Synovitis-Driven Deformity | Tendon Rupture | Surgical Sequencing
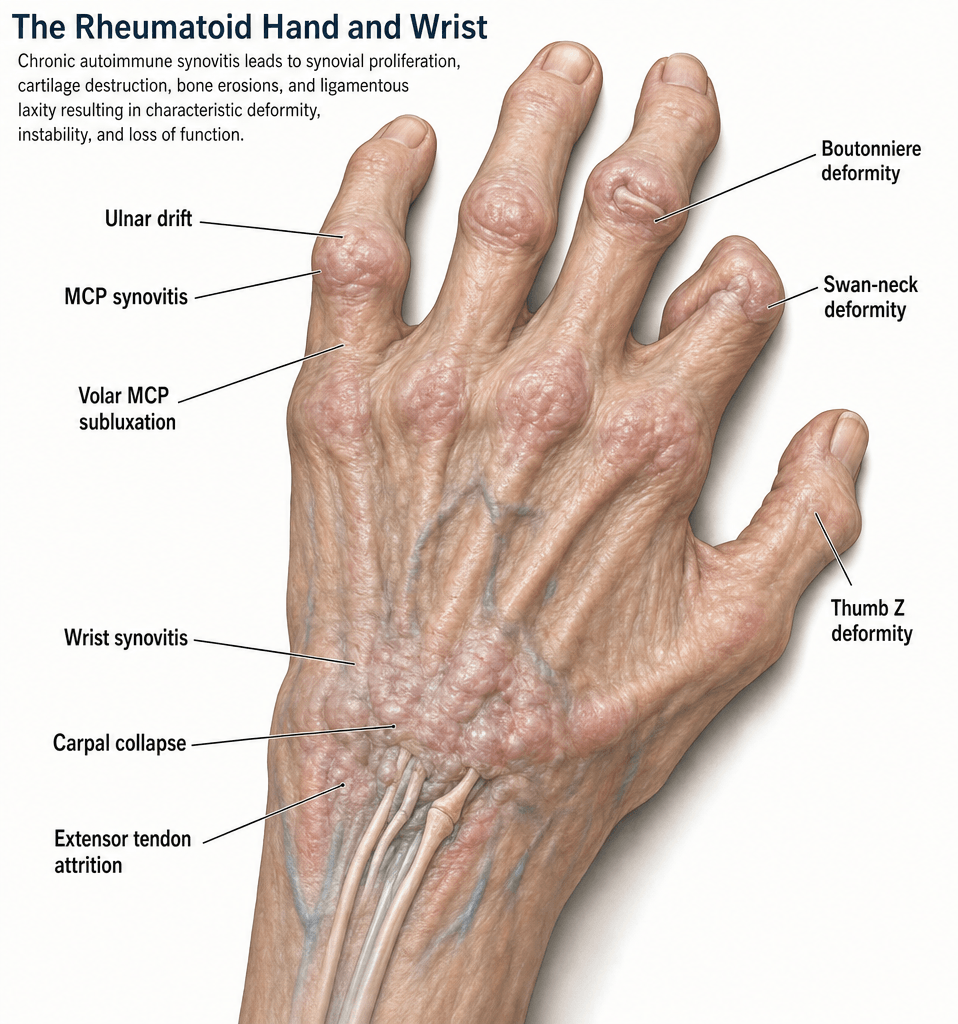
- RA synovitis destroys ligaments, tendons and cartilage producing characteristic zig-zag deformities
- Caput ulnae = dorsal DRUJ subluxation; attrition ruptures extensor tendons (Vaughan-Jackson, Mannerfelt)
- Nalebuff classification guides thumb reconstruction: Type I (MCP), Type II (MCP+CMC), Type III (CMC), Type IV (IP)
- Surgical sequence = DIP/PIP first, then MCP, then wrist, then elbow/shoulder (distal-to-proximal)
- Medical optimisation with DMARDs is prerequisite before elective surgical intervention
- “Vaughan-Jackson = EDM rupture from attrition over caput ulnae
- “Mannerfelt-Norman = FPL rupture over scaphoid osteophyte
- “Ulnar drift worsened by radial deviation of wrist (zig-zag collapse)
- “Surgical sequence is distal-to-proximal; wrist before MCP if both needed
Synovial hypertrophy destroys stabilising ligaments and tendons. Pannus erodes articular cartilage and bone. The resulting imbalance produces the classic deformities. Medical control of synovitis is the foundation of management.
