Open distal phalanx physeal fracture, nail-bed injury and infection prevention
- Definition: distal phalanx physeal or juxta-epiphyseal fracture with associated nail-bed injury.
- It mimics a mallet finger but behaves like an open fracture.
- The nail plate may lie superficial to the eponychial fold rather than tucked under it.
- Interposed germinal matrix or nail bed prevents stable closed reduction.
- Delayed recognition increases infection, osteomyelitis, non-union, malunion, nail deformity and growth disturbance.
- “Blood at the proximal nail fold in a child with a flexed distal phalanx is the red flag.
- “Request true AP and lateral views of the digit, not only a hand film.
- “Remove or elevate the nail plate to inspect, debride and repair the nail bed.
- “Use K-wire fixation when reduction is unstable after soft-tissue interposition is cleared.
A child with a mallet-like distal phalanx posture plus blood at the nail fold has a Seymour fracture until proven otherwise. Splinting alone can leave germinal matrix trapped in the fracture and convert a small injury into osteomyelitis, nail deformity or physeal arrest.
Images and Diagrams


| Question | Answer | Clinical use |
|---|---|---|
| What is it? | Open paediatric distal phalanx physeal fracture with nail-bed injury | Do not manage it like a simple mallet finger |
| Clinical clue? | Mallet posture, blood at nail fold and nail plate perched above the eponychial fold | Inspect the nail fold before accepting the diagnosis |
| Key blocker? | Germinal matrix or nail-bed tissue in the fracture | Explains failed closed reduction |
| Core treatment? | Antibiotics, tetanus check, washout, debridement, reduction, nail-bed repair and fixation if unstable | Prevents infection and nail/growth complications |
NAILRecognition Clues
Hook:NAIL separates Seymour fracture from a harmless-looking mallet injury.
WASHOpen Fracture Priorities
Hook:WASH is the operative logic of an acute Seymour fracture.
MALTNot a Simple Mallet
Hook:MALT reminds learners why mallet-style splinting alone is unsafe.
Overview/Epidemiology
A Seymour fracture is a paediatric distal phalanx physeal or juxta-epiphyseal fracture with associated nail-bed injury. In practical terms, it is an open fracture until proven otherwise. The injury usually follows a fingertip crush, door injury, ball strike, fall, forced flexion injury or great-toe stubbing mechanism. The X-ray may look small, but the open nail-bed wound makes the injury high risk.
The classic clinical trap is that Seymour fractures resemble mallet finger, but the treatment is different.
| Finding | Seymour fracture implication | Risk if treated as mallet finger |
|---|---|---|
| Flexed distal phalanx | May look like terminal extensor injury but the fracture involves the distal phalanx physis or juxta-epiphyseal region. | Splinting may leave the fracture unreduced. |
| Blood at proximal nail fold | Suggests nail-bed violation and open fracture communication. | Open fracture may be missed. |
| Nail plate out of eponychial fold | Indicates proximal nail-bed disruption. | Germinal matrix may remain interposed. |
| Reduction keeps springing back | Soft-tissue block is likely. | Persistent malreduction, infection, non-union and nail deformity. |
The consultation should answer four questions:
- Is this a nail-bed wound communicating with bone?
- Is the fracture through or near the open distal phalanx physis?
- Is germinal matrix or nail bed interposed in the fracture?
- Is the reduction stable after the soft-tissue block is cleared?
The great toe has an equivalent injury after axial load or stubbing trauma. It is less commonly discussed than finger Seymour fracture, but the logic is the same: nail-bed injury plus distal phalangeal physis involvement requires open-fracture thinking.
