Russell-Taylor Classification of Subtrochanteric Fractures
- Letting the lesser trochanter decide I vs II. The piriformis fossa decides Type I vs II (the entry point); the lesser trochanter decides A vs B (the medial buttress). A fracture with the lesser trochanter detached but an intact fossa is a Type IB, NOT a Type II.
- Reaming a standard piriformis-entry nail through a fractured fossa (Type II). This drives the proximal fragment into varus/extension — the original rationale for avoiding a piriformis-entry nail in Type II.
- Ignoring the medial column in B subtypes. Loss of the lesser trochanter/calcar removes the medial buttress; nailing into residual varus without medial support invites varus collapse and implant failure.
- Claiming the nail is proven superior. Higher-level evidence (Starr; Lee) shows NO outcome difference between entry portals or between recon nail and plate — say outcomes are comparable and reduction quality matters most.
- Forgetting reduction quality. Subtrochanteric malreduction (varus, flexed proximal fragment) drives nonunion regardless of implant — an out-of-varus, biological reduction is the priority.
Anatomical basis — piriformis fossa & lesser trochanter
The piriformis fossa sits at the junction of the femoral neck and intertrochanteric region, medial to the tip of the greater trochanter — the classic antegrade nail entry for the adult femur. When the fracture extends through it (Type II), the proximal fragment is a separate piece with no intact bony bridge to the shaft, and reaming through the fossa can widen the gap and separate it further.
The lesser trochanter is the iliopsoas insertion and an important medial cortical buttress (with the calcar femorale). When it stays attached to the proximal fragment (subtype A) the medial column retains support; when it is fractured away (subtype B) the proximal fragment loses its medial column and is at high risk of varus collapse under weight-bearing.
In Type IB fractures the piriformis fossa entry survives but the medial cortex is stripped of the lesser trochanter. A cephalomedullary nail still works, but supplement the medial column (cerclage cables, medial buttress) or restore medial contact at reduction — nailing into residual varus with an unsupported medial defect invites early implant failure.
The classic subtrochanteric viva is "why is this fracture so hard to reduce and so prone to nonunion?" — and the answer is muscle pull plus mechanical load:
- The proximal fragment is pulled into a predictable deformity — flexion (iliopsoas on the lesser trochanter), abduction (gluteus medius and minimus on the greater trochanter) and external rotation (the short external rotators and iliopsoas). The distal fragment is adducted and shortened (the adductors) and pulled proximally. The net result is an apex-anterolateral / varus deformity that a simple traction nail will not correct on its own.
- Reduction must actively counter this — you bring the shaft out to the flexed-abducted proximal fragment (a lateral and slightly anterior start point, a percutaneous reduction clamp, a ball-spike or blocking screws, sometimes a mini-open reduction), and the single biggest determinant of union is finishing out of varus and out of flexion.
- The subtrochanteric region is a high-stress zone — it carries the largest compressive stress medially and tensile stress laterally in the skeleton (very large bending moments), and is mostly cortical bone with a limited blood supply. So a malreduced or medially-deficient fracture cycles enormous load through the implant → fatigue failure and nonunion — which is exactly why restoring the medial column and an anatomical reduction matter more than the nail-versus-plate choice.
Implant selection in detail

- 1Assess the piriformis fossaIntact (Type I) → an intramedullary nail is straightforward; involved (Type II) → do NOT ream a standard piriformis-entry nail through the fracture.
- 2Assess the medial column (lesser trochanter)Intact (A) → standard construct; detached/comminuted (B) → plan against varus collapse with medial support, valgus reduction, or a plate that spans the proximal fragment.
- 3Type II → trochanteric entry or plateA trochanteric-entry reconstruction nail bypasses the fractured fossa; a 95° blade plate / proximal femoral locking plate gives direct reduction of both columns.
- 4Reduce well, whatever the implantSubtrochanteric malreduction (varus, flexion of the proximal fragment) drives nonunion regardless of implant — anatomical/biological reduction matters more than nail-versus-plate.
