Superior Labrum Anterior to Posterior | Biceps Anchor | Type II Critical
SLAP CLASSIFICATION (Snyder)
Critical Must-Knows
- Type II is the CLINICALLY SIGNIFICANT SLAP tear - biceps anchor is detached
- O-Brien test and Speed test are key provocative tests
- Overhead athletes (throwers) are high-risk population
- SLAP repair outcomes declining in literature - tenotomy/tenodesis rising
- Age over 40: consider biceps tenotomy/tenodesis over SLAP repair
Clinical Pearls
- "MR arthrography is gold standard for SLAP diagnosis
- "Peel-back test: arthroscopic confirmation (ABER position)
- "High failure rate of SLAP repair in throwing athletes
- "Type II can be subdivided: anterior, posterior, combined
Clinical Imaging
Imaging Gallery




Critical Exam Concepts
Type II is KEY
Type II SLAP = biceps anchor detached. This is the clinically significant lesion. Types I and III can be debrided. Type IV involves biceps tendon itself.
Overhead Athletes
Throwers have posterosuperior SLAP tears from peel-back mechanism in late cocking. Often associated with GIRD (glenohumeral internal rotation deficit) and posterior capsular tightness.
SLAP Repair Declining
Recent literature shows high failure rates of SLAP repair, especially in patients over 40. Trend toward biceps tenotomy or tenodesis with comparable outcomes and faster recovery.
Age Matters
Under 40: Consider SLAP repair in motivated patient. Over 40: Biceps tenotomy or tenodesis preferred. Degenerative labral changes common over 40.
Quick Decision Guide
| SLAP Type | Pathology | Treatment | Role of Biceps |
|---|---|---|---|
| Type I | Degenerative fraying | Debridement only | Anchor intact - leave |
| Type II | Biceps anchor detached | Repair or biceps procedure | Anchor must be addressed |
| Type III | Bucket handle tears | Excise bucket handle | Anchor intact - leave |
| Type IV | Bucket handle into biceps | Excise +/- repair or tenotomy | Biceps tendon involvement |
| Type V-X | Combined lesions | Address each component | Variable - case dependent |
FBBBSLAP Classification
| F | Fraying Type I - degenerative fraying |
| B | Biceps anchor detached Type II - most important |
| B | Bucket handle Type III - displaced labrum |
| B | Biceps tendon split Type IV - bucket into biceps |
| F | Fraying Type I - degenerative fraying | B | Bucket handle Type III - displaced labrum |
| B | Biceps anchor detached Type II - most important | B | Biceps tendon split Type IV - bucket into biceps |
Hook:FBBB - Know Type II (Biceps anchor) is the KEY clinical SLAP!
SOAPSLAP Clinical Tests
| S | Speed test Resisted forward flexion with extended elbow |
| O | O-Brien test Forward flexion, adduction, IR then ER |
| A | Anterior slide Hand on hip, forward/upward force |
| P | Peel-back sign Arthroscopic ABER detachment |
| S | Speed test Resisted forward flexion with extended elbow | A | Anterior slide Hand on hip, forward/upward force |
| O | O-Brien test Forward flexion, adduction, IR then ER | P | Peel-back sign Arthroscopic ABER detachment |
Hook:SOAP up the shoulder tests for SLAP diagnosis!
AGESLAP Repair vs Biceps Procedure Decision
| A | Age under 40 Consider SLAP repair if motivated |
| G | Gross biceps pathology Tenotomy/tenodesis if tendon degenerative |
| E | Expectations Throwers may not return to prior level |
| A | Age under 40 Consider SLAP repair if motivated |
| G | Gross biceps pathology Tenotomy/tenodesis if tendon degenerative |
| E | Expectations Throwers may not return to prior level |
Hook:AGE guides SLAP repair vs biceps procedure decision!
Overview and Epidemiology
Declining SLAP Repair Rates
SLAP repairs peaked then declined in the 2000s-2010s as studies showed high failure rates, especially in patients over 40 and throwers. Trend now toward biceps tenotomy or tenodesis which provides reliable pain relief with faster recovery.
Epidemiology
- Originally described in 1990 (Snyder)
- Peak age 26-50 years
- Male greater than female
- Overhead athletes overrepresented
- Increasing diagnosis with MRI/arthroscopy
Mechanism
- Compression: Fall on outstretched hand, arm forward and abducted
- Traction: Sudden pulling force on arm
- Peelback: Throwing motion (late cocking) in throwers
- Degenerative: Age-related in Type I
- Repetitive overhead: Cumulative microtrauma
Pathophysiology and Mechanisms
Superior Labral Anatomy
Location: 10 o-clock to 2 o-clock position on glenoid.