Pathophysiology
The distal phalanx physis lies near the base of the distal phalanx, close to the nail-bed complex. In a Seymour fracture, the distal phalanx is forced into a flexed posture through the weak physeal or juxta-epiphyseal region.
| Structure | Role in Seymour fracture | Clinical consequence |
|---|---|---|
| Distal phalanx physis | The fracture passes through or near the growing base of the distal phalanx. | Growth disturbance is possible if missed or infected. |
| Terminal extensor tendon | Attached dorsally near the epiphysis, creating a mallet-like posture. | The posture can mislead the clinician. |
| FDP insertion | Volar distal insertion contributes to flexion posture and distal fragment control. | Motion does not exclude the fracture. |
| Nail bed and germinal matrix | Tears at the same level and may fold into the fracture. | Blocks reduction and increases infection risk. |
The important soft-tissue structure is the germinal matrix. It produces most of the nail and sits deep to the proximal nail plate. When the nail plate is avulsed or displaced, the germinal matrix can fold into the fracture gap. This creates two problems: it blocks reduction and it leaves devitalised or contaminated soft tissue inside an open physeal fracture.
The nail plate position is therefore diagnostic. A normal nail plate tucks beneath the eponychial fold. In Seymour fracture, the proximal edge of the nail plate may sit on top of the eponychial fold, making the nail look too long. This subtle sign may be more obvious than the X-ray.
The injury behaves differently from a simple tuft fracture or mallet finger because the open physis and nail-bed laceration connect the outside environment with the growth plate and distal phalanx. That is why early antibiotics, debridement, reduction and nail-bed repair matter.
Mechanism
The usual mechanism is a crush or forced-flexion load to the fingertip. Door-crush injuries are common, but ball sports, falls, machinery, direct blows and toe-stubbing injuries can produce the same pattern. The child often presents with pain, swelling, bleeding at the nail fold and a fingertip that appears flexed at the DIP joint.
Mechanistically, the injury sits between two familiar patterns:
- Like mallet finger, the distal phalanx appears flexed.
- Like an open fracture, there is communication through the nail bed.
- Like a physeal fracture, growth disturbance is possible.
- Like a nail-bed laceration, final nail appearance depends on precise soft-tissue repair.
This combination is why the diagnosis is easy to underestimate. The wound may be tiny, the child may move the finger, and the X-ray may show only subtle physeal widening. The red flag is the combination of distal phalanx posture and proximal nail-fold injury.
Classification
Seymour fractures are commonly described as Salter-Harris I, Salter-Harris II or juxta-epiphyseal distal phalanx injuries. This classification confirms the injury involves the growing distal phalanx base, but it does not by itself decide treatment. Treatment is driven by nail-bed violation, displacement, soft-tissue interposition, contamination, timing and stability.
- Salter-Harris I: fracture through the distal phalanx physis, sometimes only seen as widening on the lateral film.
- Salter-Harris II: physeal fracture with a small metaphyseal fragment.
- Juxta-epiphyseal: fracture just distal to the physis, behaving similarly in the clinical setting.
- Tuft fracture with nail-bed injury: more distal crush injury; nail-bed repair may be required, but it is not the classic basal physeal Seymour injury.
Clinical Presentation
History
The history should quickly determine mechanism, contamination, delay and infection risk.
- Mechanism: door crush, ball injury, fall, forced flexion, direct blow, machinery injury or toe stubbing.
- Time from injury: delayed presentation changes infection risk and debridement planning.
- Nail symptoms: bleeding at the proximal nail fold, nail plate avulsion, nail plate sitting high, subungual haematoma or visible nail-bed wound.
- Contamination: soil, farm injury, water exposure, bite, dirty sports field or foreign material.
- Previous treatment: antibiotics, splinting, trephination, nail removal or attempted reduction.
- Infection symptoms: increasing pain, redness, discharge, fever, odour or progressive swelling.
- Functional context: digit involved, hand dominance, school or sport needs, and associated fingertip injuries.
Examination
Inspection is the most important part of the examination. A Seymour fracture may look like a minor nail injury unless the proximal nail fold is examined carefully.
| Area | Look for | Why it matters |
|---|---|---|
| Posture | Mallet-like flexion posture of the distal phalanx. | Raises suspicion for Seymour fracture in a child. |
| Nail fold | Blood at proximal nail fold, nail plate superficial to eponychial fold or nail appearing too long proximally. | Suggests open nail-bed injury and possible matrix interposition. |
| Nail bed | Transverse matrix laceration, subungual haematoma, nail avulsion, exposed matrix or open wound. | Determines need for washout and nail-bed repair. |
| Distal digit | Tenderness, swelling, pulp viability, capillary refill and sensation. | Documents open fracture severity and neurovascular baseline. |
| Hand alignment | Rotational alignment, finger cascade and associated crush injuries. | Avoids missing a second injury. |
Active motion can be misleading. A child may still flex through the FDP and may have pain-limited extension. Preserved motion does not exclude an open physeal injury.