- First choice
- Cephalomedullary nail
- Alternative
- Long nail if the line extends distally
- Key technical point
- Reliable entry; standard technique
- First choice
- Cephalomedullary nail + cerclage/medial support
- Alternative
- Proximal femoral locking plate if medial comminution prevents reduction
- Key technical point
- Rebuild the medial column; avoid varus malreduction
- First choice
- Trochanteric-entry recon nail or 95° blade plate
- Alternative
- Proximal femoral locking plate
- Key technical point
- Trochanteric entry avoids the fractured fossa; plate gives direct proximal-fragment control
- First choice
- 95° blade plate / DCS / locking plate, or trochanteric-entry recon nail
- Alternative
- Bone graft for large medial defects
- Key technical point
- Highly unstable — anatomical/biological reduction of both columns; don't force a nail through a comminuted proximal fragment
The subtrochanteric/proximal-diaphyseal region is the classic site of an atypical femoral fracture (AFF) — a stress/insufficiency fracture associated with long-term antiresorptive therapy (bisphosphonates, and also denosumab; often with glucocorticoids). Miss it and you treat it as an ordinary subtrochanteric fracture and overlook the contralateral leg.
- ASBMR radiographic features (need most of the major criteria) — located anywhere from just distal to the lesser trochanter to just proximal to the supracondylar flare; little or no trauma; a transverse or short-oblique line that begins at the lateral cortex; non-comminuted (a complete fracture may have a medial spike); and localized lateral-cortex periosteal/endosteal thickening or "beaking" at the fracture site. Minor features: generalised cortical thickening, prodromal thigh/groin pain, bilaterality and delayed healing.
- Always image the OTHER femur — AFFs are frequently bilateral; a contralateral incomplete fracture (a "dreaded black line") with pain warrants prophylactic cephalomedullary nailing.
- Management — a complete AFF is fixed with a full-length cephalomedullary nail; an incomplete painful one is nailed prophylactically. Stop the bisphosphonate, correct calcium and vitamin D, and consider teriparatide as an anabolic adjunct. Counsel the patient that union is often slower than in an ordinary fracture.