Biceps anchor: LHB tendon inserts at supraglenoid tubercle, blending with superior labrum.
Meniscoid appearance: Less firmly attached than anterior labrum - may appear loose on arthroscopy.
Blood supply: Relatively avascular zone (10-12 o-clock) - limits healing.
Distinguish SLAP from Normal Variants
Sublabral foramen (absent anterosuperior labrum) and Buford complex (cord-like MGHL) are normal variants that should NOT be repaired. True SLAP tears show: fraying, instability of biceps anchor, extension toward biceps, and positive peel-back test.
Classification Systems
Original Snyder Classification (Types I-IV)
| Type | Pathology | Treatment | Key Point |
|---|---|---|---|
| I | Fraying of superior labrum | Debridement | Anchor intact - no repair |
| II | Biceps anchor detached from glenoid | Repair or biceps procedure | MOST IMPORTANT clinically |
| III | Bucket handle tear of labrum | Excise bucket handle | Anchor intact - preserve it |
| IV | Bucket handle extending into LHB | Excise +/- repair/tenotomy | Biceps tendon split |
Clinical Assessment
History
- Mechanism: Compression, traction, throwing
- Pain: Anterior/deep shoulder, with overhead activity
- Clicking/popping: Common complaint
- Sport level: Overhead athlete critical
- Weakness: May report with overhead activity
Examination
- O-Brien test: Pain with forward flex/adduct/IR, relieved with ER
- Speed test: Resisted forward flexion
- Anterior slide: Hand on hip, force applied
- Biceps load test: ABER with biceps contraction
- GIRD: Check internal rotation deficit
O-Brien Test (Active Compression Test)
Arm at 90° forward flexion, 10-15° adduction, thumb down (IR). Resist downward pressure. Then repeat with palm up (ER). Positive: Pain with IR, relieved with ER. Most commonly used clinical test for SLAP.
Key Examination Findings
Overhead athletes: Check for GIRD (internal rotation deficit greater than 20° compared to opposite side), posterior capsular tightness, scapular dyskinesis.
Combined pathology: SLAP tears often associated with rotator cuff pathology - assess thoroughly.
Differential Diagnosis
The "deep anterior shoulder pain with overhead activity" presentation overlaps with several conditions. No single SLAP test is reliable in isolation, so the differential must be worked through clinically and on imaging.
Differential Diagnosis of Suspected SLAP Tear
| Condition | Discriminating Features | Best Test |
|---|---|---|
| Biceps (LHB) tendinopathy | Pain over bicipital groove, point tender, Speed/Yergason positive | Ultrasound or MRI of groove; diagnostic LHB block |
| Rotator cuff tear / tendinopathy | Painful arc, weakness on cuff testing, night pain | MRI; often coexists with SLAP |
| Internal (posterosuperior) impingement | Posterior pain in late cocking, GIRD, throwers | ABER MR arthrography; arthroscopy |
| Anterior instability / Bankart | Apprehension, prior dislocation, relocation positive | MR arthrography (anteroinferior labrum) |
| AC joint pathology | Point tenderness over AC joint, cross-body pain | Targeted exam, AC joint injection |
| Normal variant (sublabral foramen / Buford) | No fraying, stable biceps anchor, asymptomatic | Arthroscopic recognition - do NOT repair |
Investigations
MR Arthrography (Gold Standard)
Sensitivity: 82-98% for Type II SLAP.
Technique: Intra-articular gadolinium increases labral visualization.
Key findings: Contrast extension between labrum and glenoid at superior labrum.
ABER sequence: Increases sensitivity for peel-back lesions.
Superior to standard MRI for labral pathology.
Peel-Back Test
Arthroscopic ABER positioning: With arm in abduction and external rotation (throwing position), the biceps vector becomes vertical and peels the posterosuperior labrum off the glenoid. Positive peel-back = Type II SLAP (especially IIB in throwers).