The nail fold tells the story. A child with a flexed distal phalanx and blood at the proximal nail fold should be treated as having an open physeal fracture until imaging and inspection prove otherwise.
Investigations
| Clinical question | Investigation | Decision it informs |
|---|---|---|
| Confirm fracture pattern | True AP and true lateral radiographs of the affected digit | Shows physeal widening, juxta-epiphyseal fracture and flexion displacement |
| Assess open injury | Clinical inspection of nail fold and nail bed | Determines need for open-fracture pathway |
| Delayed or infected case | FBC, CRP, ESR, cultures if discharge or systemic illness | Guides infection severity and antibiotic plan |
| Suspected osteomyelitis | MRI if extent is uncertain or symptoms are disproportionate | Defines marrow involvement and abscess |
Obtain dedicated radiographs of the affected digit, not just a hand X-ray. The AP view helps with alignment and associated fractures, but the true lateral view is the key image. The lateral view shows the relationship between the distal phalanx epiphysis, physis, metaphysis and nail plate.
Look for:
- Widening of the distal phalanx physis.
- Salter-Harris I or II fracture pattern.
- Juxta-epiphyseal fracture just distal to the physis.
- Flexion deformity or volar angulation of the distal fragment.
- Nail plate displacement or soft-tissue swelling.
- Subtle physeal asymmetry compared with the contralateral digit if uncertain.
Imaging cannot replace the nail-fold examination. A tiny radiographic abnormality with proximal nail-fold bleeding is still clinically important. Conversely, an apparent mallet posture in a skeletally immature patient should not be accepted as simple tendinous mallet injury until the nail bed and lateral film are reassuring.
Differential Diagnosis
The differential diagnosis matters because each injury has a different treatment pathway.
| Diagnosis | Distinguishing features | Why it matters |
|---|---|---|
| Tendinous mallet finger | Closed terminal extensor injury, no nail-bed wound, no physeal widening | Usually treated with extension splinting rather than open-fracture care |
| Bony mallet fracture | Dorsal intra-articular avulsion fragment at the distal phalanx base | Assess articular fragment size and DIP subluxation |
| Tuft fracture with nail-bed injury | More distal crush fracture through the tuft rather than basal physis | Nail-bed repair and protection may be needed, but it is not the same physeal injury |
| Subungual haematoma | Painful nail bleeding; nail plate may be intact | Radiographs decide whether fracture management is also required |
| Paronychia, felon or osteomyelitis | Delayed pain, swelling, discharge, redness or systemic symptoms | May be the presentation of a missed open Seymour fracture |
| Simple nail-bed laceration | No physeal fracture or distal phalanx instability | Needs precise soft-tissue repair but not fracture reduction |
Management

Management is built around a simple principle: if the nail bed is violated and the distal phalanx physis is injured, this is an open fracture. The aim is to prevent infection, remove the soft-tissue block, restore distal phalanx alignment, repair the nail bed and protect the reduction until union.
- Give analgesia and protect the fingertip with a sterile dressing.
- Treat as an open fracture when nail-bed laceration or proximal nail-fold bleeding is present.
- Start antibiotics according to local open-fracture and hand-injury protocol.
- Check tetanus status.
- Obtain dedicated digit X-rays before definitive manipulation unless vascular compromise demands immediate action.
Operative Technique

Preparation
Confirm the diagnosis clinically and radiographically. Consent should cover open fracture care, nail-bed repair, possible K-wire fixation, infection, nail deformity, stiffness, malunion, non-union, physeal disturbance and possible further surgery. Give antibiotics according to local open-fracture and paediatric hand protocols. Check tetanus status.