Dorsal subluxation of the ulnar head at the DRUJ. Creates a sharp bony prominence that attritions extensor tendons, especially EDM and EDC to small and ring fingers (Vaughan-Jackson sequence). Caput ulnae sign = prominent ulnar head visible and palpable dorsally.
Vaughan-Jackson: Extensor ruptures from ulnar to radial (EDM, then EDC small, ring, middle) due to attrition over caput ulnae. Mannerfelt-Norman: FPL rupture from attrition over a scaphoid osteophyte or rough bone in the carpal tunnel.
Distal-to-proximal rule: Address DIP/PIP deformities first, then MCP joints, then wrist. Exception: significant wrist disease drives MCP deformity and should be stabilised before or concurrently with MCP surgery. Proximal procedures (elbow, shoulder) are performed last.
- Pathoanatomy
- Synovitis destroys collateral ligaments and dorsal capsule; extensor tendons slip ulnarly
- Non-operative
- DMARDs, MCP splinting, intrinsic stretching
- Surgical Options
- Synovectomy, crossed intrinsic transfer, silicone arthroplasty
- Pathoanatomy
- PIP hyperextension from FDS rupture, volar plate attenuation, or intrinsic tightness
- Non-operative
- PIP extension-block splint, exercise
- Surgical Options
- FDS tenodesis, lateral band relocation, PIP arthrodesis
- Pathoanatomy
- Central slip attenuation from synovitis, lateral bands migrate volar
- Non-operative
- PIP extension splint, DMARDs
- Surgical Options
- Central slip reconstruction, PIP arthrodesis
- Pathoanatomy
- Attrition over caput ulnae (Vaughan-Jackson) or scaphoid (Mannerfelt)
- Non-operative
- DMARDs, wrist splint to reduce attrition
- Surgical Options
- Tendon transfer (EIP to EDM, side-to-side), Darrach/sauve-kapandji
DRIFTRheumatoid Hand Deformity Sequence
Hook:DRIFT describes the cascade from synovitis to deformity: treat the inflammation first!
DISTALSurgical Sequencing Rule
Hook:DISTAL = the surgical sequence goes from fingers back toward the shoulder!
EXTRAVaughan-Jackson Attrition Ruptures
Hook:EXTRA tendons rupture from EXTRA bone - smooth the ulnar head before any tendon transfer!
Overview and Epidemiology

Rheumatoid arthritis affects the hand and wrist in approximately 90 percent of patients, making it the most commonly involved region. The hand deformities are the visible hallmark of RA and are a high-yield exam topic. Understanding the pathomechanics of each deformity, the eponymous tendon rupture patterns, and the correct sequence of surgical reconstruction is essential for fellowship-level knowledge.
- Prevalence: RA affects approximately 0.5-1 percent of the global population
- Hand involvement: Up to 90 percent of RA patients develop hand/wrist manifestations
- Female-to-male ratio: 3:1
- Peak onset: 30-50 years, though all ages affected
- Bilateral and symmetrical: Characteristic distribution pattern
- Grip strength: Reduced by up to 70 percent in advanced disease
- Pinch weakness: Especially key pinch (thumb involvement)
- ADL limitation: Buttoning, writing, opening jars affected early
- Deformity progression: Predictable pattern from synovitis to ligament destruction to joint subluxation
Pathophysiology
Rheumatoid synovitis produces hypertrophied pannus tissue that invades and destroys periarticular structures through enzymatic digestion and mechanical pressure. In the hand and wrist, this process targets:
- Joint capsules and ligaments: Leading to instability, subluxation, and ulnar drift
- Extensor tendons: Attrition ruptures over bony prominences (caput ulnae, scaphoid)
- Flexor tendons: Especially FPL in the carpal tunnel (Mannerfelt lesion)
- Articular cartilage and bone: Marginal erosions, cartilage loss, osteopenia
- Intrinsic muscles: Fibrosis and contracture drive swan-neck deformity and contribute to MCP subluxation The resultant imbalance between flexors and extensors produces the classic zig-zag deformity patterns.
