Stable vs Unstable | In Situ Pin | AVN Risk
LODER CLASSIFICATION (STABILITY)
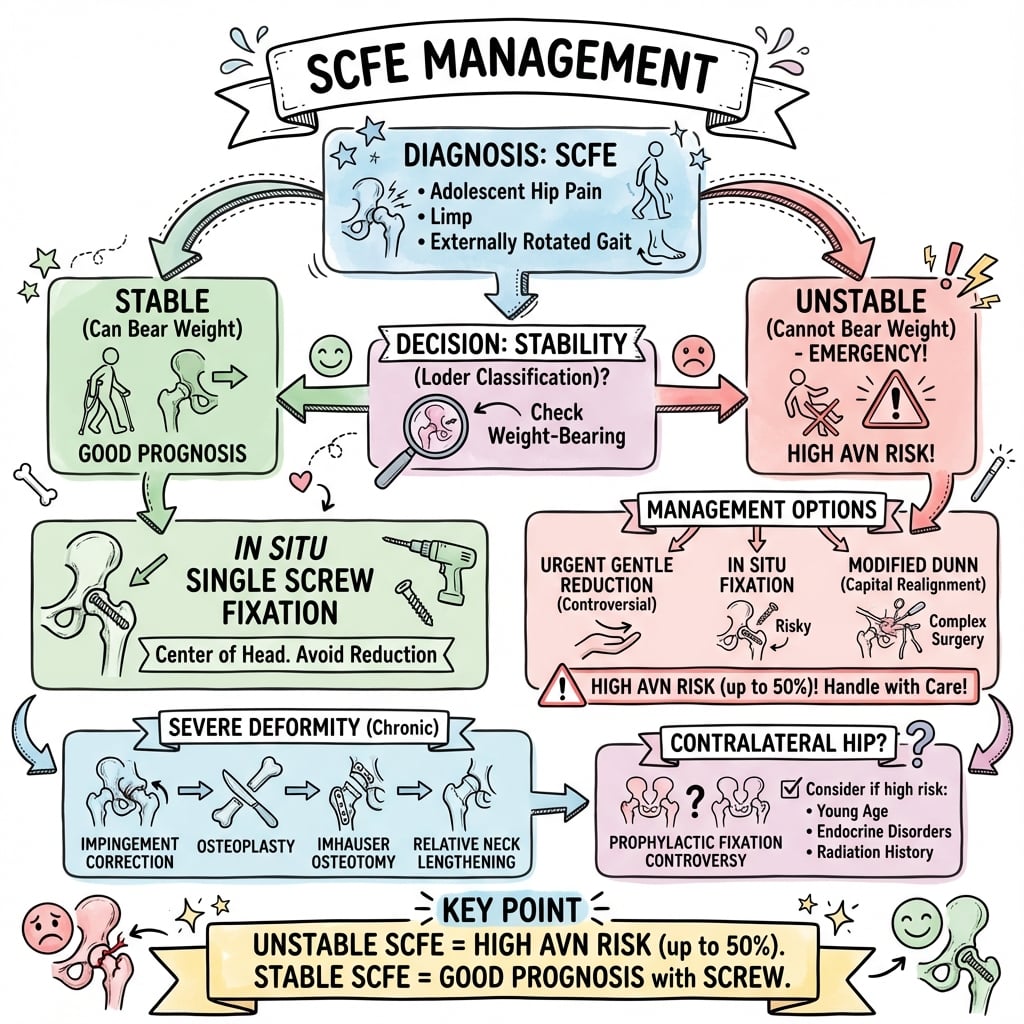
Critical Must-Knows
- Stable SCFE = can weight-bear. Unstable SCFE = cannot weight-bear
- IN SITU fixation - do NOT attempt reduction (AVN risk)
- Unstable SCFE has 47% AVN rate even with best treatment
- Contralateral prophylactic pinning: consider in high-risk patients
- Single central screw perpendicular to physis is gold standard
Clinical Pearls
- "Unstable = emergency surgery (within 24 hours)
- "Any attempt at reduction increases AVN dramatically
- "Southwick angle measures slip severity on frog lateral
- "Klein's line should intersect lateral epiphysis on AP
Clinical Imaging
Imaging Gallery



Critical Exam Concepts
Do NOT Reduce
In situ fixation is the rule. Any attempt to reduce increases AVN risk dramatically. Even unstable SCFE should be pinned in situ with only gentle positioning.