Management Algorithm
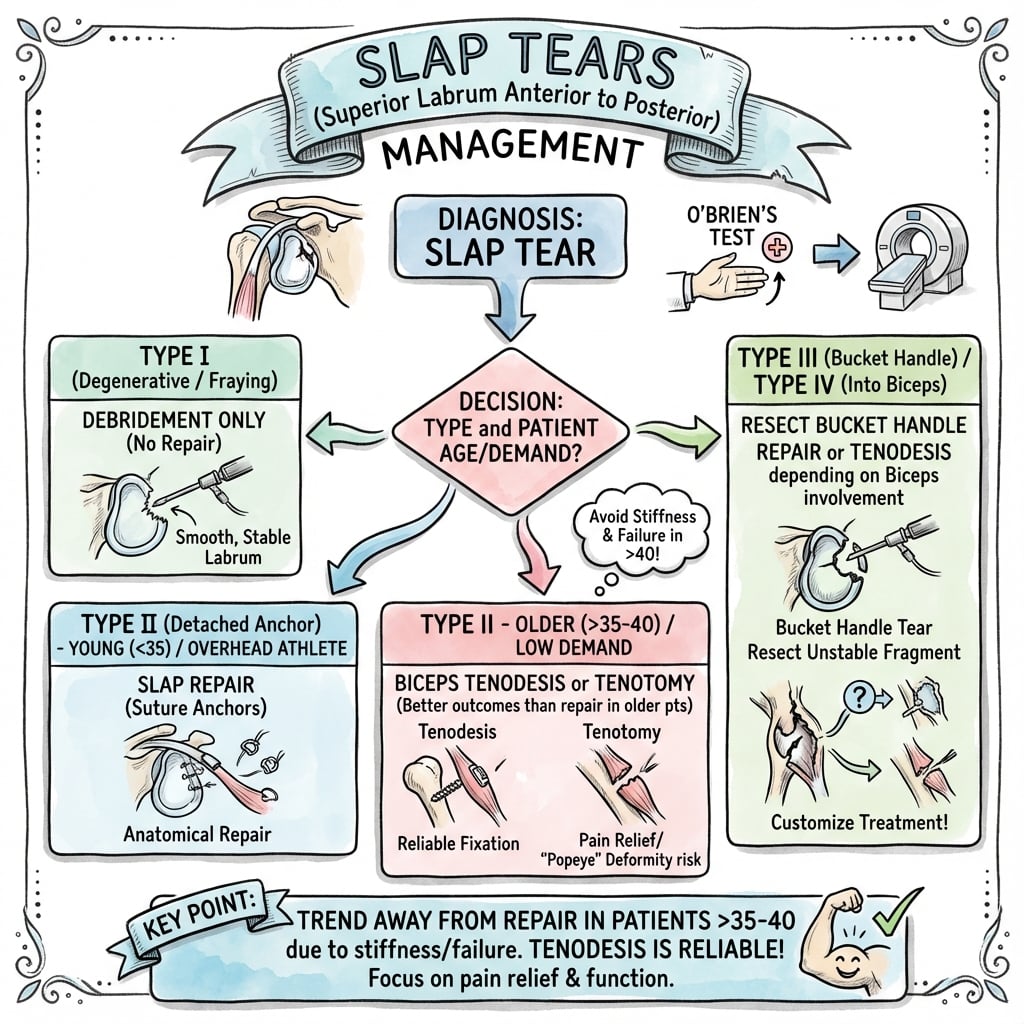
SLAP Type-Based Treatment
Decision Pathway
Degenerative fraying. Anchor intact. Simple debridement of frayed tissue. No repair needed.
Biceps anchor detached. Options: SLAP repair (under 40, motivated), biceps tenotomy (over 40, low demand), or tenodesis (over 40, active).
Bucket handle tear. Anchor intact. Excise the displaced bucket handle fragment. Preserve the anchor.
Bucket handle into biceps. If less than 30% biceps involvement: excise bucket handle. If greater than 30%: biceps tenotomy or tenodesis.
Surgical Technique
Arthroscopic SLAP Repair
Surgical Steps
Confirm SLAP classification. Perform peel-back test. Assess biceps tendon quality.
Debride frayed tissue. Decorticate glenoid rim to bleeding bone. Mobilize the labrum.
1-3 suture anchors at superior glenoid rim. Place at 10-11 o-clock and 12-1 o-clock. Avoid suprascapular nerve on superior anchor.
Pass sutures through labrum. Tie to restore labral bumper and biceps anchor stability.
Anchor Positioning
Avoid placing anchors too posterior (risk suprascapular nerve at spinoglenoid notch) or too medial on glenoid neck (inadequate purchase). Anchors should be on the glenoid rim at the articular margin.