- Primary Structure Damaged
- Dorsal capsule, collateral ligaments, volar plate
- Mechanism
- Synovitis stretches dorsal capsule; flexor tendons pull proximal phalanx volarly
- Resulting Posture
- Proximal phalanx subluxes volarly on metacarpal head
- Primary Structure Damaged
- Radial collateral ligament, radial sagittal band
- Mechanism
- Radial-sided structures attenuate; intrinsic muscles pull ulnarly; extensor tendons slip ulnar to MCP axis
- Resulting Posture
- Fingers deviate ulnarly at MCP joints
- Primary Structure Damaged
- Volar plate, FDS insertion, intrinsic muscles
- Mechanism
- Volar plate laxity + intrinsic tightness + FDS rupture/attenuation allows PIP hyperextension
- Resulting Posture
- PIP hyperextension + DIP flexion
- Primary Structure Damaged
- Central slip (extensor mechanism)
- Mechanism
- Synovitis at PIP attenuates central slip; lateral bands migrate volar
- Resulting Posture
- PIP flexion + DIP hyperextension
- Primary Structure Damaged
- DRUJ capsule, TFCC, ECU tendon sheath
- Mechanism
- DRUJ synovitis leads to dorsal ulnar head subluxation and supination of carpus
- Resulting Posture
- Prominent dorsally subluxed ulnar head
Wrist radial deviation drives MCP ulnar deviation (zig-zag collapse). When the carpus supinates and deviates radially due to RA destruction, the metacarpals point more ulnarly. This biomechanical linkage means wrist position governs MCP alignment. Correcting wrist alignment is critical before or during MCP surgery.
The DRUJ and ulnar-sided wrist structures are the first to be affected in RA because:
- Ulnar styloid and head have thin overlying soft tissue
- ECU tendon sheath is a common site of early synovitis
- The TFCC is vulnerable to pannus invasion
- Extensor tendons (especially EDM) lie directly over the subluxing ulnar head
Classification and Types
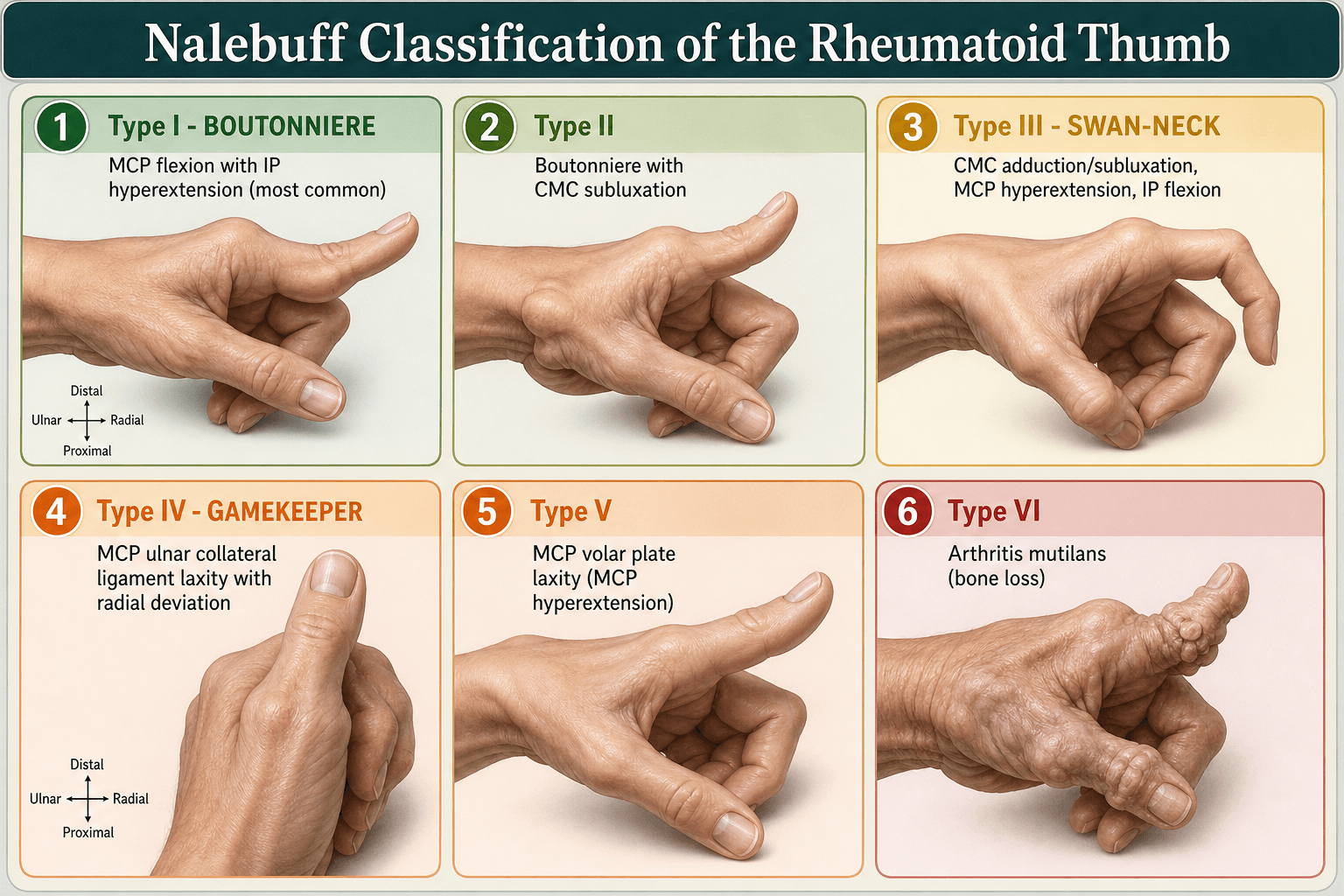
Nalebuff Classification of RA Thumb Deformity
- Joint Affected
- MCP joint
- Pathoanatomy
- MCP synovitis stretches dorsal capsule and collateral ligaments; IP hyperextends to compensate
- Deformity
- MCP flexion + IP hyperextension (boutonniere-type)
- Surgical Treatment
- MCP arthrodesis or synovectomy + extensor reconstruction
- Joint Affected
- MCP + CMC
- Pathoanatomy
- Combined MCP boutonniere and CMC subluxation
- Deformity
- MCP flexion + CMC dorsal subluxation + IP hyperextension
- Surgical Treatment
- CMC arthroplasty + MCP arthrodesis
- Joint Affected
- CMC joint
- Pathoanatomy
- CMC synovitis leads to dorsal subluxation; MCP hyperextends and adducts (swan-neck type)
- Deformity
- CMC subluxation + MCP hyperextension + IP flexion
- Surgical Treatment
- CMC arthroplasty or arthrodesis + MCP flexion release
- Joint Affected
