- A Segond fracture is a small, crescentic avulsion of the lateral tibial plateau rim, produced by internal rotation and varus stress, and it is a pathognomonic radiographic sign of ACL disruption.
- The avulsed fragment arises from the attachment of the anterolateral ligament (ALL) or the anterolateral joint capsule — a structure that runs from the lateral femoral epicondyle to the mid-lateral tibia, between the ITB and the LCL.
- A reverse Segond fracture is a posteromedial tibial rim avulsion produced by external rotation and valgus stress; it signals PCL rupture and medial-side ligament injury rather than ACL disruption.
- Missing a Segond fragment on plain radiographs is an exam-level error. Always inspect the lateral tibial plateau closely on the AP view; even a tiny fleck should trigger MRI to evaluate the cruciate ligaments.
A Segond fracture is one of the most reliable radiographic indicators of ACL rupture — the association is reported in 75 to 100 percent of cases across large series. Conversely, nearly all complete ACL tears have some degree of anterolateral capsular injury, even if a bony Segond fragment is not visible. In the exam, the critical action is: see the fragment, suspect the ACL, order the MRI, and mention the anterolateral ligament. Failure to connect the fragment to the cruciate is the mark of an unsafe surgeon.
SALSARecognising the Segond fracture
Hook:A tiny bony fleck that shouts: look at the ACL.
ALLAnterolateral ligament anatomy
Hook:Between the band and the collateral — a narrow ribbon that locks internal rotation.
MPCLReverse Segond — think posteromedial
Hook:Medial fragment equals PCL problem — the mirror image.
Overview and Epidemiology
The Segond fracture was first described by the French surgeon Paul Segond in 1879 from cadaveric experiments on forced internal rotation of the knee. It is a small cortical avulsion from the proximal lateral tibial rim, 1 to 3 mm distal to the lateral tibial plateau and just posterior to Gerdy tubercle.
| Feature | Details |
|---|---|
| Location | Proximal lateral tibial rim, 3–4 mm distal to the lateral tibial plateau |
| Fragment size | 1–3 mm cortical fleck, elliptical or crescentic |
| Mechanism | Internal rotation + varus stress + knee near full extension |
| Structure avulsed | Anterolateral ligament and/or anterolateral joint capsule |
| Associated injury | ACL rupture (75–100%) |
| Reverse Segond | Posteromedial tibial rim avulsion — PCL + medial complex |
The injury occurs most commonly in pivoting sports such as football, skiing, rugby, and basketball, and affects patients typically aged 15 to 45 years. It accounts for a small proportion of all knee injuries but carries disproportionate clinical significance because of its near-certain association with ACL disruption. Males are affected more frequently than females, reflecting the higher participation rates in contact and pivoting sport.