Exposure and debridement
| Step | How to do it | Pitfall |
|---|---|---|
| Field and perfusion | Use a bloodless field when safe, while confirming fingertip perfusion is not compromised. | A tight digital tourniquet left on is unsafe. |
| Nail plate | Elevate or remove it if displaced, dirty, trapped or blocking inspection. | Leaving the nail plate in place can hide matrix interposition. |
| Eponychial fold | Handle gently and preserve the fold. | Scarring here can damage future nail growth. |
| Debridement | Irrigate thoroughly and remove dirt, clot and devitalised tissue. | Over-aggressive curettage can injure physis and germinal matrix. |
Clearing the reduction block
The germinal matrix or nail bed is often folded into the fracture. This is the reason closed reduction may repeatedly fail. Extract the interposed tissue gently with fine instruments. Do not keep forcefully manipulating the distal phalanx against a soft-tissue block.
Reduction and fixation
Reduce the distal phalanx anatomically and confirm alignment clinically and with AP and lateral imaging.
| Situation | Treatment direction | Reason |
|---|---|---|
| Stable after debridement and nail-bed repair | Splint protection may be enough. | The soft-tissue block has been cleared and alignment is reliable. |
| Displaced or unstable fracture | Use K-wire fixation. | Maintains reduction while the open physeal injury heals. |
| Delayed, contaminated or repeatedly redisplacing injury | Strongly consider K-wire fixation after debridement. | Higher risk of loss of position and infection-related complications. |
| Unreliable protection | Fix if the child cannot protect the digit safely. | Prevents recurrent displacement during healing. |
The wire often crosses the DIP joint to hold the distal phalanx, but fixation should follow fracture stability, child factors and local hand-surgery practice.
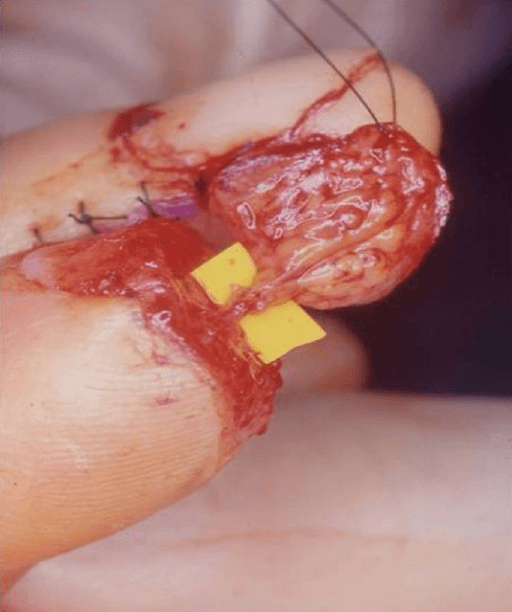
Nail-bed repair and stenting
Repair the germinal or sterile matrix precisely with fine absorbable sutures. The aim is smooth nail-bed continuity without inversion, overlap or excessive tension. Replace a clean nail plate, or use a sterile substitute, beneath the eponychial fold to prevent fold adhesion and support nail regrowth. Apply a non-adherent dressing and protective splint.
Antibiotics and Delayed Presentation
Antibiotic choice and duration should follow local paediatric open-fracture and hand-injury protocols. A typical clean acute injury is usually covered for skin flora. Broaden the discussion with senior clinicians for bites, farm injuries, water exposure, immunocompromise, gross contamination, delayed presentation or established infection.
| Presentation | Assess | Management implication |
|---|---|---|
| Delayed but not infected | Pain, nail position, wound status, X-ray alignment and signs of matrix interposition. | Treat as higher-risk open fracture; debridement and stabilisation may still be required. |
| Local infection | Discharge, redness, swelling, odour, worsening pain and pin or wound concerns. | Cultures when available, debridement, antibiotics and close hand-surgery follow-up. |
| Possible osteomyelitis | Fever, persistent pain, radiographic change, raised inflammatory markers or deep infection concern. | Senior review, targeted imaging when it changes care and longer antibiotic pathway. |
| Unwell child | Systemic signs or rapidly worsening infection. | Do not delay treatment for MRI if urgent debridement and antibiotics are needed. |
The follow-up question is not only "has the fracture united?" It is also "has infection declared itself, is the nail growing normally, and is distal phalanx growth staying acceptable?"