- IP joint
- Pathoanatomy
- IP joint destruction from synovitis; rare isolated pattern
- Deformity
- IP joint destruction, often fibrous or bony ankylosis
- Surgical Treatment
- IP arthrodesis
The Nalebuff classification is the most commonly examined system for RA thumb deformity. Type I is by far the most common. Key principle: the thumb is classified by which joint is the primary site of destruction, which then dictates the surgical plan.
The table above covers the four common patterns, but the full Nalebuff classification runs to six types, and the two additional ones are easy marks if an examiner pushes beyond Type IV:
- Type V - MCP volar plate laxity (MCP hyperextension): an isolated MCP hyperextension deformity caused by attenuation of the MCP volar plate, without the primary CMC disease that defines Type III. The IP joint compensates by flexing. Treatment is to restore the volar checkrein - MCP volar plate capsulodesis or sesamoid arthrodesis (or MCP arthrodesis if the joint is destroyed) - rather than addressing the CMC.
- Type VI - arthritis mutilans (skeletal collapse): gross bone loss and resorption ("opera-glass hand"/main en lorgnette) producing a flail, telescoping, grossly shortened thumb ray. This is the end-stage destructive pattern and usually needs bony reconstruction with bone graft and arthrodesis to restore length and a stable post for pinch.
Exam point: distinguish Type III (CMC-driven swan-neck with MCP hyperextension secondary to CMC collapse and adduction) from Type V (primary MCP volar plate laxity with a normal CMC) - the discriminator is whether the CMC joint is the driver, because it changes the operation (CMC arthroplasty for III vs MCP-level stabilisation for V).
Clinical Assessment
- Disease duration and treatment: DMARDs, biologics, steroid history
- Hand function: Grip, pinch, ADLs (buttoning, key turning, writing)
- Deformity progression: Rate of change, which fingers affected first
- Pain: Localise to specific joints (wrist, MCP, PIP)
- Tendon function: Sudden loss of extension (rupture), triggering
- Inspect: Zig-zag deformity pattern, MCP ulnar drift, wrist supination, thumb posture
- Palpate: Synovitis (boggy swelling), caput ulnae, tendon fraying (crepitus)
- Active ROM: Finger extension (test each tendon individually), flexion cascade
- Tendon integrity: Test EDM independently (extend small finger while holding others flexed)
- Passive correctability: Can MCP joints be reduced? PIP deformity flexible or fixed?
Caput ulnae sign: Prominent ulnar head palpable dorsally, especially with forearm pronation. The "piano key" test demonstrates dorsal subluxation: press the ulnar head - it depresses like a piano key and rebounds when released.