Mechanism and Pathophysiology
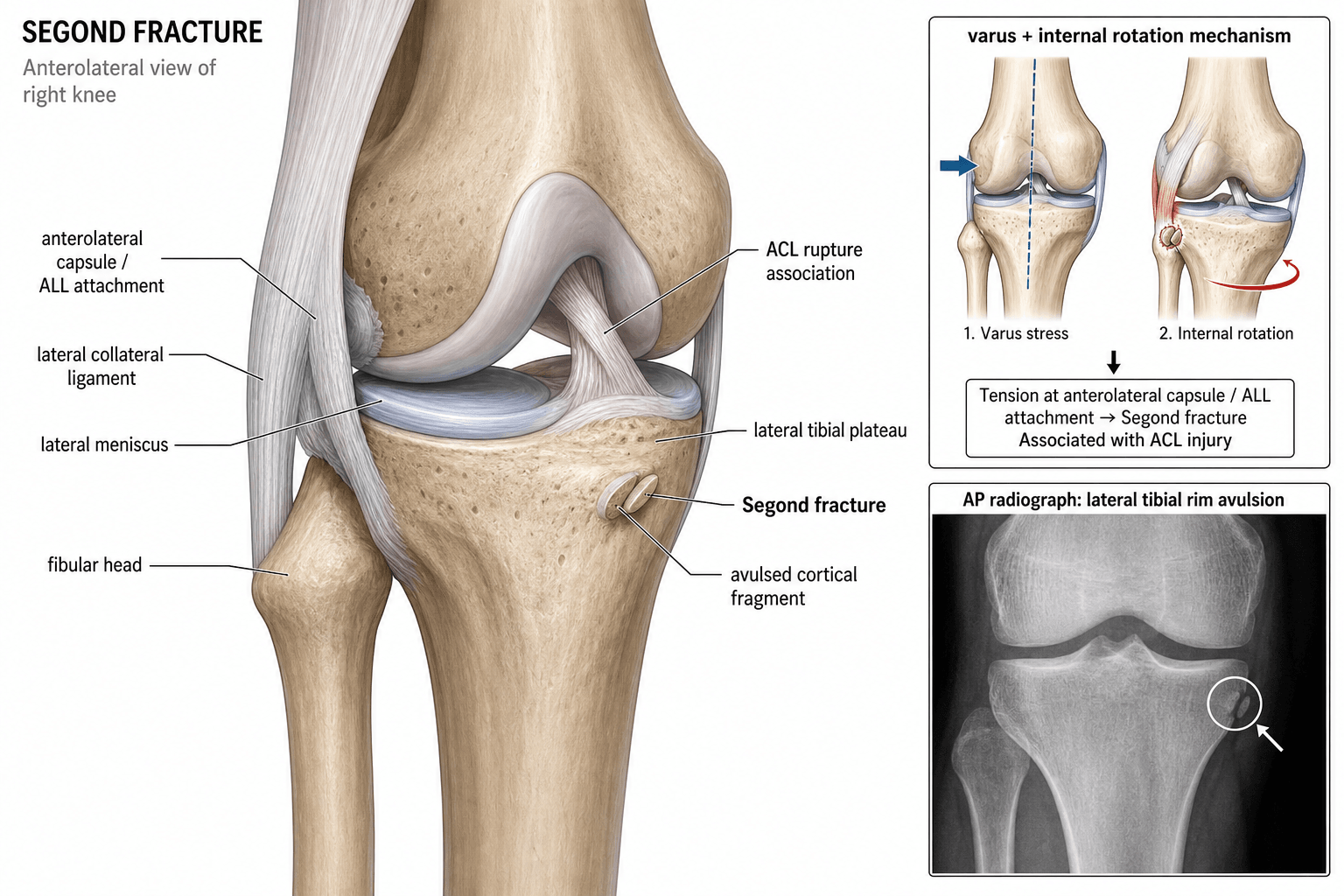
The Segond fracture is produced by a combination of internal rotation and varus stress applied to a knee that is near or at full extension. This loads the anterolateral soft-tissue envelope to failure before the ACL itself, or at the same instant.
Force transmission path:
- The tibia internally rotates relative to the femur, placing the anterolateral structures under tension.
- The anterolateral ligament (originating near the lateral femoral epicondyle, inserting on the mid-lateral tibia between Gerdy tubercle and the fibular head) resists internal rotation.
- When the tensile load exceeds the ligament's bony attachment strength, a crescentic cortical fragment is pulled off the lateral tibial plateau.
- The same rotational force simultaneously stresses and typically ruptures the ACL — either the mid-substance or femoral attachment.
The Segond fragment is therefore a bony marker of soft-tissue failure: the bone gives way at the ligament's tibial insertion, leaving the ligament itself intact (or partially torn), while the ACL sustains the full rotational load and fails.
Anatomy of the anterolateral complex:
Three key structures form the anterolateral stabilising envelope of the knee:
| Structure | Origin | Insertion | Function | Relevance to Segond |
|---|---|---|---|---|
| Iliotibial band (ITB) | Iliac crest and tensor fasciae latae | Gerdy tubercle (anterolateral tibia) | Resists varus and external rotation | Anterior to the ALL; may contribute to anterolateral stability |
| Anterolateral ligament (ALL) | Lateral femoral epicondyle (anterior/distal to LCL origin) | Mid-lateral tibia, between Gerdy tubercle and fibular head | Resists internal rotation and anterolateral rotatory laxity | The structure avulsed in a Segond fracture |
| Lateral collateral ligament (LCL) | Lateral femoral epicondyle | Fibular head | Resists varus opening | Posterior to the ALL; generally intact in Segond injuries |
The ALL was formally identified as a distinct ligament by Claes and colleagues in 2013, but its clinical significance had been recognised implicitly for over a century — the Segond fracture described in 1879 was avulsing exactly this structure. The ALL lies between the ITB (anterior) and the LCL (posterior) and is distinct from both. It tightens in internal rotation.
The Segond fragment is a bony avulsion, not a ligament rupture in isolation. The ALL may remain attached to the fragment and stay functionally intact; the critical injury is the associated ACL disruption that occurs from the same mechanism. Think of the fragment as the visible tip of a much larger soft-tissue iceberg.
