CCP with IgM-RF raised positive predictive value to 91%
- Anti-CCP at first visit predicted erosive disease at 2 years (PPV 91%)
Silicone MCP Arthroplasty: 14-Year Durability
- 208 silicone MCP arthroplasties in 52 hands (36 patients), mean 14-year follow-up - single surgeon
- Ulnar drift improved from 26 degrees to under 5 degrees postoperatively but recurred to a mean of 16 degrees
- Extension deficit improved from 57 degrees to 11 degrees but worsened to 23 degrees at final follow-up
- 130 of 208 implants (63%) were fractured and a further 22% deformed; implant fracture correlated with recurrent ulnar drift (p less than 0.001)
- Mean MHQ score 48/100; patients were satisfied with only 38% of hands and only 27% were pain-free at final review
DRUJ Hemiresection-Interposition Arthroplasty: Long-Term Results
- 51 wrists (39 rheumatoid patients) treated with matched hemiresection-interposition arthroplasty and dorsal wrist synovectomy, mean 4.5-year follow-up
- Associated extensor tendon ruptures present in 31% of patients at surgery
- Complete relief of ulnar-sided wrist pain in 84% of wrists, partial relief in 14%
- Supination improved 73 to 81 degrees and pronation 68 to 74 degrees; grip strength improved from 6.1 to 11.5 kgf
The Rheumatoid Wrist: Principles of Surgical Management
- Authoritative JAAOS instructional review of the rheumatoid wrist
- DRUJ is usually affected first; managed with Darrach or Sauve-Kapandji depending on age and demand
- Ruptured extensor/flexor tendons are rarely amenable to direct repair - tendon transfer or grafting is required when the motored joint remains functional
- Partial (radiolunate/radioscapholunate) wrist fusion balances stability with retained midcarpal motion; total wrist fusion gives reliable pain relief at the cost of motion
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: MCP Ulnar Drift Assessment
"A 55-year-old woman with 8-year history of seropositive RA presents with progressive ulnar deviation of MCP joints in both hands. She is on methotrexate and adalimumab with good systemic disease control. Her ulnar deviation is approximately 30 degrees and partially correctable passively. What is your assessment and management?"
Scenario 2: Extensor Tendon Rupture (Vaughan-Jackson Lesion)
"A 60-year-old man with longstanding RA presents unable to extend his small and ring fingers at the MCP joint. Examination reveals prominent dorsal ulnar head and loss of EDM and EDC ring finger function. What is your assessment and surgical management?"
Scenario 3: Thumb Z-Deformity (Nalebuff Type III)
"A 50-year-old woman with RA has progressive thumb deformity with CMC joint subluxation, MCP hyperextension to 40 degrees, and compensatory IP flexion. She has weak pinch and difficulty with activities requiring precision grip. Describe your classification and surgical approach."
MCQ Practice Points
Ulnar Drift Mechanism Question
Q: What is the primary pathologic mechanism of MCP ulnar drift in rheumatoid arthritis? A: Radial collateral ligament destruction with ulnar subluxation of the extensor tendon. The radial collateral ligament fails from synovitis, allowing the extensor tendon to subluxate ulnarly. Intrinsic muscles then pull the fingers into progressive ulnar deviation, worsened with grip.
Vaughan-Jackson Lesion Question
Q: What is the typical sequence of extensor tendon rupture in Vaughan-Jackson lesion? A: EDM (extensor digiti minimi) ruptures first, followed by EDC ring, then EDC middle. The sequence progresses from ulnar to radial as tendons attrit on the prominent dorsal ulnar head (caput ulnae). EDM ruptures first because it is most ulnar and has the thinnest cross-section.
Boutonniere vs Swan-Neck Question
Q: What is the primary pathology distinguishing boutonniere from swan-neck deformity? A: Boutonniere: Central slip rupture/attenuation causes PIP flexion and DIP extension. Lateral bands migrate volar to PIP axis. Swan-neck: Volar plate laxity or FDS rupture causes PIP hyperextension and DIP flexion. Intrinsics pull PIP into hyperextension.
Anti-CCP Antibody Question
Q: What is the specificity of anti-CCP antibodies for rheumatoid arthritis diagnosis? A: 95% specificity for RA (compared to RF at 85%). Anti-CCP antibodies are highly predictive of erosive disease and indicate need for early aggressive DMARD therapy. Combination of RF + anti-CCP positive is 90% predictive of erosive RA.
Soft Tissue Rebalancing Question
Q: What is the most important soft tissue procedure to prevent recurrent ulnar drift after MCP arthroplasty? A: Ulnar intrinsic release combined with radial sagittal band tightening. Releasing the ulnar intrinsics removes the ulnar-deviating force, while tightening the radial sagittal band centralizes the extensor tendon over the MCP joint. Implant alone without soft tissue rebalancing has 30% recurrence rate.
Nalebuff Type III Question
Q: In Nalebuff Type III thumb deformity, what is the primary pathology and surgical target? A: CMC joint subluxation is the primary pathology (not MCP). The thumb metacarpal adducts and subluxates at CMC from ligamentous laxity. MCP hyperextension and IP flexion are compensatory to achieve pinch. Surgical treatment must address CMC stabilization first before correcting MCP deformity, otherwise recurrence is inevitable.
Guidelines, Registries & Global Practice
Global Epidemiology
Rheumatoid arthritis affects approximately 0.5-1% of adults worldwide, with a consistent female predominance of roughly 3:1 and peak onset between 40 and 60 years. Prevalence is highest in some Indigenous North American populations and lowest in parts of sub-Saharan Africa and East Asia, reflecting genetic (HLA-DRB1 shared epitope) and environmental (notably smoking) contributions. The hand is involved in the majority of patients over the disease course, and is the most common site requiring reconstructive surgery. Critically, the incidence of major rheumatoid hand surgery has fallen substantially in the biologic era, mirroring earlier diagnosis (2010 ACR/EULAR criteria) and treat-to-target medical control (TICORA).
