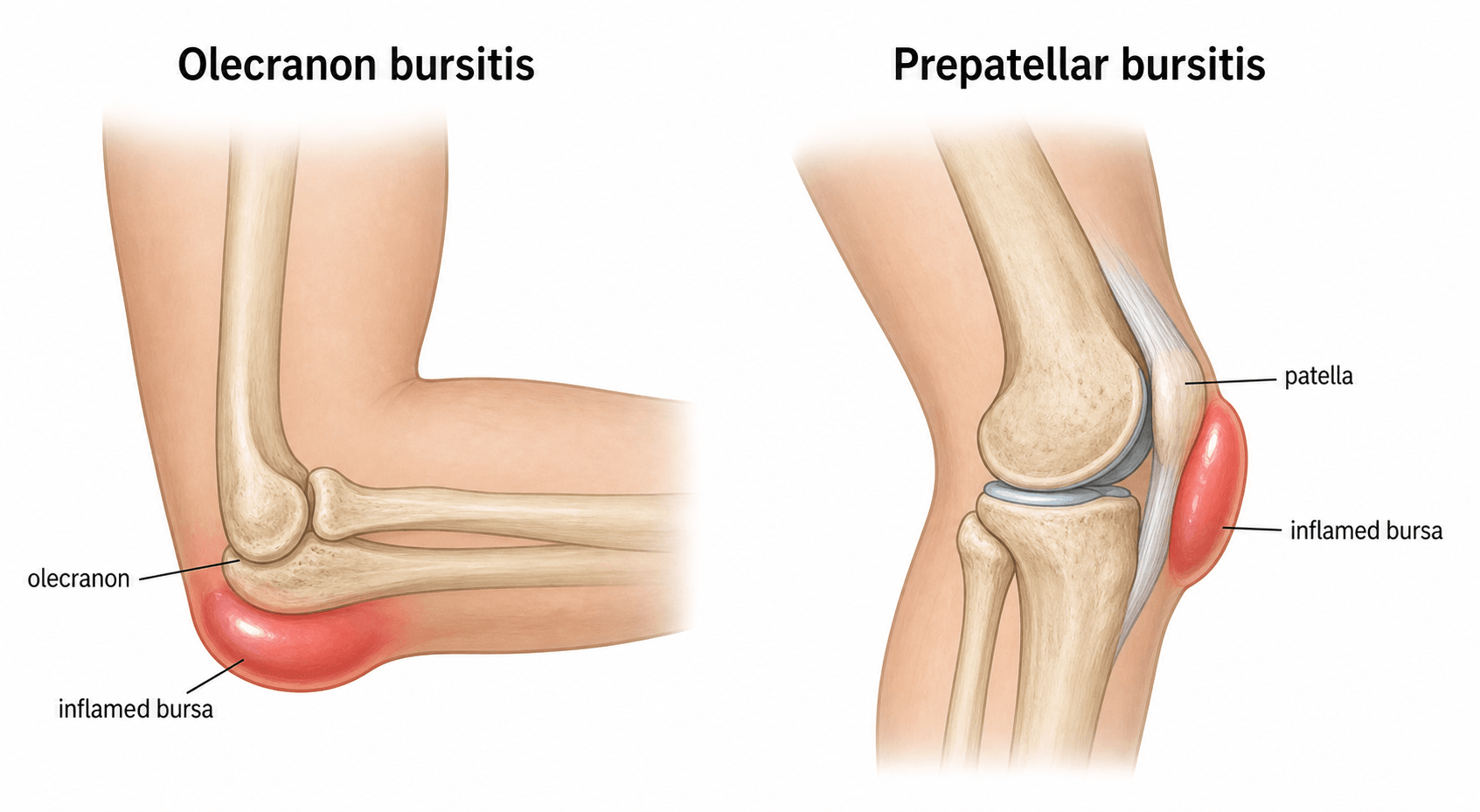
Infection of the Superficial Olecranon and Prepatellar Bursae
- Septic bursitis is infection of a bursa, most commonly the SUPERFICIAL OLECRANON (elbow) and PREPATELLAR (knee) bursae, which sit just under the skin over a bony point and are prone to TRAUMA, abrasion and direct INOCULATION (occupational kneeling/leaning - 'housemaid's knee', 'student's elbow').
- The usual organism is STAPHYLOCOCCUS AUREUS (about three-quarters of cases), followed by streptococci, reaching the bursa by direct inoculation through a skin breach; risk factors include trauma, diabetes, immunosuppression, gout and rheumatoid disease.