The Russell-Taylor classification
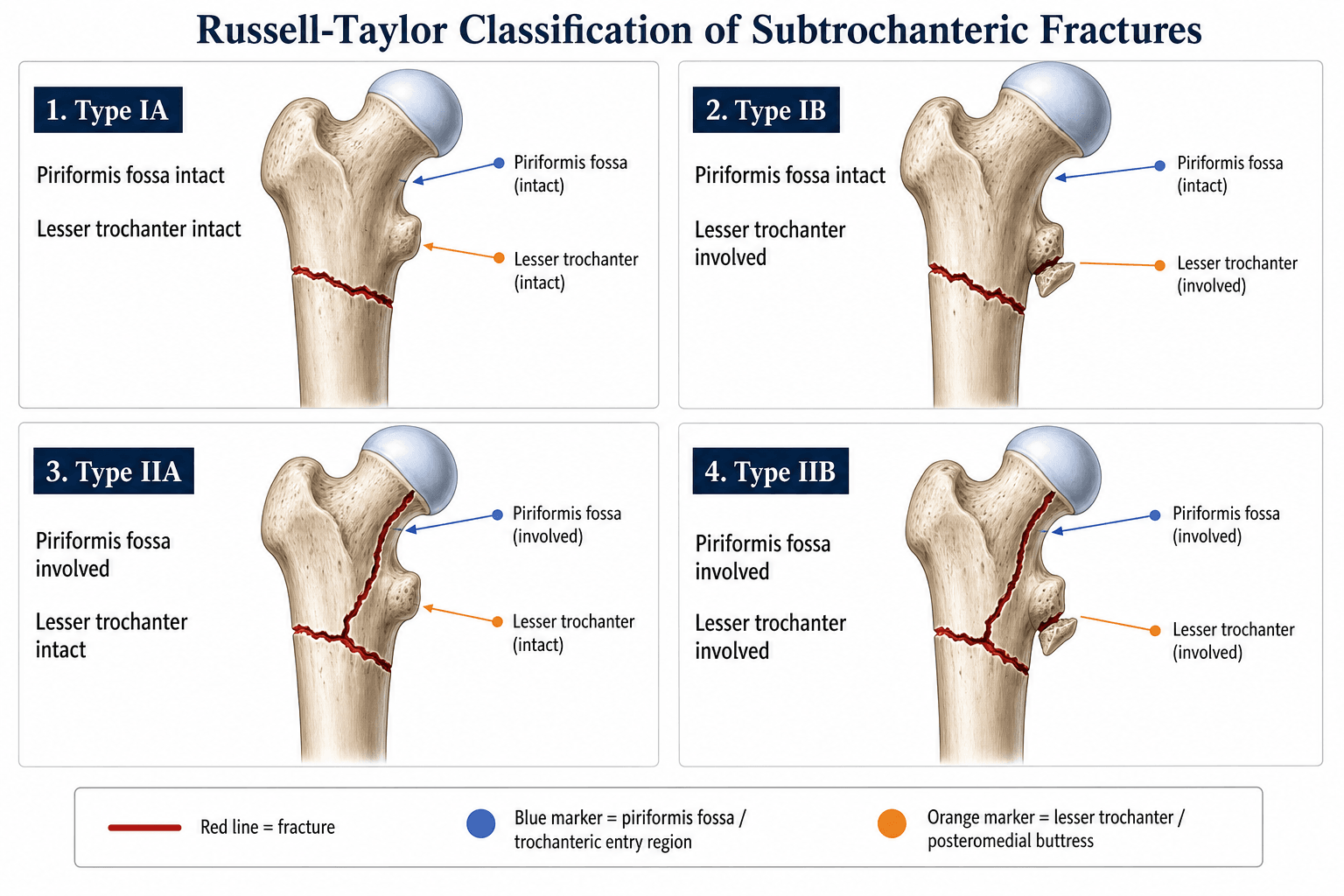

The classification uses two binary decisions applied to AP and lateral radiographs of the proximal femur.
- Piriformis fossa
- Intact
- Lesser trochanter
- Intact
- Implant implication
- Standard cephalomedullary nail
- Piriformis fossa
- Intact
- Lesser trochanter
- Involved / fragmented
- Implant implication
- Cephalomedullary nail with medial support / cable cerclage
- Piriformis fossa
- Involved
- Lesser trochanter
- Intact
- Implant implication
- Trochanteric-entry reconstruction nail or 95° plate
- Piriformis fossa
- Involved
- Lesser trochanter
- Involved / fragmented
- Implant implication
- Plate (95° blade plate or locking plate) or trochanteric-entry recon nail; highest instability
Fossa? then Lesser trochanter?The two binary decisions
Hook:First the fossa (I vs II = entry point), then the lesser trochanter (A vs B = medial buttress).
The piriformis fossa is the entry point for a first-generation (piriformis-entry) cephalomedullary nail. If the fracture line passes through it, reaming and nail insertion through that point can drive the proximal fragment into varus/extension and malreduce the fracture — the rationale for Type II avoiding a standard piriformis-entry nail. Modern caveat: most contemporary nails use a TROCHANTERIC entry point, which sidesteps the fossa, so the Type I/II distinction is less decision-critical than when Russell and Taylor devised it — and randomised trials (Starr; Lee) found little outcome difference between entry portals or between a recon nail and a plate.
Relationship to other classifications
Russell-Taylor is one of several subtrochanteric systems. The AO/OTA (31-A / 32 with subtrochanteric location) system is widely used but does not encode piriformis fossa involvement. The Seinsheimer classification subdivides by fragment number and lesser-trochanter involvement (anatomically detailed, less operationally directive). The Fielding classification divides by distance from the lesser trochanter. Russell-Taylor is the one that makes the "can I nail through the piriformis fossa?" question explicit — though, with trochanteric-entry nails now standard, that question is less pivotal than it once was.