Stable vs Unstable
Loder Classification determines prognosis. Stable (can weight-bear): less than 1% AVN. Unstable (cannot weight-bear): 47% AVN. This is the most important prognostic factor.
Single Screw Technique
Single screw perpendicular to physis. Enter anterolateral femur, aim for center of epiphysis. Screw should be central and perpendicular. Multiple screws add AVN risk without benefit.
Contralateral Hip
20-40% bilateral risk. Consider prophylactic pinning if high-risk (younger, endocrine disorder, renal disease, hypothyroid). Discuss with family.
Stable vs Unstable SCFE Comparison
| Feature | Stable SCFE | Unstable SCFE |
|---|---|---|
| Weight-bearing | Able to walk with/without crutches | Unable to walk even with crutches |
| AVN Risk | Less than 1% | 47% |
| Timing | Semi-urgent (within days) | Emergency (within 24 hours) |
| Treatment | In situ screw | In situ screw (gentle positioning) |
| Prognosis | Excellent | Guarded (high AVN risk) |
FAT HIPSCFE Risk Factors
| F | Fat (obesity) Most common risk factor |
| A | Adolescence Growth spurt, weak physis |
| T | Thyroid (hypothyroid) Endocrine disorders |
| H | Hypogonadism Hormonal imbalance |
| I | Island populations (African, Pacific) Higher incidence |
| P | Physis weakness/Renal disease Renal osteodystrophy weakens physis |
| F | Fat (obesity) Most common risk factor | T | Thyroid (hypothyroid) Endocrine disorders | I | Island populations (African, Pacific) Higher incidence |
| A | Adolescence Growth spurt, weak physis | H | Hypogonadism Hormonal imbalance | P | Physis weakness/Renal disease Renal osteodystrophy weakens physis |
Hook:FAT HIP - the fat hip is at risk of slipping!
SCREWSCFE in situ Fixation Principles
| S | Single screw One screw prevents additional AVN risk |
| C | Central placement Center of epiphysis on both views |
| R | Right angles to physis Perpendicular for maximum purchase |
| E | Enter lateral (anterolateral) Lateral cortex entry point |
| W | Within center - no joint penetration Avoid articular surface |
| S | Single screw One screw prevents additional AVN risk | E | Enter lateral (anterolateral) Lateral cortex entry point |
| C | Central placement Center of epiphysis on both views | W | Within center - no joint penetration Avoid articular surface |
| R | Right angles to physis Perpendicular for maximum purchase |
Hook:Get the SCREW right - single, central, perpendicular!
PYREContralateral Prophylaxis Indications
| P | Prepubertal/Young age More growth remaining = higher risk |
| Y | Years of growth remaining Open physis on contralateral |
| R | Renal disease or endocrine disorder Metabolic causes bilateral |
| E | Expected compliance issues If difficult follow-up |
| P | Prepubertal/Young age More growth remaining = higher risk | R | Renal disease or endocrine disorder Metabolic causes bilateral |
| Y | Years of growth remaining Open physis on contralateral | E | Expected compliance issues If difficult follow-up |
Hook:Set a PYRE - burn the contralateral hip risk with prophylaxis!
Overview and Epidemiology
Pathophysiology
SCFE occurs through the hypertrophic zone of the physis (weakest zone). The epiphysis is held by the acetabulum. The metaphysis slips anteriorly and externally rotates relative to the epiphysis. Mechanical overload (obesity) and hormonal factors (growth spurt, endocrine) weaken the physis.
Epidemiology
- Peak age: 10-16 years (during growth spurt)
- Male to female 2-3:1 (males later puberty)
- Boys: mean 12-13 years
- Girls: mean 11-12 years
- Higher in African American, Pacific Islander populations
Risk Factors
- Obesity (most common)
- Rapid growth (tall for age)
- Endocrine: hypothyroidism, GH abnormalities
- Renal osteodystrophy
- Radiation therapy (previous)
- Retroversion of femoral head
Anatomy and Biomechanics
Blood Supply Considerations
The retinacular vessels (from MFCA) are the primary blood supply to the femoral head. They run along the posterior-superior femoral neck. Any manipulation, reduction attempt, or surgical dissection risks disrupting these vessels and causing AVN.