Complications
| Complication | Procedure | Incidence | Management |
|---|---|---|---|
| Stiffness | SLAP repair | Common | Aggressive PT, avoid in throwers |
| Persistent symptoms / failure | SLAP repair | Common in throwers | Revision or biceps procedure |
| Popeye deformity | Tenotomy | ~23% (vs ~7% tenodesis) | Cosmetic - counsel preop |
| Nerve injury | Repair | Rare | Avoid superior/posterior anchor |
| Persistent pain | Any | Variable | Address all pathology, consider revision |
SLAP Repair Failure in Throwers
Overhead throwing athletes return unreliably after SLAP repair. In a systematic review (Thayaparan 2019), pitchers returned to sport at only 57.5% versus 87.1% for non-pitching athletes. Peel-back forces during late cocking stress the repair. Many surgeons now favour biceps tenodesis for throwers with Type II SLAP.
Postoperative Care
Rehabilitation Protocol (SLAP Repair)
Sling immobilization. Elbow/hand exercises. Gentle pendulums only. No active biceps.
Wean sling. Passive to active-assisted ROM. Avoid ABER position. No resisted biceps.
Full AROM. Isometric cuff strengthening. Begin light biceps activity.
Progressive resistance. Sport-specific training. No throwing until 6 months minimum.
Tenotomy/Tenodesis Recovery
Biceps procedures have faster recovery. Tenotomy: sling 1-2 weeks, no restrictions by 6 weeks. Tenodesis: protect biceps 6 weeks, no heavy biceps loading 3 months. Both return to full activity faster than SLAP repair.
Outcomes and Prognosis
Procedure-Specific Outcomes
SLAP Repair: Overall return to sport around 70% (Thayaparan 2019), but pitchers return at only ~58%. Outcomes are poorer in throwers, older patients, and workers-compensation cases. Postoperative stiffness is the most common concern.
Biceps Tenotomy vs Tenodesis: Level I evidence (Belk 2021) shows equivalent pain and functional scores; cosmetic (Popeye) deformity is the key difference - 23.3% after tenotomy versus 6.8% after tenodesis.
Biceps Tenodesis: Comparable pain relief to tenotomy with a much lower cosmetic deformity rate; preferred in younger, active, or cosmetically concerned patients, and an effective salvage for failed SLAP repair (McCormick 2014, Boileau 2009).
Return to Sport
SLAP repair: 6-9 months for non-throwing sports. Throwing athletes may take 9-12 months with variable return to prior level.
Biceps procedures: Often faster return (3-4 months).
Controversies and Areas of Uncertainty
Repair vs primary tenodesis in the young
The biggest unresolved question. Registry data show a clear practice shift to tenodesis, and Boileau (2009) reported far better sport return after tenodesis - but his tenodesis group was older, confounding the comparison. Whether a motivated patient under 30 with an isolated Type II tear does better with repair (preserving native anatomy) or primary tenodesis remains unsettled.
Does the LHB anchor matter functionally?
The biomechanical role of the biceps anchor in glenohumeral stability is debated. If its contribution is minor, sacrificing it (tenotomy/tenodesis) carries little functional cost - which would favour the move away from repair. Cadaveric and clinical data remain conflicting.
Over-diagnosis on MRI/arthroscopy
Superior labral signal and a meniscoid attachment are common in asymptomatic shoulders and increase with age. A "SLAP" seen on imaging or scope is not necessarily the pain generator - over-treatment of normal variants and age-related change is a real risk.
Managing the throwing athlete
No approach reliably returns elite pitchers to prior performance. Whether to repair, add posterior capsular release for GIRD, or proceed directly to tenodesis is individualised and controversial, and honest counselling about uncertain return is essential.