Extensor tendon assessment in RA:
- Test each finger's active extension independently
- EDM rupture: Inability to extend small finger independently (Vaughan-Jackson)
- EDC rupture cascade: Progressive loss of extension from ulnar to radial digits
- FPL rupture (Mannerfelt): Loss of thumb IP flexion against resistance
- Sudden loss of extension is a rupture until proven otherwise - do not attribute to disease flare without ultrasound or MRI confirmation
- Tendon(s) Involved
- EDM first, then EDC (small, ring, middle sequentially)
- Mechanism
- Attrition over dorsally subluxed ulnar head
- Site of Attrition
- Dorsal DRUJ (caput ulnae)
- Reconstruction
- EIP transfer to EDM; side-to-side for EDC; address ulnar head
- Tendon(s) Involved
- Flexor pollicis longus (FPL)
- Mechanism
- Attrition over scaphoid osteophyte or rough bone in carpal tunnel
- Site of Attrition
- Volar wrist / carpal tunnel (scaphoid ridge)
- Reconstruction
- FDS ring finger transfer to distal FPL; carpal tunnel release
- Tendon(s) Involved
- ECU rupture or subluxation
- Mechanism
- Synovitis of ECU sheath, tendon attenuation
- Site of Attrition
- Dorsal ulnar wrist
- Reconstruction
- ECU reconstruction or transfer; stabilise DRUJ
FPL rupture in RA is often painless and may present as an incidental finding. The patient reports inability to flex the thumb IP joint. Unlike extensor ruptures, this is a flexor-side attrition in the carpal tunnel. Always examine FPL function in RA patients - loss of thumb IP flexion against resistance is diagnostic. Carpal tunnel release alone may prevent further ruptures if caught early.
"This rheumatoid patient cannot extend their fingers - why?" is a classic examiner trap, because the answer is not automatically tendon rupture. There are three distinct causes, and they are managed completely differently:
- True extensor tendon rupture (attrition - Vaughan-Jackson): the tendon is discontinuous. Test with the tenodesis effect - passive wrist flexion should produce passive finger extension; if the finger stays flexed (no tenodesis), the tendon is ruptured. The patient can neither initiate nor hold extension.
- Extensor tendon subluxation off the MCP head (sagittal band attenuation): the tendon is intact but has slipped ulnarly into the intermetacarpal valley, so it can no longer extend the MCP from a flexed position. The giveaway is that if you passively extend the finger, the patient can HOLD it extended (the relocated tendon works), but cannot initiate extension from flexion. Tenodesis is intact. This needs sagittal-band reconstruction/extensor re-centralisation, not a tendon transfer.
- Posterior interosseous nerve (PIN) palsy: radiocapitellar/elbow synovitis or a proximal forearm lesion denervates the digital extensors. Multiple fingers and thumb lose extension with an intact tenodesis effect and (often) preserved wrist extension in radial deviation (ECRL spared). Examine the elbow and check for a PIN cause before assuming the problem is at the wrist.
Exam point: the tenodesis test plus the "can hold but cannot initiate" sign separate these three at the bedside - rupture (no hold, no tenodesis), subluxation (can hold, tenodesis intact), PIN palsy (multiple digits, tenodesis intact, look proximally). Operating as if it were a rupture when it is a subluxation or a PIN palsy is a recognised error.
Investigations
Imaging Protocol
Views: PA, lateral, oblique of both hands and wrists; Norgard (ball-catcher) view for early erosions
Look for: Periarticular osteopenia, joint space narrowing, marginal erosions, carpal collapse, ulnar translocation, scapholunate dissociation, MCP volar subluxation, ulnar drift
Larsen grading: Standardised scoring system for RA radiographic progression
Ultrasound: Dynamic assessment of tendon integrity, synovitis (power Doppler), tenosynovitis
MRI: Gold standard for early erosions, pannus, bone marrow oedema; assesses tendon quality
Key finding: Tendon discontinuity, surrounding synovitis, bony spurs causing attrition
Indication: Assess bone stock for arthroplasty or arthrodesis, carpal bone erosion severity
Helpful for: Planning wrist arthrodesis fixation, evaluating distal radius and ulnar head architecture
The Norgard (ball-catcher) view is the most sensitive plain radiograph for early RA erosions in the hands. It profiles the MCP joints and wrist in slight oblique and ulnar-deviated position, revealing erosions that may be missed on standard PA views. Always request bilateral hand and wrist radiographs for comparison and to document the symmetrical pattern typical of RA.