Side-by-Side Guideline Guidance
Guideline and Body Comparison - RA Hand Management
| Body | Scope | Key Position | Evidence Basis |
|---|---|---|---|
| ACR/EULAR (2010 criteria; EULAR 2022 management update) | Diagnosis and medical treat-to-target | Classify and treat early; methotrexate first-line, escalate to biologic/targeted synthetic DMARD if target not met; short-term glucocorticoid bridging only | RCT and systematic review (Level 1) |
| NICE (NG100, UK) | Diagnosis, monitoring, referral | Refer suspected persistent synovitis urgently; treat-to-target with monthly review until target met; offer hand exercise and therapy | Guideline (Level 1-2 underpinning) |
| BSR / BOA (UK) | Perioperative DMARD management and hand surgery | Continue methotrexate through surgery; withhold biologics around surgery timed to dosing cycle; involve hand therapy | Guideline / consensus |
| Perioperative consensus (peri-op DMARD handling) | Surgical optimisation | Methotrexate may be continued perioperatively; biologics held one dosing interval and surgery scheduled at the trough; resume once wound healed and no infection | Consensus / cohort |
Perioperative DMARD Handling - Evolving Practice
Earlier teaching to stop methotrexate before surgery has been superseded: current ACR/EULAR-aligned perioperative guidance supports continuing methotrexate through hand surgery, as it does not increase infection or wound complications and avoids disease flare. Biologics are withheld for one dosing cycle and surgery booked at the trough, then resumed once the wound is healed and infection is excluded. Quote both the traditional and the current position in vivas and state the current evidence-based answer.
Registry and Outcome Evidence
Registry & Population Data
- Falling surgical burden: National cohort and registry data across Scandinavia, the UK and the USA show declining rates of rheumatoid hand and wrist surgery since widespread biologic use
- Implant durability: Long-term series (Goldfarb and Stern) document ~63% silicone MCP implant fracture at 14 years - durability, not early failure, is the key issue
- Treat-to-target benefit: TICORA-type strategies reduce radiographic progression and downstream reconstruction
Practice Variation
- DRUJ procedure choice varies: Darrach (older/lower demand) vs Sauve-Kapandji or hemiresection (younger, motion-preserving)
- Implant vs fusion decisions for MCP/PIP differ by surgeon and region
- Access: biologic availability and elective hand-surgery waiting times differ markedly between health systems, shifting the surgical/medical balance
- Australia: DMARDs and biologics are subsidised via the PBS (biologics under rheumatologist authority); eTG informs surgical antibiotic prophylaxis and Quitline (13 7848) supports peri-operative smoking cessation
Glucocorticoids in RA - Evidence Informing the 2022 EULAR Update
- Systematic literature review underpinning the 2022 EULAR RA management recommendations
- Confirmed efficacy of short-term glucocorticoid bridging; most patients can stop within 12-24 months
- Dose- and duration-dependent harms confirmed: osteoporotic fracture, serious infection, diabetes and increased mortality
- Supports using the lowest effective steroid dose for the shortest time as a bridge while DMARDs take effect
RHEUMATOID ARTHRITIS - HAND
Clinical summary
Key Pathophysiology
- •Synovial inflammation (pannus) invades cartilage and bone causing progressive destruction
- •Ulnar drift = radial collateral ligament destruction + ulnar extensor subluxation + intrinsic contracture
- •Boutonniere = central slip rupture, PIP flexion, DIP extension (lateral bands volar to PIP axis)
- •Swan-neck = volar plate laxity or FDS rupture, PIP hyperextension, DIP flexion
- •Vaughan-Jackson = EDM, EDC ring, EDC middle sequential rupture from caput ulnae attrition
Classification
- •Nalebuff Thumb Type I = boutonniere (MCP flexion, IP extension) = MCP synovitis
- •Type II = swan-neck (MCP hyperext, IP flex) = MCP ligament laxity
- •Type III = swan-neck from CMC subluxation (treat CMC first!)
- •Boutonniere deformity staging: Stage I (under 30° lag, correctable), Stage II (30-50°), Stage III (over 50°, fixed)
Medical Management
- •DMARDs within 2 years critical - window of opportunity to prevent erosions
- •Anti-CCP 95% specific for RA, predicts erosive disease
- •Methotrexate gold standard, add biologic if inadequate response at 3 months
- •Pre-op: stop MTX 2 weeks before, biologics 1 dosing cycle, continue corticosteroids
Surgical Pearls
- •Proximal-to-distal surgery sequence - correct wrist before MCP, MCP before PIP
- •MCP arthroplasty requires soft tissue rebalancing: ulnar intrinsic release + radial sagittal band reef
- •Darrach (distal ulna excision) for caput ulnae prevents further extensor ruptures
- •Dynamic extension splint for 6 weeks post-MCP arthroplasty prevents recurrent drift
- •Synovectomy only effective if done under 6 months of synovitis onset
Complications
- •Infection 2-5% (immunosuppression from RA medications)
- •MCP implant fracture 10-20% at 10 years (mostly asymptomatic)
- •Recurrent ulnar drift 10-15% (inadequate soft tissue balancing or poor splinting compliance)
- •Stiffness 20-30% (ROM may worsen but pain improves)
- •Arthrodesis nonunion 5-10% (smoking, corticosteroids, poor bone quality)