Evidence Base and Key Studies
Original Description of SLAP Lesions (Snyder Classification)
- Retrospective review identifying 27 SLAP lesions among more than 700 shoulder arthroscopies
- Defined the four original types (I-IV); injury runs posterior to anterior including the biceps anchor
- Most common mechanism was a compression force from a fall onto an outstretched arm
- No preoperative imaging test reliably defined the lesion - diagnosis was arthroscopic
Declining SLAP Repair, Rising Biceps Tenodesis
- 619 SLAP repairs among 9,765 shoulder arthroscopies across four surgeons, 2004-2014
- Percentage of SLAP repairs fell significantly over the decade (P less than .001)
- Number and percentage of biceps tenodeses rose significantly over the same period
- Most SLAP repairs were performed for Type II tears; mean patient age fell over time
ABOS Database - Nationwide Decline in SLAP Repair
- 9,908 cases from the American Board of Orthopaedic Surgery part-II examination database, 2012-2017
- Significant decline in SLAP repair rate over the study period (P less than .001)
- Patients receiving biceps tenodesis were significantly more likely to be over 35 years
- SLAP repair remained concentrated in younger patients
Return to Sport After SLAP Repair (Pitchers Fare Worst)
- Systematic review of 22 studies, 944 patients undergoing arthroscopic SLAP repair
- Overall return to sport 69.6%; return to previous level of play 69.0%
- Mean time to return to sport 8.9 months
- Pitchers returned at only 57.5% versus 87.1% for non-pitching athletes
Biceps Tenodesis as Alternative to Type II SLAP Repair (Boileau)
- Cohort of 25 patients with isolated Type II SLAP lesions: 10 SLAP repair vs 15 biceps tenodesis
- Return to previous sport: 87% after tenodesis vs only 20% after SLAP repair (P = .01)
- 60% of repair patients were dissatisfied (persistent pain or failure to return to sport)
- Four failed SLAP repairs were successfully salvaged with subsequent biceps tenodesis
Biceps Tenodesis for Failed Type II SLAP Repair
- Prospective series of 42 patients undergoing open subpectoral tenodesis after a failed Type II SLAP repair
- Significant improvement in ASES, SANE and WOSI scores and in range of motion (P less than .0001)
- 81% returned to active duty and sport at mean 3.5-year follow-up
- Single transient musculocutaneous neurapraxia; mean patient age 39 years
Tenotomy vs Tenodesis - Cosmesis and Biomechanics (Hsu)
- Systematic review of clinical and biomechanical studies on biceps tenotomy versus tenodesis
- Higher incidence of cosmetic (Popeye) deformity after tenotomy than tenodesis
- Tenodesis associated with a higher likelihood of residual bicipital pain
- All included clinical studies were Level IV - no consensus could be reached on the superior technique
Tenotomy vs Tenodesis - Level I Meta-Analysis (Belk)
- Meta-analysis of 5 Level I randomised controlled trials, 468 patients (236 tenodesis, 232 tenotomy)
- Cosmetic deformity 6.8% after tenodesis vs 23.3% after tenotomy (P less than .001)
- No difference in Constant-Murley, VAS pain or ASES scores between groups
- Comparable complication and functional outcomes at mean 23-month follow-up
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Young Athlete with Shoulder Pain
"A 28-year-old recreational volleyball player presents with right shoulder pain during overhead serving. O-Brien test is positive. MR arthrography shows a Type II SLAP lesion with intact biceps tendon. How would you manage this?"
Scenario 2: Failed SLAP Repair
"A 35-year-old had SLAP repair 18 months ago but has persistent anterior shoulder pain with overhead activities. MRI shows the repair appears intact. What is your approach?"
Scenario 3: Throwing Athlete
"A 22-year-old elite baseball pitcher has posterior shoulder pain during the cocking phase of throwing. MR arthrography shows a posterosuperior Type IIB SLAP tear. Examination also reveals 25° GIRD. What is your treatment plan?"
MCQ Practice Points
Type II SLAP
Q: Which SLAP type is the most clinically significant? A: Type II - biceps anchor is detached from the glenoid. This requires surgical treatment (repair or biceps procedure). Types I and III can usually be debrided.
Type I Treatment
Q: How is a Type I SLAP treated? A: Debridement only. Type I is degenerative fraying with intact biceps anchor. No repair is needed - simply debride the frayed tissue.
Peel-Back Test
Q: What does a positive peel-back test indicate? A: Type II SLAP tear (especially Type IIB). In ABER position, the biceps vector becomes vertical and peels the posterosuperior labrum off the glenoid.
O-Brien Test
Q: How is the O-Brien test performed? A: Arm at 90° forward flexion, 10-15° adduction, thumb down (IR). Resist downward pressure. Repeat with palm up (ER). Positive: pain with IR, relieved with ER.
Sublabral Foramen
Q: What is the sublabral foramen? A: Normal anatomical variant - detachment of anterosuperior labrum at 1-3 o-clock position. Should NOT be repaired. Distinguished from SLAP by stable biceps anchor.
Age and SLAP Repair
Q: Why is SLAP repair less recommended in patients over 40? A: Degenerative labral and biceps changes reduce healing potential, and registry data (Cvetanovich 2020) show tenodesis is preferentially performed in patients over 35. Biceps tenotomy or tenodesis gives more reliable pain relief in this group.