Management Algorithm
Medical Optimisation (Prerequisite to Surgery)
DMARD Therapy Timeline
Methotrexate: First-line conventional synthetic DMARD (csDMARD) Adjuncts: Hydroxychloroquine, sulfasalazine, leflunomide (combination therapy common) Bridging: Short-term low-dose prednisone while awaiting DMARD effect (6-12 weeks)
Biologic DMARDs (bDMARDs): TNF inhibitors (adalimumab, etanercept), IL-6 inhibitors (tocilizumab), B-cell therapy (rituximab) JAK inhibitors: Tofacitinib, baricitinib, upadacitinib (targeted synthetic DMARDs) Treat-to-target: Aim for remission or low disease activity
Methotrexate: Generally continue through surgery (evidence supports safety) Biologics: Withhold 2-5 half-lives before surgery; restart once wound healed (usually 2 weeks) Prednisone: Stress dose coverage if on chronic steroids Coordinate with rheumatology: Perioperative DMARD management is a joint decision
The rheumatologist and hand surgeon must work as a team. Surgery on an actively inflamed joint has higher complication rates. The general principle is: optimise medical management first, then operate on the structural consequences. Exceptions include acute tendon ruptures (urgent surgery to prevent further attrition) and severe nerve compression.
Complications
- Incidence / Risk
- Common in poorly controlled disease
- Risk Factors
- Inadequate DMARD therapy, poor soft tissue quality
- Management
- Optimise medical management, revision surgery if functional
- Incidence / Risk
- 10-30 percent at 10 years
- Risk Factors
- High demand, poor bone stock, inadequate soft tissue balance
- Management
- Often asymptomatic; revision if painful or deformity recurs
- Incidence / Risk
- Reported in 10-25 percent long-term
- Risk Factors
- Aggressive distal ulnar resection, insufficient ligament repair
- Management
- Sauve-Kapandji preferred if possible; partial repair if identified
- Incidence / Risk
- 5-15 percent
- Risk Factors
- Persistent bony spurs, ongoing synovitis
- Management
- Ensure attrition source addressed at index surgery
- Incidence / Risk
- Higher than non-RA population
- Risk Factors
- Chronic steroids, poor nutrition, vasculitis
- Management
- Pre-operative skin assessment; steroid management; meticulous technique
- Incidence / Risk
- Elevated with DMARDs / biologics
- Risk Factors
- Immunosuppression, steroids, poor glycaemic control
- Management
- Perioperative antibiotic; withhold biologics; coordinate with rheumatology
The key to preventing complications in RA hand surgery is:
- Medical optimisation: Control synovitis before elective surgery
- Meticulous soft tissue handling: RA tissues are fragile and prone to failure
- Address the underlying cause: Remove bony attrition sources, tenosynovectomy
- Realistic expectations: RA surgery improves function and reduces pain but rarely restores normal hand mechanics
- Coordinate perioperative DMARD management with rheumatology to balance infection risk against flare
Outcomes and Prognosis
- Pain Relief
- Over 90 percent good-excellent pain relief
- Functional Outcome
- Stable platform for hand function; improved grip
- Survival / Durability
- Fusion rate over 95 percent; durable long-term
- Pain Relief
- Good pain relief in 80-90 percent
- Functional Outcome
- Improved alignment and appearance; modest grip improvement
- Survival / Durability
- 10-year implant survival approximately 70-80 percent
- Pain Relief
- Reliable restoration of small finger extension
- Functional Outcome
- Depends on quality of donor and recipient tissue
- Survival / Durability
- Good durability if ulnar head addressed
- Pain Relief
- Good relief of DRUJ pain
- Functional Outcome
- Improved forearm rotation, eliminates attrition
- Survival / Durability
- Risk of ulnar translocation long-term (10-25 percent)
- Pain Relief
- Excellent pain relief
- Functional Outcome
- Reliable pinch restoration, stable thumb column
- Survival / Durability
- High fusion rate, durable
Best outcomes: Well-controlled disease (DMARDs), early intervention before fixed deformity, good bone stock, patient compliance with therapy, non-smoker
Poor outcomes: Active synovitis at time of surgery, steroid dependence, multiple previous surgeries, poor bone quality, vasculitis
Key message: RA hand surgery is reconstructive, not curative. The goal is pain relief, improved function, and prevention of further deformity. Patients who understand this have better satisfaction.