- Two key DISTINCTIONS: (1) SEPTIC vs NON-SEPTIC bursitis (septic has more erythema, warmth, peri-bursal tenderness and systemic features/cellulitis), and (2) septic BURSITIS vs septic ARTHRITIS - the bursa is EXTRA-articular, so PASSIVE joint movement is relatively preserved and painless in bursitis, whereas in septic arthritis any joint movement is severely painful.
- BURSAL ASPIRATION is the key investigation - send the aspirate for Gram stain, culture, cell count and CRYSTALS (also diagnoses gout/pseudogout) - performed through HEALTHY skin away from the inflamed area to avoid creating a chronic sinus; supplement with bloods (WCC/CRP).
- Most cases RESOLVE with ANTIBIOTICS (anti-staphylococcal, e.g. flucloxacillin), oral or IV depending on severity (IV preferred with fever or extensive cellulitis); evidence shows MEDICAL and SURGICAL management have EQUIVALENT success and a low failure rate, but a course SHORTER THAN 14 DAYS is associated with more failures.
- ATTACH A DOSE TO THE DRUG: typical adult regimens are FLUCLOXACILLIN 500 mg to 1 g four times daily orally (1-2 g QDS intravenously if febrile or with extensive cellulitis), CLINDAMYCIN 300-450 mg QDS or DOXYCYCLINE 100 mg BD in penicillin allergy, and VANCOMYCIN or an oral agent such as doxycycline or co-trimoxazole where MRSA is suspected - adjusted to local policy, renal function and culture. Streptococci are about a fifth of cases so the regimen must cover them, and in the IMMUNOCOMPROMISED mycobacterial and fungal bursal infection will not grow on routine culture unless specifically requested.
- SEPTIC BURSITIS IS LARGELY AN OUTPATIENT PROBLEM despite how alarming the limb looks: in a prospective series of 47 patients with acute bursal swelling (22 septic) managed by a structured protocol, NO patient was admitted initially, only two were admitted later for two days each, and only one needed incision and drainage - with review at TWO TO THREE DAYS being what the approach depends on. Admit for genuine systemic sepsis, spreading cellulitis, significant immunocompromise, an abscess needing drainage, or where early review cannot be guaranteed.
- IF SURGERY IS NEEDED THE WOUND IS THE PROBLEM: open bursectomy goes through skin directly over the bursa, whose blood supply is tenuous and which is the surface the patient leans or kneels on, hence necrosis and dehiscence. Keep the incision OFF that surface (transverse or parapatellar, never midline over the kneeling point), and note that ENDOSCOPIC BURSECTOMY in 27 recalcitrant septic bursae produced NO wound-healing complications and one minor recurrence.
- SURGERY (incision/drainage or bursectomy) is reserved for an ABSCESS, a retained FOREIGN BODY, FAILED medical therapy, or chronic/recurrent disease; bursectomy is also used for refractory chronic non-septic bursitis.
- “Olecranon & prepatellar = the commonly infected superficial bursae; Staph aureus ~75-80%.
- “Bursitis is EXTRA-articular: passive joint movement preserved (vs septic arthritis where movement is agonising). Aspirate (Gram/culture/cell count/crystals) through healthy skin.
- “Most resolve with antibiotics (>=14 days); surgery only for abscess/foreign body/failure - medical = surgical success.
- “Doses: flucloxacillin 500 mg-1 g QDS PO (1-2 g QDS IV if febrile); clindamycin 300-450 mg QDS or doxycycline 100 mg BD if penicillin-allergic; vancomycin if MRSA. Cover strep too (~19%).
- “Outpatient, not admission: 0 of 47 patients needed initial admission on a structured protocol with review at 2-3 days. Admit for systemic sepsis, spreading cellulitis, abscess, immunocompromise or unreliable follow-up.
- “Operating? Keep the incision OFF the kneeling/leaning surface (transverse or parapatellar, never midline) - the skin there has a tenuous blood supply. Endoscopic bursectomy: 27 cases, no wound complications, 1 minor recurrence.
Swelling over the bursa; PASSIVE joint movement preserved and relatively painless. Mostly treated with antibiotics.
The joint is infected; any movement is agonising, with a hot, held joint. A surgical emergency - washout. (See Septic Arthritis.)
Anatomy, Risk Factors & Presentation
The olecranon and prepatellar bursae are superficial, lying between skin and a bony prominence where they reduce friction; this exposes them to repetitive pressure (kneeling/leaning) and abrasions, which can inoculate organisms directly. Septic bursitis therefore commonly follows minor trauma to the elbow or knee, especially in manual/kneeling workers, and is more frequent with diabetes, immunosuppression, gout and rheumatoid disease. Patients present with a warm, red, tender, fluctuant swelling over the bursa; features favouring a septic rather than non-septic cause are greater erythema and warmth, peri-bursal tenderness, surrounding cellulitis and systemic features (fever) - though clinical differentiation is unreliable, hence the need for aspiration.