Proximal Femoral Physis
The physis is the weak point: The slip occurs through the hypertrophic zone of the physis (zone of provisional calcification is weakest).
Direction of slip: The epiphysis stays in the acetabulum. The metaphysis (and shaft) slips anteriorly and externally rotates. This creates the classic clinical finding of external rotation contracture.
Periosteal sleeve: The posterior periosteum remains attached to the epiphysis, containing the retinacular vessels.
Classification Systems
Loder Classification (Stability) - MOST IMPORTANT
| Classification | Definition | AVN Risk | Urgency |
|---|---|---|---|
| Stable | Can weight-bear (with or without crutches) | Less than 1% | Days |
| Unstable | Cannot weight-bear even with support | 47% | Hours (emergency) |
Most important classification for prognosis. The stability (ability to weight-bear) is the single best predictor of AVN.
Clinical Assessment
History
- Groin, thigh, or knee pain (referred)
- Limp (abductor or antalgic gait)
- Duration of symptoms
- Able to weight-bear? (critical question)
- Endocrine or metabolic history
- Family history of SCFE
Examination
- Obligate external rotation with hip flexion
- Loss of internal rotation
- Short limb (if severe slip)
- Trendelenburg gait
- Check contralateral hip
- BMI and body habitus
Obligate External Rotation
The classic sign: when you flex the hip, it obligatorily externally rotates. This is because the metaphysis has slipped anteriorly relative to the epiphysis. Flexion drives the neck against the anterior acetabulum, forcing external rotation.
Knee Pain in an Adolescent = Hip X-ray
Referred pain to the knee is common in SCFE. Any adolescent with hip, thigh, OR knee pain should have hip X-rays. Missing a SCFE presenting as knee pain is a classic medicolegal pitfall.
Investigations
Radiological Investigations
| View | Key Findings | Measurement |
|---|---|---|
| AP Pelvis | Klein's line disruption | Line along superior neck should intersect epiphysis |
| Frog Lateral | Posterior slip visible | Southwick angle (severity) |
| Cross-table lateral | Alternative if frog lateral painful | Same findings |
Klein's line: On AP, a line along the superior border of the femoral neck should intersect the lateral portion of the epiphysis. If it does not, the epiphysis has slipped.
Management
In Situ Fixation - Do NOT Reduce
The single most important principle: Fix the slip in situ. ANY attempt at reduction - whether open or closed - significantly increases AVN risk. Even in severe slips, in situ fixation followed by deformity correction later is safer than reduction.
Stable SCFE Management
Timing: Semi-urgent (within days). Patient should be non-weight-bearing until surgery.
Treatment: In situ single screw fixation.
Technique: Single partially threaded (6.5mm or 7.0mm) cannulated screw. Enter from anterolateral femur. Aim for center of epiphysis on both views. Screw should be perpendicular to physis and engage center of epiphysis.
Post-op: Weight-bear as tolerated. Physis will close over 6-12 months.
Single vs Multiple Screws
Single screw is sufficient for most SCFE. Multiple screws add AVN risk without improving stability. The exception may be an unstable SCFE where additional fixation is considered, but even then, many surgeons use single screw.
Surgical Technique Considerations
In Situ Single Screw Fixation
Position: Supine on fracture table with fluoroscopy.
Entry point: Anterolateral femur, below vastus lateralis ridge. Entry should BE in line with center of epiphysis on lateral view.
Screw trajectory: Aim for center of epiphysis on both AP and lateral. Screw should be perpendicular to physis (parallel to the slip direction correction if it were to occur). At least 5 threads should cross the physis into epiphysis.
Critical: Check no joint penetration on frog lateral (hip flexed and externally rotated). Screw tip should be greater than 5mm from articular surface.
Complications
Complications of SCFE and Treatment
| Complication | Cause | Prevention/Treatment |
|---|---|---|
| AVN (most feared) | Reduction attempt, unstable SCFE | In situ fixation, no reduction |
| Chondrolysis | Screw penetration, unknown | Avoid joint penetration, check fluoro |
| Slip progression | Inadequate fixation, missed diagnosis | Secure screw placement |
| FAI | Residual deformity (cam lesion) | Later osteoplasty or osteotomy |
| Contralateral slip | Natural history (20-40%) | Prophylactic pinning if high-risk |
| Hardware complications | Screw prominence, backout | Bury screw head, check fixation |
AVN Rates
Stable SCFE: Less than 1% AVN with in situ pinning. Unstable SCFE: 47% AVN even with in situ pinning (due to initial blood supply disruption). With reduction attempt: AVN rates increase dramatically (up to 100% in some series).