Classification and Variants
Classic Segond fracture (anterolateral):
- Crescentic or elliptical cortical fragment on the proximal lateral tibial rim
- 1 to 3 mm distal to the lateral tibial plateau articular surface
- Just posterior to Gerdy tubercle, anterior to the fibular head
- Best seen on AP radiograph; may be visible on oblique views
- Pathognomonic of ACL rupture (75–100% reported association)
- Associated meniscal tears in 66 to 75 percent of cases
- Mechanism: internal rotation + varus + near full extension
Clinical Presentation and Examination
History:
- Acute twisting injury, typically during pivoting sport (football, skiing, basketball)
- Patient reports a pop or giving way at the knee
- Rapid onset haemarthrosis within hours
- Inability to continue activity; pain over the lateral joint line
- May describe the knee "shifting" or "going out"
Physical examination — practical sequence:
- Look: marked haemarthrosis, diffuse swelling, often held in slight flexion
- Feel: tenderness over the lateral joint line; palpable gap if chronic ACL laxity
- Move: restricted range, especially extension, from haemarthrosis and pain
- Special tests:
- Anterior drawer test: supine, hip flexed 45 degrees, knee flexed 90 degrees, foot stabilised on couch. Pull tibia forward. Positive if excessive anterior tibial translation compared with the contralateral side, or if a soft endpoint is felt. A firm endpoint with 5 mm or less of translation is considered normal; a soft endpoint with greater than 5 mm is highly suggestive of ACL disruption. Sensitivity improves under anaesthesia.
- Lachman test: supine, knee flexed 20 to 30 degrees. One hand stabilises the femur above the patella; the other grasps the proximal tibia and applies an anterior force. Positive with increased anterior tibial translation and a soft or absent endpoint. The Lachman is the most sensitive clinical test for ACL rupture (approximately 85% sensitivity in the acute setting, higher under anaesthesia). False negatives occur when a haemarthrosis limits positioning or when the examiner does not fully relax the patient.
- Pivot shift test: supine, knee extended, apply valgus and internal rotation while flexing. Positive when a palpable clunk occurs as the tibia subluxates anteriorly in extension and reduces at 20 to 30 degrees of flexion. Highly specific for anterolateral rotatory instability but difficult to perform in the acute, painful knee. Often requires anaesthesia or an elective follow-up.
In the viva, state the Lachman test as your most reliable acute examination for ACL integrity, and the pivot shift as your most specific test for rotatory instability. The pivot shift is often not reproducible in the acutely swollen knee — mention this limitation rather than performing a painful, uninterpretable test.
Investigations
Plain radiographs (mandatory first line):
| View | What to Look For | Diagnostic Value |
|---|---|---|
| AP view | Tiny cortical fleck on the proximal lateral tibial rim, 1–3 mm distal to plateau | |
| Lateral view | Effusion (sail sign), tibial translation anteriorly, bone bruises may suggest | |
| Oblique views | May clarify the fragment if overlapped on AP | |
| Stress views | Not indicated acutely; reserved for chronic laxity assessment |
MRI (mandatory once a Segond fragment is identified):
- Confirms ACL disruption — assess the site (mid-substance, femoral, tibial), completeness (partial versus complete), and any retraction
- Evaluates meniscal integrity — medial meniscus tears are common; lateral tears also possible
- Identifies bone bruises — lateral femoral condyle and posterolateral tibial plateau kissing pattern, characteristic of pivot-shift mechanism
- Assesses the ALL — oedema or disruption adjacent to the Segond fragment; helps differentiate ALL from ITB involvement
- Screens for posterolateral corner injury, osteochondral loose bodies, and associated fractures
On MRI, the Segond fragment shows marrow oedema at the lateral tibial rim with adjacent soft-tissue swelling. The fragment itself may be too small to identify on all sequences — look for the periosteal stripping and cortical breach at the characteristic location rather than searching for the bony fleck itself.
Management
Indications:
- Patient declined surgery or is unfit for anaesthesia
- Low-demand lifestyle, sedentary occupation
- Partial ACL tear with maintained functional stability and negative pivot shift on follow-up
Non-operative management is NOT the standard for a Segond fracture with complete ACL rupture. The Segond fragment itself is not the problem — it is the associated ACL disruption and rotatory instability that determines treatment. Non-operative care of a complete ACL tear in an active patient leads to recurrent instability, meniscal damage, and early osteoarthritis.
Rehabilitation protocol (if non-operative chosen):
- RICE for the acute phase (rest, ice, compression, elevation)
- Hinged brace for the first 3 to 6 weeks as inflammation settles
- Structured physiotherapy: quadriceps and hamstring strengthening, proprioception, closed-chain exercises
- Formal pivot-shift reassessment at 6 weeks when swelling has resolved
The Segond fragment does not require internal fixation. It is the associated ACL rupture and rotatory instability that drive the surgical decision. Fixing a 2 mm cortical fleck achieves nothing and adds risk. Treat the ACL; the fragment takes care of itself.