Complications
Early
- Missed open fracture and delayed antibiotics.
- Pin-site infection when fixation is used.
- Loss of reduction from unrecognised matrix interposition or inadequate fixation.
- Soft-tissue necrosis from crush injury or tight dressings.
- Persistent pain, swelling and stiffness.
Late
- Osteomyelitis, especially after delayed diagnosis.
- Non-union or malunion of the distal phalanx.
- Persistent mallet deformity or extensor lag.
- Nail deformity including ridging, split nail, hook nail or absent nail growth.
- Premature physeal arrest and distal phalanx growth disturbance.
- DIP stiffness and hypersensitive fingertip.
The feared complication is not the X-ray appearance on day one; it is the open physeal wound that can become infected or scar the germinal matrix if not treated properly.
Decision-Making in Practice
A Seymour fracture is small in size but high in consequence. The decision-making sequence is: recognise the open physeal injury, protect against infection, remove the soft-tissue block, restore nail-bed anatomy, stabilise the fracture if needed and follow the nail and physis.
| Decision | How to decide | Treatment consequence |
|---|---|---|
| Is it open? | Blood at nail fold, nail-bed laceration or nail plate sitting above eponychial fold | Antibiotics, tetanus check and operative-style wound thinking |
| Is reduction blocked? | Persistent displacement or nail-bed tissue in the fracture | Lift or remove nail plate and extract interposed germinal matrix |
| Is fixation needed? | Unstable reduction, marked displacement, poor compliance or delayed presentation | K-wire fixation across distal phalanx and sometimes DIP joint |
| Delayed or infected? | Discharge, erythema, fever, osteolysis or persistent pain | Cultures, debridement and targeted antibiotics |
| Follow-up focus | Union, pin site, nail growth, mallet posture and physis | Detect nail deformity, osteomyelitis or growth arrest |
The nail plate is a diagnostic structure. If it is perched on top of the eponychial fold, the germinal matrix is likely disrupted. Simply pushing the distal phalanx straight and applying a mallet splint can trap matrix in the fracture and leave contamination behind.
Operative care should be meticulous but not aggressive. Irrigate, debride devitalised tissue, remove interposed matrix, reduce anatomically, repair the nail bed with fine absorbable suture, stent the eponychial fold with the nail or substitute when appropriate, and stabilise if the fracture is unstable. Avoid repeated physeal trauma during wire placement.
Controversies and Areas of Uncertainty
The Seymour fracture is uncommon, so the evidence base is dominated by small retrospective series and a single registered systematic review protocol rather than randomised trials. Several practical questions remain genuinely unsettled and are favourite viva discussion points.
| Question | Arguments either way | Pragmatic position |
|---|---|---|
| Does every Seymour fracture need K-wire fixation? | Al-Qattan reported uncomplicated healing in all wired cases but mild flexion deformities and one infection among splinted cases; Lin and colleagues managed most acute injuries in the emergency department without theatre, and Cha and colleagues maintained reduction without wires in delayed cases. | Reserve K-wire fixation for unstable, redisplacing, markedly displaced or unreliable-protection cases rather than treating it as automatic. |
| Is nail-plate removal always required? | Removal allows full inspection and nail-bed repair; some authors elevate rather than excise a clean, adherent plate and reuse it as an eponychial stent. | Remove or elevate when inspection, debridement or matrix extraction demands it; preserve a clean plate as a stent where possible. |
| Which antibiotic and for how long? | Lin and colleagues found a first-generation cephalosporin (cephalexin) adequate for most acute injuries; contaminated, bite, water or delayed injuries justify broader cover. | Follow local open-fracture protocol; cephalexin-equivalent cover is reasonable for clean acute injuries, broaden for contamination or delay. |
| What time window defines safe acute treatment? | Most series use a 24-hour cut-off; infection risk rises sharply beyond it, but the threshold is pragmatic, not biological. | Treat within 24 hours where possible and treat all delayed cases as higher-risk open fractures. |
Evidence Signals
Delayed treatment of open Seymour fractures sharply increases infection
- 35 open Seymour fractures over 10 years at a level 1 paediatric trauma centre; 7 infections, including 5 osteomyelitis.