Postoperative Care
Post-Operative Protocol
Wound check. Mobilize weight-bearing as tolerated (stable SCFE). Non-weight-bearing for few days if unstable SCFE.
Wound check. X-ray to confirm screw position. Advance mobility.
X-ray to assess physeal closure. Most begin to close by 3-6 months.
Confirm complete physeal closure. Usually no screw removal needed.
Monitor for AVN (if unstable SCFE). Assess for FAI symptoms. Check contralateral hip until skeletal maturity.
Outcomes and Prognosis
Prognosis Based on Stability
Stable SCFE: Excellent prognosis. Less than 1% AVN. Most return to full activity. Long-term concern is FAI from residual deformity.
Unstable SCFE: Guarded prognosis. 47% develop AVN. Even those without AVN may have compromised hip function. Close monitoring required.
Special Considerations
Management of Severe SCFE
Severe slips (greater than 50-60°) create significant deformity leading to FAI and early OA.
Options: In situ pinning remains safest. Address residual deformity later with:
- Femoral neck or subcapital osteotomy (high AVN risk)
- Intertrochanteric osteotomy (Imhauser - safer)
- Cam osteoplasty (arthroscopic or open)
Most surgeons prefer in situ pin and later osteoplasty rather than acute realignment.
Evidence Base and Key Studies
Loder et al. - Landmark Stability Classification
- 55 hips presenting acutely (symptoms under 3 weeks) reclassified by physeal stability
- 30 unstable (cannot weight-bear even with crutches), 25 stable (can weight-bear)
- AVN developed in 14 of 30 unstable hips (47%) and 0 of 25 stable hips
- No demonstrable association between early reduction and AVN in this series
Aronsson & Loder - Treatment of the Unstable Slip
- Treatment priorities: avoid AVN, avoid chondrolysis, prevent further slip, then correct deformity
- Manipulative reduction and acute corrective osteotomy NOT recommended (high AVN/chondrolysis)
- Recommends preoperative bed rest to settle synovitis, then stabilisation with a single central screw
- Careful positioning on the fracture table may give incidental reduction - no active manipulation
Lehmann et al. - Epidemiology Update
- Overall US incidence 10.8 per 100,000 children aged 9-16 years (Kids' Inpatient Database)
- Incidence 3.94x higher in Black and 2.53x higher in Hispanic children vs White children
- Higher in boys (13.4/100,000) than girls (8.1/100,000)
- Seasonal and latitude variation suggests environmental contribution
Tannast/Ziebarth et al. - Modified Dunn (Bernese)
- Modified Dunn via surgical hip dislocation with a retinacular soft-tissue flap protecting the MFCA
- AVN rate at the inventor institution approximately 2% - far lower than historical open reduction
- AVN occurred only where no head perfusion was evident before reduction
- Other centres report AVN up to 24% during their early learning curve
Ziebarth et al. - Modified Dunn 10-Year Outcomes
- 43 hips (mild to severe slips) treated with modified Dunn, 98% available at minimum 10 years
- Cumulative survivorship 93% at 10 years (95% CI 85-100%)
- No hips showed AVN on plain radiographs at follow-up
- Secondary impingement persisted in some hips; 14% needed further surgery for impingement
Lindell et al. - Prophylactic Fixation Algorithm
- National cohort of 379 children with SCFE (2007-2013)
- Chronological age was the only independent predictor of a subsequent contralateral slip
- Using age under 13 years as the threshold: sensitivity 88%, specificity 51% for preventing contralateral slip
- Triradiate cartilage assessment had poor inter-observer agreement and was unreliable
Ziebarth/Leunig et al. - Cartilage Damage & Perfusion
- 119 SCFE hips assessed at open surgery; acetabular cartilage damage in 97 of 109 (89%)
- Cam impingement from the slip - not slip angle alone - drives acetabular cartilage damage
- In disconnected (unstable) epiphyses, perfusion loss increased with longer time to surgery
- Posterior callus resection improved laser-Doppler epiphyseal perfusion
Loder - Controversies in SCFE
- Frames the four enduring controversies: unstable slip management, role of osteotomy, contralateral prophylaxis, fixation in the very young
- Reduction of the unstable slip remains contentious because of AVN risk
- Decision analysis is needed to weigh prophylactic fixation against expectant follow-up
- Implant choice in young children must allow continued growth
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Classic Stable SCFE
"A 13-year-old obese boy presents with 3 weeks of left groin and thigh pain. He is able to walk with a limp. Examination shows obligate external rotation with hip flexion and loss of internal rotation. X-rays show a SCFE with Southwick angle 35 degrees. How would you manage this?"