Complications and Prognosis
- Missed diagnosis: the most common complication. If the Segond fragment is missed on plain radiographs and the ACL tear is untreated, the patient develops chronic anterolateral rotatory instability, recurrent meniscal injury, and progressive osteoarthritis.
- Persistent rotatory instability after ACL reconstruction: if the surgeon addresses the ACL in isolation without recognising the ALL contribution, the pivot shift may persist. Consider ALL augmentation in revision cases or when the pre-operative pivot shift is high-grade.
- Meniscal loss: delayed or untreated ACL instability accelerates meniscal degeneration. Each additional giving-way episode damages the meniscus further. Early stabilisation preserves the meniscus.
- Post-traumatic osteoarthritis: develops in approximately 50 percent of patients with untreated ACL disruption at 10 to 20 years; significantly reduced by timely reconstruction combined with meniscal preservation.
- Arthrofibrosis: after ACL reconstruction, loss of extension is the most common early complication. Aggressive supervised rehabilitation with a target of full extension by 2 weeks post-operatively is the standard prevention strategy.
Evidence Base
The Segond fracture of the proximal tibia: a small avulsion that reflects major ligamentous damage
- Demonstrated that the Segond fragment is pathognomonic of ACL disruption in clinical imaging
- Correlated radiographic findings with surgical or MRI confirmation of ACL tears
- Established the fragment as a reliable indirect sign of internal derangement
Anatomy of the anterolateral ligament of the knee
- Identified a distinct anterolateral ligament in 40 of 41 cadaveric knees
- Defined the ALL as a well-defined structure from the lateral femoral epicondyle to the anterolateral tibia, between the ITB and LCL
- Proposed that the Segond fracture represents avulsion of the ALL insertion
The Segond fracture: a bony injury of the anterolateral ligament of the knee
- Demonstrated histologically that the Segond fragment contains fibres of the anterolateral ligament at its bony attachment
- Confirmed the Segond fracture as an avulsion of the ALL tibial insertion rather than a capsular injury in isolation
- Linked the Segond fragment to clinical anterolateral rotatory instability and residual pivot shift after ACL reconstruction
The reverse Segond fracture: not associated with knee dislocation and rarely with posterior cruciate ligament tear
- Defined the reverse Segond fracture as a small avulsion of the medial tibial plateau with intact medial collateral ligament fibres on MRI
- Demonstrated that the reverse Segond is more often associated with internal derangement of the medial meniscus and ACL than with frank PCL rupture
- Reaffirmed that knee dislocation is uncommon in this injury pattern, distinguishing it from the more familiar posterolateral corner disruption
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 23-year-old footballer twists his right knee during a tackle. AP radiograph of the knee shows an effusion and a 2 mm cortical fragment on the lateral aspect of the proximal tibia, just below the lateral tibial plateau. How would you proceed?”
“A 35-year-old skier sustains a hyperextension-valgus injury. Radiographs show a small cortical fragment on the posteromedial aspect of the proximal tibia. What does this signify and how does your management differ from the more common lateral pattern?”
Definition and key facts
- Small (1–3 mm) cortical avulsion of the proximal lateral tibial plateau rim
- Avulses the anterolateral ligament (ALL) or anterolateral capsule insertion
- Pathognomonic of ACL rupture (75–100% association)
- Mechanism: internal rotation + varus stress + near full knee extension
- Best seen on AP radiograph just distal to the lateral tibial plateau
Anterolateral ligament anatomy
- Origin: lateral femoral epicondyle, anterior/distal to LCL
- Insertion: mid-lateral tibia, between Gerdy tubercle and fibular head
- Lies between the ITB (anterior) and the LCL (posterior)
- Resists internal rotation and anterolateral rotatory laxity
- Identified as a distinct structure by Claes et al. in 2013
Reverse Segond
- Posteromedial tibial rim avulsion (opposite side to classic Segond)
- Mechanism: external rotation + valgus stress (hyperextension)
- Associated with PCL rupture and medial collateral ligament injury
- The fragment does not require fixation; treat the PCL and medial complex
Management principles
- MRI is mandatory once the Segond fragment is identified on plain radiograph
- The fragment itself does NOT require fixation
- ACL reconstruction is the standard for complete ACL rupture with functional instability
- Consider ALL augmentation in revision ACL cases or high-grade pivot shift
- Arthrofibrosis prevention: aim for full extension by 2 weeks post-operative