- Infection rate was 0 percent (0/11) with acute appropriate treatment, 15 percent (2/13) with acute partial treatment and 45 percent (5/11) with delayed treatment.
- Appropriate treatment was defined as irrigation and debridement, fracture reduction and antibiotics.
Most acute Seymour fractures can be managed without theatre
- 65 acute Seymour fractures (presenting within 24 hours) in 65 children, mean age 10 years.
- 58 of 65 (89 percent) were managed in the emergency department; 7 had primary irrigation, debridement, open reduction and K-wire fixation, usually for unsuccessful closed reduction.
- Cephalexin gave adequate cover and complications were rare, with superficial infection most common; 4 ED-managed cases needed unplanned surgery, usually for redisplacement.
Clinical Reasoning Notes
The strongest answer starts by naming the injury correctly: an open distal phalanx physeal or juxta-epiphyseal fracture with nail-bed injury. That opening phrase immediately separates it from a simple mallet finger.
The next step is to explain why the clinical appearance is deceptive. The distal phalanx is flexed, but the nail fold is the dangerous clue. If the proximal nail plate sits superficial to the eponychial fold, the germinal matrix has probably been disrupted. If germinal matrix is trapped in the fracture, reduction fails until the tissue is cleared.
Nail-bed repair is not cosmetic trivia. It is part of fracture management because the nail bed and fracture communicate. Poor matrix alignment causes nail deformity. Missed contamination causes infection. Persistent soft-tissue interposition causes malunion, non-union or redisplacement.
A safe family explanation is:
"This is a small bone injury at the end of the finger, but because the nail bed is torn it behaves like an open fracture. We need to clean it properly, put the nail bed and bone back in the right position, give antibiotics, and then watch for infection, healing and nail growth."
Common pitfalls
- Calling it a mallet finger and treating with extension splint alone.
- Ordering only a hand X-ray and missing the true lateral digit view.
- Not looking under or around the proximal nail fold.
- Trying repeated closed reductions despite a soft-tissue block.
- Forgetting antibiotics and tetanus assessment.
- Repairing skin but leaving the nail bed and physis untreated.
Evidence Base
Al-Qattan: the defining Seymour fracture series
- 25 extra-articular transverse fractures of the base of the distal phalanx across children, adolescents and adults.
- Before physeal closure the fracture line runs through the metaphysis 1 to 2 mm distal to the growth plate; in adults it lies just distal to the extensor tendon insertion.
- 18 fractures were treated by closed reduction and splinting, with 1 infection and 3 mild residual flexion deformities; all 5 K-wired fractures healed without complication, and 2 late-presenting adults developed malunion.
Seymour fractures carry a high complication rate among distal phalanx injuries
- 206 paediatric distal phalanx fractures reviewed; Seymour fractures made up 6 percent of the cohort.
- Overall complications occurred in 31 percent of children, with the highest rates in Salter-Harris IV (100 percent), Seymour (62 percent) and mallet (49 percent) fractures.
- The commonest complications were infection (22 percent), stiffness (15 percent) and nail deformity (13 percent).
Great-toe (hallux) Seymour fractures follow the same open-fracture logic
- 5 boys (mean age 10.3 years) with open physeal fractures of the hallux distal phalanx and nail-bed injury.
- 40 percent were initially missed and 60 percent were transfers, underlining frequent diagnostic delay in toe injuries.
- Suture-only stabilisation produced no infections, no reoperations and no physeal bars on follow-up imaging.
No consensus on optimal management: systematic review framing
- Confirms there is at present no consensus on the optimal management of Seymour fractures.
- Defines the injury as an open, displaced juxta-epiphyseal distal phalanx fracture with overlying nail-bed laceration in a child with an open physis.
