Volar Angulated Distal Radius | Flexion Mechanism | Volar Plating Standard
THOMAS CLASSIFICATION (3 TYPES)
Critical Must-Knows
- Volar angulation distinguishes Smith from Colles (dorsal angulation)
- Flexed wrist FOOSH or direct blow to dorsal wrist = typical mechanism
- Volar plate fixation is treatment of choice - provides buttress against volar displacement
- Thomas Type II is essentially a volar Barton fracture - highly unstable, needs surgery
- Flexor tendon irritation is main complication - assess at follow-up
Clinical Pearls
- "Smith = volar angulation, Colles = dorsal angulation (garden spade vs dinner fork)
- "All displaced Smith fractures require surgical fixation - casting fails
- "FCR approach protects median nerve and allows direct fracture visualization
- "Volar plate acts as buttress preventing re-displacement
High-Yield Smith's Fracture Exam Points
Smith vs Colles
CRITICAL DIFFERENTIATION: Smith = volar angulation (apex dorsal), Colles = dorsal angulation (apex volar). Smith is the "reverse Colles." Think: Smith = Sunrise (apex points up/dorsal).
Instability Pattern
Smith fractures are inherently unstable due to volar carpal shift. The strong volar ligaments pull the distal fragment volarly. Casting alone has high failure rate - most require volar plate fixation.
Thomas Classification
Type I: Extra-articular transverse. Type II: Intra-articular (volar Barton variant). Type III: Extra-articular oblique. Type II is most unstable and always requires surgery.
Surgical Approach
FCR approach is standard for volar plating. The plate provides a buttress effect against the volar displacing forces. Distal locking screws capture dorsal cortex for stability.
At a Glance: Smith's Fracture Management
| Fracture Type | Stability | Management | Key Consideration |
|---|---|---|---|
| Type I - Undisplaced | Relatively stable | Consider casting if aligned | Very rare - most are displaced |
| Type I - Displaced | Unstable | Volar plate ORIF | Standard surgical indication |
| Type II (Volar Barton) | Highly unstable | Volar plate ORIF mandatory | Intra-articular requires anatomic reduction |
| Type III - Oblique | Moderately unstable | Volar plate ORIF | Obliquity makes casting unreliable |
| Associated carpal injury | Complex instability | Address both components | Assess scapholunate, DRUJ |
SMITH - KSMITH - Key Features
| S | Sunrise apex Apex dorsal (pointing up like sunrise) |
| M | Mechanism = flexed FOOSH Fall on flexed wrist or direct dorsal blow |
| I | Inherently unstable Volar ligaments pull fragment - needs surgery |
| T | Thomas classification Types I, II, III based on fracture pattern |
| H | Handle with volar plate Volar buttress plating is standard treatment |
| S | Sunrise apex Apex dorsal (pointing up like sunrise) | T | Thomas classification Types I, II, III based on fracture pattern |
| M | Mechanism = flexed FOOSH Fall on flexed wrist or direct dorsal blow | H | Handle with volar plate Volar buttress plating is standard treatment |
| I | Inherently unstable Volar ligaments pull fragment - needs surgery |
Hook:SMITH reminds you of the Sunrise apex and that volar plating is the fix
VOLAR - WVOLAR - Why Volar Plate Works
| V | Volar approach (FCR) Direct access to fracture site |
| O | Opposing force Buttresses against volar displacement |
| L | Locking screws Distal locking screws capture dorsal cortex |
| A | Anatomic reduction Direct visualization of articular surface |
| R | Rigid fixation Allows early mobilization |
| V | Volar approach (FCR) Direct access to fracture site | A | Anatomic reduction Direct visualization of articular surface |
| O | Opposing force Buttresses against volar displacement | R | Rigid fixation Allows early mobilization |
| L | Locking screws Distal locking screws capture dorsal cortex |
Hook:VOLAR plating provides the buttress that neutralizes the volar displacing force
FCR AFCR Approach Steps
| F | Find FCR tendon Palpate at wrist crease |
| C | Cut along radial border Incise sheath radial to FCR |
| R | Retract FCR ulnarly Protects median nerve which is ulnar to FCR |
| F | Find FCR tendon Palpate at wrist crease |
| C | Cut along radial border Incise sheath radial to FCR |
| R | Retract FCR ulnarly Protects median nerve which is ulnar to FCR |
Hook:FCR approach protects median nerve - retract FCR ulnarly to stay safe
I-II-IIIThomas Types I-II-III
| I | I = Transverse extra-articular Simple transverse fracture pattern |
| II | II = Intra-articular (Barton) Volar lip fracture with carpal subluxation |
| III | III = Oblique extra-articular Juxta-articular oblique line |
| I | I = Transverse extra-articular Simple transverse fracture pattern |
| II | II = Intra-articular (Barton) Volar lip fracture with carpal subluxation |
| III | III = Oblique extra-articular Juxta-articular oblique line |
Hook:Type II is the worst - Intra-articular means Inherently unstable
Overview and Epidemiology
Smith's fracture is a distal radius fracture with volar angulation of the distal fragment (apex dorsal). It was first described by Irish surgeon Robert William Smith in 1847, 33 years after Abraham Colles described the dorsally angulated variant.