Viva practice
- Two questions: piriformis fossa (I vs II) and lesser trochanter (A vs B).
- Type I → intramedullary nail; Type II → trochanteric-entry recon nail or plate (don't ream a standard nail through a fractured fossa).
- B subtypes lose the medial calcar buttress → varus-collapse risk → medial support or a spanning plate.
- Reduction quality (avoid varus/flexion malreduction) drives union more than the implant choice.
- Modern caveat: trochanteric-entry nails sidestep the fossa, and RCTs show comparable outcomes between portals and between recon nail and plate — so the I/II distinction is less decision-critical now.
- Russell-Taylor is the only classic system that explicitly addresses the nail entry point.
Exam viva
Practise clinical reasoning and management decisions out loud
“A 72-year-old woman is brought in after a fall. Radiographs show a subtrochanteric fracture of the right femur. The fracture line extends from below the lesser trochanter to the mid-shaft, and the lesser trochanter is fractured away from the proximal fragment. The piriformis fossa appears intact. How would you classify this fracture and what would your management plan be?”
“A 55-year-old man sustains a high-energy subtrochanteric fracture in a road traffic collision. Radiographs show the fracture line passing through the piriformis fossa with extension into the greater trochanter. The lesser trochanter is fractured and the medial cortex is comminuted over a 6 cm segment. What classification applies and what are your fixation options?”
Exam cheat sheet
The four types
- IA: piriformis fossa intact, lesser trochanter intact — cephalomedullary nail
- IB: fossa intact, lesser trochanter involved — nail + medial support/cerclage
- IIA: fossa involved, lesser trochanter intact — trochanteric-entry recon nail or blade plate
- IIB: fossa involved, lesser trochanter involved — plate or recon nail; highest instability
The two binary questions
- Piriformis fossa intact? — yes = Type I, no = Type II (decides nail entry)
- Lesser trochanter intact? — yes = A, no = B (decides medial-column stability)
- Type I = nailable; Type II = standard piriformis entry lost
- B subtypes = medial calcar gone → varus-collapse risk
Key clinical rules & caveats
- Don't ream a standard piriformis-entry nail through a fractured fossa (Type II)
- Restore the medial column / avoid varus malreduction in B subtypes
- Reduction quality drives union more than nail-versus-plate
- Modern nails use trochanteric entry, blunting the I/II distinction; RCTs show comparable portal and nail-vs-plate outcomes
Evidence
Classifications in Brief: The Russell-Taylor Classification of Subtrochanteric Hip Fracture
- A concise modern review of the Russell-Taylor classification and its four types based on piriformis fossa and lesser trochanter involvement.
- Type I (fossa intact) is amenable to standard cephalomedullary nailing; Type II (fossa involved) favours a trochanteric-entry reconstruction nail or plate.
- Notes that with the shift to trochanteric-entry nails the original piriformis-fossa-based decision has become less central in practice.
According to PubMed, the classification description comes from Rizkalla et al. 2019 (DOI 10.1097/CORR.0000000000000505); the entry-portal RCT (no difference) from Starr et al. 2006 (DOI 10.1097/00005131-200604000-00002); the nail-versus-plate RCT (comparable union) from Lee et al. 2007 (DOI 10.1097/TA.0b013e3180f62f00); the salvage of nonunion from Haidukewych & Berry 2004 (DOI 10.1097/00003086-200402000-00030); and the biomechanical nail comparison from Roberts et al. 2002 (DOI 10.1097/00005131-200204000-00003). The piriformis-entry rationale and the calcar/medial-buttress principle are standard subtrochanteric-fracture teaching; note that the higher-level trials do not show entry-portal or nail-versus-plate superiority.