Guidelines, Registries & Global Practice
Global Epidemiology
SLAP lesions account for a small proportion of all shoulder arthroscopies (around 6% in large series; Erickson 2016) but are over-represented in overhead athletes - baseball pitchers, volleyball and tennis players, swimmers and javelin throwers. Peak presentation is in active adults roughly 20-50 years, with a male predominance reflecting sport and occupational exposure. Isolated SLAP tears are uncommon; most coexist with rotator cuff or biceps pathology, particularly over 40, where degenerative superior labral change is frequently incidental.
Guidelines & Society Positions (Side by Side)
How Major Bodies Frame SLAP Management
| Body / Region | Emphasis | Practical Position |
|---|---|---|
| AAOS (US) | Evidence-based, shared decision-making | No isolated SLAP CPG; supports trial of non-operative care and procedure choice by age/demand |
| BOA / BESS (UK) | Stepwise, rehab-first | Physiotherapy and activity modification before surgery; tenodesis favoured in older patients |
| AO / arthroscopy societies | Technique and classification fidelity | Distinguish true SLAP from normal variants; address concomitant pathology |
| ESSKA / EFOST (Europe) | Athlete-centred | Individualised approach in throwers; caution about repair outcomes |
There is no dedicated randomised-trial-based clinical practice guideline specific to SLAP repair; recommendations are consensus- and cohort-driven. The consistent global theme across societies is a rehabilitation-first approach and a shift from labral repair toward biceps tenodesis, especially with increasing age.
Registry & Database Signals
- Surgeon practice databases (US): Both single-practice (Erickson 2016) and the nationwide ABOS examination database (Cvetanovich 2020) show a significant fall in SLAP repair volume and a rise in biceps tenodesis over the last decade, with tenodesis concentrated in patients over 35.
- SLAP repair has no implant-survivorship registry equivalent to arthroplasty (NJR / AOANJRR / SHAR); evidence comes from cohort series and the database trends above.
High- vs Limited-Resource Practice Variation
Well-resourced settings
- MR arthrography and ABER sequences readily available
- Arthroscopic repair, tenodesis and tenotomy all offered
- Structured sports-physiotherapy and return-to-throwing programmes
- Procedure choice driven by age, sport and patient preference
Limited-resource settings
- Diagnosis often clinical plus standard MRI or even plain films to exclude bony pathology
- Biceps tenotomy favoured - cheap, fast, no implants, minimal rehab burden
- Repair reserved for young high-demand athletes where anchors and rehab are accessible
- Greater reliance on activity modification and analgesia
Orthopaedic Exam Relevance
SLAP tears are a common viva topic. Know the Snyder classification (especially Type II), clinical tests (O-Brien, peel-back), and the global trend toward biceps tenotomy/tenodesis. Be prepared to discuss treatment in overhead athletes and why outcomes are variable.
SLAP TEARS
Clinical summary
Classification (Snyder I-IV)
- •Type I: Fraying - debride only
- •Type II: Biceps anchor detached - MOST IMPORTANT
- •Type III: Bucket handle - excise, anchor intact
- •Type IV: Bucket into biceps - excise +/- tenotomy
Clinical Tests (SOAP)
- •Speed test: Resisted forward flexion
- •O-Brien test: Forward flex/adduct/IR vs ER
- •Anterior slide: Hand on hip, force applied
- •Peel-back: Arthroscopic ABER position
Type II Decision Factors
- •Under 40: Consider SLAP repair
- •Over 40: Biceps tenotomy or tenodesis
- •Throwing athlete: High failure rate - consider tenodesis
- •Degenerative biceps: Tenotomy or tenodesis
Imaging
- •MR arthrography: Gold standard
- •Look for contrast at labral-glenoid junction
- •ABER sequence increases sensitivity
- •Peel-back test confirms at arthroscopy
Outcomes
- •SLAP repair: ~70% return to sport overall
- •Pitchers return at only ~58% (vs ~87% non-pitchers)
- •Tenotomy: Popeye deformity ~23% vs ~7% tenodesis
- •Tenodesis: Equivalent pain/function, less deformity
Normal Variants (Do NOT repair)
- •Sublabral foramen (1-3 o-clock)
- •Buford complex (cord-like MGHL)
- •Meniscoid labrum (loose attachment)
- •Distinguish by stable biceps anchor