Scenario 2: Unstable SCFE
"A 12-year-old girl presents with sudden onset left hip pain after a minor fall. She is unable to weight-bear. The leg is held in external rotation and she screams with any hip movement. X-rays show a significantly displaced SCFE. How would you manage this?"
Scenario 3: Bilateral SCFE
"A 10-year-old boy with known hypothyroidism presents with new right hip pain. He had a left SCFE pinned 6 months ago. X-rays show a new right SCFE. How would you manage this, and what would you do differently if asked at the time of the first SCFE?"
MCQ Practice Points
Stability Classification Question
Q: What is the key factor in the Loder classification of SCFE? A: Ability to weight-bear. Stable = able to walk (with or without crutches). Unstable = unable to walk. This is the most important prognostic factor.
AVN Rate Question
Q: What is the AVN rate in unstable SCFE and stable SCFE? A: Unstable: 47%. Stable: less than 1%. The difference is due to initial disruption of retinacular blood supply in unstable SCFE.
Treatment Principle Question
Q: What is the principle of SCFE treatment that minimizes AVN risk? A: In situ fixation without reduction. Any attempt at reduction (open or closed) dramatically increases AVN risk.
Screw Technique Question
Q: What is the ideal screw position for SCFE fixation? A: Single screw, central in epiphysis on both views, perpendicular to physis. Multiple screws increase AVN risk without added benefit.
Klein's Line Question
Q: What is Klein's line and what does an abnormal finding indicate? A: A line along the superior border of the femoral neck on AP view. Normally intersects the lateral epiphysis. If it does NOT, the epiphysis has slipped.
Bilateral Risk Question
Q: What is the risk of contralateral SCFE and when should prophylactic pinning be considered? A: 20-40% bilateral risk. Consider prophylaxis if: young age, endocrine disorder, renal disease, compliance issues, or physeal widening.
Guidelines, Registries & Global Practice
Global Epidemiology
- Overall incidence approximately 10-11 per 100,000 children aged 9-16 years (US data); regional rates range widely
- Boys affected more than girls (roughly 13 vs 8 per 100,000); peak at the adolescent growth spurt
- Markedly higher in children of African and Pacific Islander ancestry; lowest in East Asian populations
- Incidence rising in parallel with childhood obesity worldwide
- Bilateral disease in 18-50% across series, clustering in younger and endocrine/renal patients
Registry & Cohort Signals
- No dedicated SCFE arthroplasty registry; signal comes from national paediatric cohorts (e.g. Swedish, Norwegian) and KID database
- National cohorts identify younger chronological age as the dominant contralateral-slip risk factor
- Long-term cohorts confirm cam-FAI and early osteoarthritis as the principal late burden, including in mild slips
- Modified Dunn durability data come from single expert centres, not population registries
Guideline & Society Positions (Side by Side)
| Theme | Common ground (AAOS / BOA-BSCOS / AO / EFORT consensus) | Where practice genuinely varies |
|---|---|---|
| Diagnosis | AP plus frog-leg (or cross-table) lateral pelvis; treat knee/thigh pain in an adolescent as a hip until excluded | Threshold for MRI to detect a pre-slip or assess perfusion |
| Definitive treatment | In situ fixation is the default for stable and most unstable slips; avoid forced reduction | Single vs two screws for unstable slips; cannulated screw vs smooth pins in the very young |
| Unstable slip timing | Urgent stabilisation; non-weight-bearing until theatre | Emergency within 24h vs planned-urgent after synovitis settles (capsular decompression debated) |
| Severe deformity | Address symptomatic cam-FAI; protect the MFCA blood supply | Modified Dunn (capable centres) vs intertrochanteric (Imhauser) osteotomy vs osteochondroplasty |
| Contralateral hip | Counsel on bilateral risk; monitor to skeletal maturity | Routine prophylactic fixation under age 13 vs selective (endocrine/renal/young) vs watchful waiting |