Investigation & Management
- Aspiration: the key test - send bursal fluid for Gram stain, culture, cell count and crystals (which also diagnoses gout/pseudogout). Aspirate through healthy skin away from the inflamed area to avoid a chronic sinus. Add WCC/CRP; image only if a foreign body or deeper collection is suspected.
- Confirm it is bursitis, not septic arthritis: check that passive joint movement is preserved and relatively painless.
- Antibiotics (mainstay): anti-staphylococcal (e.g. flucloxacillin), oral for mild cases and IV if there is fever or extensive cellulitis, refined by culture; treat for at least ~14 days (shorter courses fail more often).
- Surgery: reserve incision and drainage or bursectomy for an abscess, a foreign body, or failed medical therapy; medical and surgical management have equivalent success, so antibiotics are first-line for uncomplicated cases.
- Adjuncts: rest, compression, elevation, avoid further pressure/trauma.
Do not aspirate or incise directly through the most inflamed/thin skin over the bursa - this can leave a draining sinus. Aspirate through adjacent healthy skin, and treat infection adequately before any elective bursectomy. In a chronic, recurrent or thickened bursa that has failed conservative care, plan an elective bursectomy once infection is controlled, and counsel about wound-healing problems over the olecranon/patella.
Keep the risk in proportion, though: in the prospective series of 47 acute bursitis patients, three developed a discharging sinus and all three healed spontaneously. A sinus is a real reason to choose the needle's entry point carefully, not a reason to avoid aspirating a bursa you believe is infected - and the converse error matters more. Aspiration is mandatory when infection is suspected, but a bland, chronically thickened, non-infected bursa should generally not be tapped at all, because that is precisely how iatrogenic septic bursitis is created (developed in Prepatellar Bursitis).
Antibiotic Choice, Setting, and the Surgical Options
Which Antibiotic, at What Dose
Empirical cover is directed at Staphylococcus aureus while also covering streptococci. Typical adult regimens, to be adjusted to local antimicrobial policy, renal function and the culture result:
- Typical adult regimen
- Flucloxacillin 500 mg to 1 g four times daily
- Note
- First choice where MRSA is not suspected; covers Staph aureus and streptococci
- Typical adult regimen
- Clindamycin 300-450 mg four times daily, or doxycycline 100 mg twice daily
- Note
- Clindamycin also covers most streptococci; counsel about C. difficile
- Typical adult regimen
- Doxycycline, co-trimoxazole or clindamycin orally; vancomycin or teicoplanin if intravenous
- Note
- Suspect with prior MRSA, recent healthcare exposure or failure of flucloxacillin
- Typical adult regimen
- Flucloxacillin 1-2 g four times daily IV (vancomycin if MRSA suspected)
- Note
- Step down to oral once settling; the total course still runs to at least 14 days
Duration is the part that changes outcome. A course of at least 14 days applies whether the patient was treated medically or surgically - shorter courses failed more often in the multicentre data, and duration was the variable that separated success from failure rather than the choice between antibiotics and an operation.
Streptococci account for about a fifth of cases, so a regimen must cover them as well as staphylococci. In the immunocompromised, remember that mycobacterial and fungal bursal infection exist and will not grow on routine culture - ask the laboratory specifically if the picture is indolent and standard cultures are sterile.
Where the Patient Is Treated
Septic bursitis is largely an outpatient problem, which is worth stating because the inflamed elbow or knee looks alarming. In a prospective series of 47 patients with acute olecranon or prepatellar bursal swelling - 22 of them septic - managed by a structured protocol, no patient was admitted initially; only two were admitted later, for two days each, and only one required incision and drainage. Pain scores fell from 4.8 to 1.7 for olecranon and 3.8 to 2.7 for prepatellar septic bursitis by the first review, which was at two to three days - so a definite early review, rather than admission, is what the structured approach depends on.
Reserve admission for genuine systemic sepsis, extensive or rapidly spreading cellulitis, significant immunocompromise or uncontrolled diabetes, an abscess needing drainage, or an unreliable social situation where early review cannot be guaranteed.
Open Versus Endoscopic Bursectomy
When surgery is needed, the wound is the problem, and the reason is anatomical: an open bursectomy is performed through an incision directly over the bursa, where the skin has a tenuous blood supply and is the surface the patient leans or kneels on - hence the well-recognised rate of necrosis and dehiscence.