Guidelines, Registries & Global Practice
- RA prevalence: 0.5-1 percent worldwide; higher in Northern European and North American populations
- Hand involvement: The most common site of RA manifestation across all ethnicities
- Declining surgery rates: Biologic DMARDs have dramatically reduced the need for reconstructive RA hand surgery in well-resourced settings
- Delayed presentation: In resource-limited settings, patients often present with established deformities
- High-resource: Early biologic therapy, hand therapy teams, silicone arthroplasty, total wrist arthroplasty as an option
- Limited-resource: Conventional DMARDs, arthrodesis preferred over arthroplasty (no implant costs, no need for long-term follow-up of implants)
- Universal principle: Tendon attrition must be addressed surgically regardless of resource setting - delay leads to further ruptures
- Surgical training: RA hand reconstruction is increasingly concentrated in specialist centres as caseloads decline
- Medical Management Emphasis
- Treat-to-target with DMARDs; biologics for inadequate response at 6 months
- Surgical Indications
- Surgery for structural damage unresponsive to medical therapy; urgent for tendon rupture
- Implant Preference
- Silicone MCP arthroplasty well-established; wrist arthrodesis preferred over arthroplasty
- Medical Management Emphasis
- Methotrexate first-line; early biologic escalation; JAK inhibitors as option
- Surgical Indications
- Functional impairment and pain despite optimal medical therapy
- Implant Preference
- Silicone MCP arthroplasty; wrist arthroplasty gaining acceptance in select patients
- Medical Management Emphasis
- Treat-to-target within 6 months; combination csDMARDs before biologics
- Surgical Indications
- Multidisciplinary decision; surgery for irreversible structural damage
- Implant Preference
- No specific implant guidance; arthrodesis vs arthroplasty by surgeon preference
- Medical Management Emphasis
- Coordinate perioperative DMARD management with rheumatology
- Surgical Indications
- Tendon rupture is semi-urgent; electives when disease quiescent
- Implant Preference
- Silicone MCP standard; pyrolytic carbon an alternative in some centres
Joint replacement registries (NJR UK, AOANJRR Australia, AJRR US) now track wrist and small joint arthroplasty. Data consistently show that silicone MCP implants have 10-year survival of approximately 70-80 percent, with fracture being the primary mode of failure. Total wrist arthrodesis remains the benchmark against which wrist arthroplasty is measured. The overall volume of RA hand surgery has declined dramatically in countries with early biologic access, making surgical training and maintenance of expertise an ongoing concern.
Coordinate with rheumatology for every RA surgical case:
- Continue: Methotrexate through surgery (evidence supports safety)
- Withhold biologics: 2-5 half-lives pre-operatively; restart 2 weeks post-op if wound healed
- Prednisone: Stress dose coverage for patients on chronic steroids
- JAK inhibitors: Withhold 3-7 days before surgery (short half-life)
- Postpone elective surgery if active infection or poorly controlled disease
- Document: DMARD plan in the operation note and communicate to the anaesthetic team
Controversies & Areas of Uncertainty
The Darrach procedure removes the attrition source but risks ulnar translocation of the carpus over time (10-25 percent). Sauve-Kapandji preserves the ulnar buttress but creates a pseudarthrosis that can be unstable. Choice depends on bone quality, DRUJ congruency, and surgeon preference. No high-quality RCTs compare the two.
Total wrist arthrodesis is reliable and durable but sacrifices all motion. Total wrist arthroplasty preserves some flexion-extension but has higher revision rates and is unsuitable for high-demand patients. In RA (low demand, bilateral disease), arthroplasty is increasingly considered for the non-dominant side while fusing the dominant wrist.
Silicone (Swanson) implants have long track records but fracture over time and may cause particulate synovitis. Pyrolytic carbon implants aim for more anatomical reconstruction but have limited long-term data in RA. Most surgeons still use silicone for RA MCP arthroplasty due to familiarity and published outcomes.
With effective biologic DMARDs, the need for RA hand surgery has declined markedly in well-resourced settings. This creates a training challenge: fewer cases mean fewer surgeons gaining expertise. The paradox is that when surgery is needed, it is often more complex (revision-type scenarios) and requires subspecialist skills.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old woman with long-standing seropositive RA presents with sudden inability to extend her small and ring fingers of the right hand over the past 2 weeks. She reports no pain. On examination, she has a prominent dorsally subluxed ulnar head, active extension of index and middle fingers is preserved, but she cannot actively extend the small and ring fingers. Passive extension is full. Wrist radiographs show advanced RA changes with dorsal subluxation of the ulnar head and carpal collapse. What is the diagnosis and management?”
“A 52-year-old woman with seropositive RA presents with bilateral hand deformities. The right hand shows: fixed MCP volar subluxation of all four fingers with 30 degrees ulnar drift, extensor tendon rupture of the small finger, caput ulnae with carpal collapse, and a Type I Nalebuff thumb deformity. Her disease is well-controlled on methotrexate and adalimumab. She requests surgical reconstruction. Describe your surgical plan and the order of procedures.”