High- vs Limited-Resource Practice
Well-Resourced Settings
- Reliable fluoroscopy and cannulated screw systems; in situ pinning routine and same-admission
- Access to hip-preservation expertise for modified Dunn and arthroscopic/open osteochondroplasty
- MRI available to assess perfusion or a pre-slip when indicated
Limited-Resource Settings
- Late and chronic presentation more common, so severe deformity and established FAI predominate
- Limited image intensifier access shifts some toward open techniques or threaded pins
- Endocrine/renal screening and long-term FAI surveillance may be incomplete
- Prophylactic contralateral fixation favoured where follow-up is unreliable
Differential Diagnosis
The Limping / Hip-Pain Adolescent
Differentiating SCFE from Mimics
| Condition | Typical age / patient | Discriminating features | Key investigation |
|---|---|---|---|
| SCFE | 10-16y, often obese, growth spurt | Obligate external rotation on flexion, loss of internal rotation, knee/thigh pain | AP + frog-leg lateral pelvis (Klein line, Southwick angle) |
| Perthes disease | 4-9y, often smaller/thin | Insidious limp, younger child, lateral pillar changes | AP + frog-leg radiographs; MRI early |
| Septic arthritis | Any age, systemic upset | Fever, refusal to weight-bear, raised CRP/ESR/WCC, exquisite pain on micro-movement | Joint aspiration; ultrasound; inflammatory markers |
| Transient synovitis | 3-8y, recent viral illness | Well child, settles in days, mild markers | Diagnosis of exclusion after septic ruled out |
| Femoral neck stress fracture | Athletic adolescent, RED-S/female athlete | Activity-related groin pain, normal early X-ray | MRI |
| Apophysitis / avulsion | Adolescent athlete | Pain at AIIS/ischial apophysis, mechanism of sprint/kick | AP pelvis; oblique views |
The Two Cannot-Miss Mimics
A febrile, systemically unwell child who cannot weight-bear is septic arthritis until proven otherwise - aspirate, do not just X-ray. And remember the reverse trap: a well adolescent with isolated knee pain may have a SCFE - always image the hip.
Controversies & Areas of Uncertainty
Reduction of the Unstable Slip
The classical doctrine is in situ fixation with no forced reduction. Modified Dunn series suggest anatomical realignment with low AVN is achievable, but only in expert centres - elsewhere AVN climbs steeply. There is no randomised comparison, so the safe default outside high-volume units remains in situ pinning.
Capsular Decompression
Some argue urgent decompression of the tense haemarthrosis in unstable slips lowers AVN by relieving tamponade of the retinacular vessels; evidence is conflicting and it is not universally adopted.
Prophylactic Contralateral Fixation
Cohort data point to chronological age (under 13) as the strongest predictor, supporting a low threshold in younger children, but routine bilateral fixation risks unnecessary surgery in those who would never slip. Decision remains shared and individualised.
Timing of the Unstable Slip
Emergency stabilisation within 24 hours versus deliberately waiting for synovitis to settle is debated; AVN is driven largely by the initial vascular insult, which surgical timing may only partly influence.
SLIPPED CAPITAL FEMORAL EPIPHYSIS
Clinical summary
Key Facts
- •Peak age 10-16 years
- •Obesity is main risk factor
- •20-40% bilateral risk
- •Knee pain = get hip X-ray
Loder Classification
- •Stable = can weight-bear
- •Unstable = cannot weight-bear
- •Stable: less than 1% AVN risk
- •Unstable: 47% AVN risk
Treatment Principles
- •IN SITU fixation - do NOT reduce
- •Single screw, central, perpendicular
- •Unstable = emergency (24h)
- •Stable = semi-urgent (days)
Radiographic Signs
- •Klein's line disruption (AP)
- •Posterior slip on frog lateral
- •Southwick angle (severity)
- •Physeal widening (early sign)
Prophylactic Pinning
- •Young age at presentation
- •Endocrine disorder
- •Renal osteodystrophy
- •Physeal widening contralateral