- Placing an open incision. Avoid a midline longitudinal incision over the kneeling or leaning surface; a transverse or parapatellar approach keeps the scar off the point of contact - the part of the knee that meets the floor, or the part of the elbow that meets the desk.
- Endoscopic bursectomy is the alternative, initially described for aseptic disease and since applied to infection. In a series of 27 recalcitrant septic bursae (14 olecranon, 13 prepatellar) it produced no wound-healing complications and one minor recurrence, with shorter hospital stays - directly addressing the wound problem that makes the open operation unattractive. The concern it was designed to answer was whether endoscopy debrides infected tissue thoroughly enough to prevent recurrence; that series suggests it does.
Attach a dose to the drug: flucloxacillin 500 mg-1 g QDS orally, clindamycin or doxycycline for penicillin allergy, vancomycin if MRSA is suspected - and at least 14 days whichever route, medical or surgical. Manage as an outpatient with review at two to three days; in a structured series none of 47 patients needed initial admission. If operating, keep the incision off the leaning or kneeling surface, and know that endoscopic bursectomy avoids the wound-healing problem of the open approach.
The Differential of a Swelling Over the Olecranon or Patella
Septic versus non-septic, and bursitis versus septic arthritis, both assume the lump is a bursitis at all. The wider differential of a swelling over these superficial bony points splits into the non-septic bursitis subtypes and the non-bursitis mimics - and the aspirate plus a radiograph sort most of them.
- Discriminating clue
- Marked erythema/warmth, peri-bursal tenderness, cellulitis, fever; aspirate positive on culture/Gram
- What it means for management
- Aspirate before antibiotics, then antibiotics covering Staph aureus; surgical drainage if it fails to settle or the bursa is loculated
- Discriminating clue
- Recent knock; serous or bloodstained aspirate; less erythema, no systemic features
- What it means for management
- (conservative - rest/compression)
- Discriminating clue
- Known gout/tophi or chondrocalcinosis; urate or CPPD crystals on aspirate
- What it means for management
- Treat the crystal arthropathy - but remember crystals and infection can coexist, so send culture even when crystals are seen
- Discriminating clue
- Rheumatoid arthritis, often bilateral; associated rheumatoid nodules
- What it means for management
- (treat the underlying RA)
- Discriminating clue
- Acute injury, bony point tenderness, effusion; lucent line on radiograph
- What it means for management
- A fracture, not a bursal problem - radiograph before you aspirate anything after trauma
- Discriminating clue
- Firm, chronic, NOT fluctuant; not warm; no fever
- What it means for management
- Not an acute problem - but a firm chronic lump that is not clearly a tophus needs imaging and a mass work-up rather than repeated aspiration
Interpreting the Bursal Aspirate
Aspiration is the key test that differentiates septic from non-septic, but how it is interpreted is the examinable point - because, unlike a joint, no single bursal-fluid number is decisive.
- Gram stain and culture are decisive: a positive result confirms septic bursitis and guides antibiotics. In the evidence an organism is identifiable in about two-thirds of cases.
- Cell count: a raised white-cell count with neutrophil predominance supports infection, but the threshold is lower and overlaps more than synovial fluid in septic arthritis - so there is no single reliable cut-off (the septic-arthritis synovial thresholds belong to that topic, not here).
- A sterile aspirate does NOT exclude septic bursitis (about a fifth of bursal samples are culture- negative, and prior antibiotics lower the yield) - treat on the whole picture.
- Crystals do NOT exclude infection: urate/CPPD crystals diagnose gout/pseudogout but can co-exist with sepsis, so still culture and cover empirically if the picture is septic.
- Bloods (WCC/CRP) support but are non-specific.
Culture and Gram stain are the only things that confirm septic bursitis; cell count merely supports it (lower, overlapping thresholds vs a joint). A negative culture does not exclude infection, and crystals do not exclude it either - so when the clinical picture is septic, treat empirically and let culture refine it.
Mnemonics & Memory Aids
BURSA
Hook:Run through BURSA for any septic bursitis.
NOT ARTHRITIS
Hook:Septic bursitis is NOT septic arthritis - passive joint movement is preserved.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A manual worker has a hot, red, swollen elbow tip after kneeling/leaning a lot. How do you assess and manage it?”
“When would you operate on septic bursitis, and how do you avoid complications?”