Pathomechanics
- Synovial pannus destroys ligaments, tendons, and cartilage producing zig-zag deformities
- Caput ulnae = dorsal DRUJ subluxation; causes attrition ruptures of extensors
- Wrist radial deviation drives MCP ulnar drift (zig-zag collapse concept)
- Ulnar-sided structures fail first (ECU sheath synovitis, DRUJ, EDM attrition)
Key Deformities
- MCP: volar subluxation + ulnar drift from ligament destruction and flexor pull
- Swan-neck: PIP hyperextension + DIP flexion (intrinsic tightness, volar plate laxity, FDS rupture)
- Boutonniere: PIP flexion + DIP hyperextension (central slip attenuation, lateral bands volar)
- Thumb: Nalebuff Type I (MCP boutonniere) most common; Type III (CMC swan-neck) second
Tendon Ruptures
- Vaughan-Jackson: EDM then EDC small, ring, middle - ulnar to radial attrition over caput ulnae
- Mannerfelt-Norman: FPL rupture from attrition over scaphoid osteophyte in carpal tunnel
- Treatment principle: address the bone causing attrition before or during tendon transfer
- EIP is workhorse donor for EDM; FDS ring finger for FPL reconstruction
Surgical Sequence
- Distal-to-proximal rule: DIP/PIP first, then MCP, then wrist, then elbow/shoulder
- Exception: stabilise wrist before or with MCP surgery (wrist drives MCP position)
- Combine procedures using same approach when possible (dorsal wrist + extensor repair)
- Medical optimisation (DMARDs) is prerequisite before elective surgery
Key Procedures
- Total wrist arthrodesis: gold standard for end-stage RA wrist (fusion in 10-20 degrees extension)
- Darrach: distal ulnar excision for caput ulnae; Sauve-Kapandji preserves ulnar buttress
- Silicone MCP arthroplasty: for fixed MCP subluxation; 10-year survival approximately 70-80 percent
- Thumb MCP arthrodesis: for Nalebuff Type I (most common thumb deformity)
Perioperative Management
- Continue methotrexate through surgery (evidence supports safety)
- Withhold biologics 2-5 half-lives pre-operatively; restart at 2 weeks post-op
- Stress dose steroids for patients on chronic prednisone
- Sudden painless loss of extension = rupture until proven otherwise (do not wait)
Evidence Base and Key Trials
Rupture of extensor tendons by attrition at the inferior radio-ulnar joint: report of two cases
- Original description of sequential extensor tendon rupture by attrition at the distal radio-ulnar joint in rheumatoid disease
- Rupture begins with extensor digiti minimi (EDM) due to attrition over the dorsally subluxed ulnar head (caput ulnae)
- Progresses radially: EDM, then extensor digitorum communis to small, ring, and middle fingers in sequence
- Identified dorsal subluxation of the ulnar head as the mechanical cause of attrition
Scaphoid exostosis causing rupture of the flexor pollicis longus
- Describes attrition rupture of flexor pollicis longus over a scaphoid exostosis (osteophyte) within the carpal tunnel in rheumatoid disease
- Mechanism parallels the Mannerfelt-Norman lesion: rough bone on the volar scaphoid ridge abrades the FPL during flexion
- Often associated with carpal tunnel syndrome, requiring concurrent release and spur excision
- FPL reconstruction by tendon transfer or graft can restore thumb IP flexion
Metacarpophalangeal joint arthroplasty in rheumatoid arthritis: a long-term assessment
- Retrospective review of Swanson silicone MCP arthroplasty in rheumatoid patients with mean follow-up over 10 years
- Significant improvement in pain scores and MCP joint alignment persisted at long-term review
- Implant fracture rate approximately 10-30 percent at long-term follow-up
- Many fractured implants remained asymptomatic and functionally acceptable
Arthrodesis of the wrist for rheumatoid arthritis
- Total wrist arthrodesis via intramedullary pin fixation combined with iliac crest bone graft provided reliable pain relief in rheumatoid arthritis
- Stable fusion provided a platform that improved hand function distally and enabled subsequent MCP and tendon reconstruction
- Position of fusion (slight extension, neutral deviation) was critical for optimal grip strength and key pinch
- Established wrist arthrodesis as a durable surgical option for end-stage RA wrist disease
Boutonniere rheumatoid thumb deformity
- Describes Nalebuff Type I boutonniere rheumatoid thumb deformity: MCP flexion with IP hyperextension
- MCP joint is the primary site of deformity, requiring MCP stabilisation (arthrodesis preferred) for a stable thumb column
- Soft-tissue rebalancing alone is rarely sufficient; bony stabilisation at MCP is the workhorse
- Pain relief, restored pinch, and durable correction with MCP arthrodesis in appropriate patients