Terminology:
- Also known as "reverse Colles fracture"
- The eponym specifically refers to the volar angulation pattern
- Distinguished from volar Barton (which is a rim fracture with subluxation)
Epidemiology:
- Accounts for approximately 5% of all distal radius fractures
- Less common than Colles fractures (approximately 1:10 ratio)
- Bimodal distribution: young adults (high-energy trauma) and elderly (low-energy falls)
- Male predominance in younger patients (sports, motorcycle accidents)
- Equal gender distribution in elderly
Mechanism of injury:
- Fall on outstretched hand with wrist flexed (most common)
- Direct blow to dorsum of hand forcing wrist into flexion
- High-energy: motorcycle accidents, sports injuries
- Low-energy: falls in elderly with osteoporotic bone
Historical Context
Robert William Smith was Professor of Surgery at Trinity College Dublin. His 1847 treatise "A Treatise on Fractures in the Vicinity of Joints and on Certain Forms of Accidental and Congenital Dislocations" described this fracture pattern as distinct from the Colles fracture.
Anatomy and Pathophysiology
Distal radius anatomy relevant to Smith fractures:
The distal radius has several key features:
- Volar tilt: Normal volar tilt is 10-15 degrees (palmar inclination)
- Radial inclination: Normal is 22-23 degrees
- Radial height: Normal is 11-12mm
- Ulnar variance: Usually neutral to slightly negative
Ligamentous attachments:
- Volar radiocarpal ligaments (radioscaphocapitate, long radiolunate, short radiolunate) are strong
- These ligaments remain attached to the distal fragment
- They pull the fragment volarly, creating the characteristic deformity
- This explains why Smith fractures are inherently unstable
Pathomechanics of Smith fracture:
Why Smith Fractures Displace Volarly
The strong volar radiocarpal ligaments remain attached to the distal fragment. When the fracture occurs, these ligaments pull the fragment volarly. Unlike Colles fractures where dorsal comminution allows settling, Smith fractures have intact volar cortex that creates a fulcrum for volar angulation.
Force transmission:
- Fall with flexed wrist applies bending moment
- Volar cortex fails in tension (transverse fracture)
- Or direct blow creates shear force (oblique fracture)
- Volar ligaments pull distal fragment volarly
- Pronator quadratus may contribute to deforming force
Watershed line:
- Critical landmark on volar distal radius
- Marks transition from flat metaphyseal surface to curved articular surface
- Volar plate should NOT extend beyond this line (causes flexor tendon irritation)
Classification Systems
Thomas Classification (1957) - Standard for Smith fractures
| Type | Description | Characteristics | Stability |
|---|---|---|---|
| I | Extra-articular transverse | Simple transverse fracture through metaphysis | Moderate |
| II | Intra-articular | Volar lip fracture with carpal subluxation (volar Barton variant) | Highly unstable |
| III | Extra-articular oblique | Oblique fracture line juxta-articular | Unstable |
Type II = Volar Barton
Thomas Type II is essentially a volar Barton fracture - an intra-articular volar lip fracture with volar subluxation of the carpus. This is highly unstable and ALWAYS requires surgical fixation. The intact volar lip fragment acts as a ramp that the carpus slides volarly upon.
Clinical Assessment
History:
- Mechanism (FOOSH with flexed wrist, direct blow, high-energy trauma)
- Hand dominance
- Occupation and functional demands
- Previous wrist injuries
- Medical comorbidities (diabetes, osteoporosis)
Physical examination:
Clinical Examination Findings
| Finding | Significance | Assessment |
|---|---|---|
| Volar wrist swelling | Characteristic of Smith pattern | Compare to contralateral side |
| Volar prominence of distal fragment | Garden spade deformity (opposite of dinner fork) | Assess degree of displacement |
| Wrist held in flexion | Antalgic posture | Patient avoids extension |
| Median nerve symptoms | At risk with volar displacement | Test sensation and motor (APB) |
| Skin integrity | Open fracture assessment | Document any wounds |
| DRUJ tenderness | Associated injury | Assess DRUJ stability after fixation |
Neurovascular assessment:
- Median nerve: Most at risk due to volar displacement
- Sensation in thumb, index, middle finger
- Motor: abductor pollicis brevis (APB)
- Carpal tunnel symptoms may develop acutely
- Radial artery: Palpate at anatomical snuffbox and wrist
- Capillary refill: Assess all digits
Garden Spade vs Dinner Fork
Smith = Garden spade deformity (volar prominence, wrist appears flexed) Colles = Dinner fork deformity (dorsal prominence, wrist appears extended) These eponymous descriptions help distinguish the fractures clinically before imaging.