Sites & cause
- Olecranon (elbow) and prepatellar (knee) superficial bursae
- Direct inoculation via trauma/abrasion (kneeling/leaning)
- Staph aureus ~75-80%, then strep; risk: diabetes, immunosuppression, gout/RA
Two distinctions
- Septic vs non-septic (erythema/warmth/peri-bursal tenderness/fever/cellulitis)
- Bursitis vs septic arthritis: passive joint movement PRESERVED in bursitis
- Aspirate through healthy skin (avoid sinus): Gram/culture/cell count/crystals
Management
- Flucloxacillin 500 mg-1 g QDS PO; 1-2 g QDS IV if febrile/extensive cellulitis
- Penicillin allergy: clindamycin 300-450 mg QDS or doxycycline 100 mg BD
- MRSA suspected: vancomycin IV, or doxycycline/co-trimoxazole/clindamycin PO
- At least 14 days whichever route - shorter courses fail more often
- Rest/compress/elevate; avoid further pressure
- Surgery (I&D/bursectomy) for abscess/foreign body/failure; medical = surgical success
Setting & surgical detail
- Outpatient with review at 2-3 days: 0 of 47 needed initial admission
- Admit for systemic sepsis, spreading cellulitis, abscess, immunocompromise, unreliable follow-up
- Open bursectomy incision must avoid the kneeling/leaning surface (transverse or parapatellar)
- Endoscopic bursectomy: 27 recalcitrant cases, no wound complications, 1 minor recurrence
- Immunocompromised: ask for mycobacterial and fungal cultures - routine culture misses them
Pitfalls
- Chronic sinus from incising inflamed thin skin
- Short antibiotic course (under 14 days) -> more failures
- Missing concurrent septic arthritis
Evidence & Key Studies
Clinical characteristics and management of olecranon and prepatellar septic bursitis: a multicentre study
- In 272 patients, an organism was identified in 67.6% (almost all from bursal fluid): staphylococci 73.4%, streptococci 19%, polymicrobial 5.5%.
- Only 26% were treated surgically; medical and surgical management had EQUIVALENT success, with a low overall failure rate (5.9%).
- Failures were more frequent when antibiotic therapy lasted less than 14 days - supporting an adequate course in both medical and surgical groups.
Current treatment concepts for olecranon and prepatellar bursitis
- Differentiation between septic and non-septic bursitis was based mainly on history/clinical presentation and blood sampling, with bursal aspiration used variably.
- Practice varied widely between surgeons, with some favouring surgery and others conservative care.
- The international literature argues for a CONSERVATIVE (antibiotic) treatment approach, reserving surgery for complicated cases.
Management of acute bursitis: outcome study of a structured approach
- Of 47 consecutive patients attending with acute olecranon or prepatellar bursal swelling, 22 had septic bursitis (15 olecranon, 7 prepatellar), managed by a structured outpatient protocol with review at two to three days.
- No patient was admitted initially; two were admitted later for two days each, and only one required incision and drainage - so a protocol with defined criteria produced good results with little need for operation or admission.
- Three patients developed discharging sinuses and all healed spontaneously; every patient recovered symptomatically and could lean on the elbow or kneel by the end of follow-up (up to 18 months).
Surgical outcomes in endoscopic versus open bursectomy of the septic prepatellar or olecranon bursa
- Open bursectomy is performed through an incision directly over the bursa, where the tenuous blood supply of the overlying skin produces a high rate of wound-healing problems including necrosis and dehiscence - the reason an alternative was sought.
- In 27 recalcitrant septic bursae (14 olecranon, 13 prepatellar) treated by endoscopic bursectomy there were no wound-healing complications and one minor recurrence, with shorter hospital stays.
- The uncertainty endoscopy had to answer was whether it debrides infected tissue thoroughly enough to prevent recurrence; these results suggest it does.
The microbiology (staphylococci 73.4%, streptococci 19%, polymicrobial 5.5%, with an organism identified in 67.6% of 272 patients), the equivalent success of medical versus surgical management, the 5.9% failure rate and the importance of a course of at least 14 days come from the cited Charret multicentre study; the practice variation with international support for conservative treatment from the cited Baumbach survey. The outpatient management figures - no initial admissions among 47 patients, review at two to three days, one incision and drainage, and three sinuses that all healed spontaneously - are Stell. The wound-healing rationale for avoiding an incision over the bursa, and the endoscopic bursectomy outcomes in 27 recalcitrant cases, are Meade.
The antibiotic agents and doses are standard formulary practice for staphylococcal skin and soft-tissue infection rather than figures from a septic-bursitis trial, and should be adjusted to local antimicrobial policy, renal function and culture; what the cited evidence does establish is the duration. The caution against tapping a bland, non-infected chronic bursa, and the rule of keeping an incision off the kneeling surface, are taken in substance from Prepatellar Bursitis. The septic-vs-non-septic and bursitis-vs-septic-arthritis distinctions and the aspiration technique are standard clinical teaching. (See also Septic Arthritis and Osteomyelitis.)