- Sets superficial and deep infection as primary outcomes, with malunion, non-union, reoperation, physeal disturbance and nail dystrophy as secondary outcomes.
Guidelines, Registries & Global Practice
The Seymour fracture is too rare to feature in standalone society guidelines or arthroplasty registries; instead it is governed by general paediatric open-fracture principles, which are broadly concordant across major bodies. The clinically useful comparison is therefore between the open-fracture frameworks that surgeons apply to this injury worldwide.
Global epidemiology
- Seymour fractures account for roughly 6 percent of paediatric distal phalanx fractures in referral series, making them uncommon but clinically high-consequence.
- Peak incidence is in school-age children and early adolescents (mean age around 9 to 10 years across series), reflecting open-physis anatomy and crush mechanisms.
- A boy predominance is consistent across hand and great-toe series. The middle finger and great toe are the most exposed digits.
- Diagnostic delay is common worldwide, with up to a third of cases presenting or being treated late, driving the infection and osteomyelitis burden.
Side-by-side principles from major bodies
| Body / framework | Relevant principle | Implication for Seymour fracture |
|---|---|---|
| BOA / BAPRAS (UK) open fracture standards (BOAST) | Early antibiotics, prompt debridement, combined orthoplastic decision-making, definitive soft-tissue cover. | Treat the nail-bed-violating injury as a true open fracture: early antibiotics and timely washout, with nail-bed repair as the soft-tissue component. |
| AAOS / American hand and paediatric practice | Open physeal injuries warrant irrigation, debridement, reduction and antibiotics; most acute, stable injuries can be ED-managed. | Supports emergency-department management of stable acute injuries with first-generation cephalosporin cover and theatre for unstable or failed reductions. |
| AO Foundation (paediatric) | Respect the physis, achieve anatomical reduction, use minimal stable fixation (smooth K-wires) and avoid repeated physeal trauma. | Use smooth wires only when needed, avoid aggressive curettage across the physis and confirm reduction on a true lateral. |
| EFORT / European consensus thinking | Emphasis on infection prevention and recognition of the hidden open fracture. | High index of suspicion for the deceptive mallet-like presentation; nail-fold inspection is mandatory. |
High- versus limited-resource practice variation
| Element | High-resource setting | Limited-resource setting |
|---|---|---|
| Imaging | Dedicated true AP and lateral digit films, occasional MRI for suspected osteomyelitis. | Plain films only; rely heavily on clinical nail-fold inspection where imaging is scarce. |
| Theatre access | Day-case theatre with magnification and fine instruments available. | Wound care, debridement and nail-bed repair may be done under digital block in a procedure room; prioritise washout and antibiotics. |
| Fixation | Smooth K-wires readily available when unstable. | Suture-only stabilisation or careful splinting after reduction is a reasonable alternative when wires are limited. |
| Follow-up | Structured review for union, nail growth and physeal status. | Family education on infection warning signs becomes the critical safety net. |
The unifying message across every framework is identical: recognise the hidden open fracture, give early antibiotics, clear the soft-tissue block, repair the nail bed and protect the physis.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A ten-year-old presents after a door crush with a flexed distal phalanx and blood at the proximal nail fold. How do you manage this?”
“Closed reduction of a distal phalanx physeal fracture keeps springing back. What is the likely reason?”
“A child presents five days after a finger crush with swelling, redness and discharge at the nail fold, and the X-ray shows a distal phalanx physeal fracture. How does delay change your management?”
Recognise
- Child or adolescent
- Crush or ball injury
- Mallet-like DIP posture
- Blood at proximal nail fold
- Nail plate above eponychial fold
Image
- Dedicated digit AP
- True lateral is essential
- Physeal widening
- Salter-Harris I or II
- Juxta-epiphyseal fracture
Treat
- Analgesia
- Antibiotics
- Tetanus check
- Washout and debridement
- Remove interposed matrix
- Nail-bed repair
- K-wire if unstable
Do Not Miss
- Open fracture
- Germinal matrix interposition
- Osteomyelitis risk
- Nail deformity
- Physeal arrest