Associated injuries to assess:
- Scapholunate ligament injury
- TFCC injury
- DRUJ instability
- Carpal fractures (especially scaphoid)
- Ulnar styloid fracture
Differential diagnosis:
The volar-prominence deformity and a distal radius injury on plain films can mimic several patterns. The single most discriminating step is the lateral radiograph (direction of angulation) and whether the fracture is articular.
Differential Diagnosis of the Volarly Deformed / Injured Wrist
| Diagnosis | Distinguishing feature | How to confirm / refute |
|---|---|---|
| Smith fracture (this topic) | Extra-articular distal radius fracture with volar angulation (apex dorsal), garden spade deformity | Lateral radiograph shows volar tilt of distal fragment; no carpal subluxation in Types I/III |
| Volar Barton (Thomas II) | Intra-articular volar rim fracture with volar carpal subluxation | Lateral shows carpus translated volarly with the rim fragment; CT defines articular extent |
| Colles fracture | Dorsal angulation (apex volar), dinner fork deformity | Lateral shows dorsal tilt - the opposite of Smith |
| Dorsal Barton | Intra-articular dorsal rim fracture with dorsal carpal subluxation | Lateral shows dorsal translation of carpus with dorsal rim fragment |
| Chauffeur (radial styloid) fracture | Oblique radial styloid fracture, often from scaphoid impaction | PA view shows styloid fragment; assess scapholunate interval |
| Distal radius epiphyseal / physeal injury (paediatric) | Salter-Harris pattern through the physis, not a true Smith eponym | Age and physeal involvement on radiograph |
| Perilunate / lunate dislocation | Carpal malalignment without a simple metaphyseal radius fracture | Lateral shows lost radius-lunate-capitate collinearity; AP shows crowded carpus |
| Isolated DRUJ injury / Galeazzi | Forearm fracture with DRUJ disruption rather than isolated distal radius bending | Assess full forearm radiograph and DRUJ stability |
Investigations
Radiographic assessment:
Standard views:
- PA view: Assess radial inclination, radial height, ulnar variance
- Lateral view: Critical for diagnosis - shows volar angulation
- Oblique view: Additional assessment of articular involvement
Key measurements on lateral view:
Signs of Smith fracture on X-ray:
- Volar angulation of distal fragment (apex dorsal)
- Volar displacement of carpus
- Loss of normal volar tilt (or reversal)
- Possible intra-articular extension (Type II)
CT imaging:
- Indicated for intra-articular fractures (Type II)
- Defines articular step-off and gap
- Helps surgical planning for fragment-specific fixation
- Not routine for simple Type I fractures
MRI:
- Not routine for acute fractures
- Consider if ligamentous injury suspected (persistent pain)
- Assess TFCC, scapholunate ligament
Lateral View is Key
The lateral radiograph is ESSENTIAL for diagnosing Smith fractures. The PA view may look similar to a Colles fracture - only the lateral view demonstrates the characteristic volar angulation that defines a Smith fracture.
Management Algorithm
Indications for non-operative management:
- Truly non-displaced fractures (rare)
- Acceptable alignment maintained in cast
- Patient factors precluding surgery
Non-operative technique:
- Closed reduction under hematoma block or sedation
- Sugar-tong splint initially (allows swelling)
- Convert to long arm cast at 1 week
- Position: wrist in extension, forearm supinated
- Duration: 6 weeks
High Failure Rate
Non-operative management of displaced Smith fractures has a high failure rate due to the deforming forces of the volar ligaments. Close follow-up with weekly X-rays for first 2-3 weeks is essential. Any loss of reduction is indication for surgery.
Acceptable alignment (non-operative):
- Volar tilt: neutral or positive (not dorsal)
- Radial inclination: within 5 degrees of normal
- Radial height: within 3mm of normal
- Articular step: less than 2mm
Non-operative management is rarely successful for displaced Smith fractures and most surgeons recommend primary surgical fixation.
Surgical Technique
Patient positioning:
- Supine on operating table
- Arm table or hand table
- Tourniquet on upper arm (250-280 mmHg)
- Image intensifier from opposite side
FCR (Flexor Carpi Radialis) Approach:
- Incision: Longitudinal over FCR tendon, 6-8cm from wrist crease proximally
- Identify FCR: Palpate tendon, incise sheath
- Retract FCR ulnarly: This protects the median nerve (ulnar to FCR)
- Incise floor of FCR sheath: Exposes flexor pollicis longus (FPL)
- Retract FPL radially: Exposes pronator quadratus
- Elevate pronator quadratus: L-shaped incision, elevate from radial border
- Expose fracture: Direct visualization of volar radius
Median Nerve Protection
The median nerve lies ULNAR to FCR. By retracting FCR ulnarly, the nerve is protected. This is the key safety principle of the FCR approach. Never dissect ulnar to FCR without identifying the nerve.
The FCR approach provides excellent exposure of the volar distal radius while protecting neurovascular structures.
Complications
Complications of Smith Fractures and Treatment
| Complication | Incidence | Prevention/Management |
|---|---|---|
| Flexor tendon irritation/rupture | 5-10% | Plate position below watershed line, PQ repair |
| Malunion | Varies with treatment | Anatomic reduction, stable fixation |
| Median nerve injury | 5-8% | Protect during approach, avoid excessive retraction |
| Hardware irritation | 10-15% | Proper plate sizing, consider removal at 1 year |
| DRUJ instability | 5-10% | Address ulnar styloid base, repair TFCC |
| Carpal tunnel syndrome | 5% | Release if acute, monitor if subacute |
| Stiffness | 10-20% | Early mobilization, hand therapy |
| Complex regional pain syndrome | 2-5% | Early recognition, multimodal treatment |
Flexor tendon complications:
Flexor Pollicis Longus Rupture
FPL rupture is the most concerning complication of volar plating. Risk factors include: (1) Plate extending beyond watershed line, (2) Prominent screw heads, (3) Failure to repair pronator quadratus. Patients present with loss of IP joint flexion of thumb. Treatment is tendon reconstruction (FDS ring finger transfer).
Malunion:
- Volar malunion is better tolerated than dorsal (Colles pattern)
- Loss of volar tilt affects wrist mechanics
- Symptomatic malunion may require corrective osteotomy
Median nerve injury:
- Can occur from initial injury (volar displacement)
- Or from surgical approach
- Most are neuropraxic and recover
- Acute carpal tunnel may require release
Postoperative Care and Rehabilitation
- Volar splint in neutral position
- Elevation above heart level
- Active finger ROM immediately
- Ice and analgesia
- Wound check at 48-72 hours
- Remove splint, convert to removable wrist brace
- Begin active wrist ROM (flexion/extension, radial/ulnar deviation)
- Suture removal at 10-14 days
- Hand therapy referral
- Continue finger and elbow ROM
- Progress active wrist ROM
- Begin forearm rotation
- Edema control (compression, elevation)
- Scar massage
- Light functional use
- X-ray at 6 weeks to confirm healing
- Discontinue brace
- Progressive strengthening
- Grip strengthening exercises
- Return to light duties
- Full ROM goal by 8-10 weeks
- Return to full activities
- Sports clearance at 3 months if healed
- Consider hardware removal if symptomatic
- Final outcome assessment
Rehabilitation principles:
- Early ROM prevents stiffness
- Volar plate allows early mobilization
- Strengthening delayed until fracture healed (6 weeks)
- Hand therapy optimizes outcomes
- Patient education on activity restrictions
Early Motion
The advantage of volar locked plating is the ability to begin early ROM within the first week. This reduces stiffness and improves outcomes. Traditional casting required 6 weeks of immobilization.
Outcomes and Prognosis
Outcomes with modern treatment:
Volar locked plating of Smith fractures produces excellent results in most patients. Functional outcomes are comparable to or better than historical non-operative management.
Prognostic factors:
- Favorable: Young age, isolated injury, anatomic reduction
- Unfavorable: Intra-articular involvement, associated carpal injury, elderly with osteoporosis
Functional outcomes:
- Most patients achieve functional ROM (60 degrees flexion/extension, 30 degrees radial/ulnar deviation)
- Grip strength typically recovers to 80-90% of contralateral
- Return to work: 4-8 weeks (desk work), 8-12 weeks (manual labor)
- Return to sport: 3-4 months
Long-term considerations:
- Post-traumatic arthritis in intra-articular fractures (Type II)
- Hardware removal if symptomatic (15-20% rate)
- Overall prognosis excellent with modern fixation techniques
Evidence Base
- Landmark series of 29 patients (31 fractures) treated through a single volar approach with a new fixed-angle (locking) plate. Final volar tilt averaged 5 degrees, radial inclination 21 degrees, radial shortening 1mm, articular incongruity 0mm, grip strength 79% of contralateral. All Gartland and Werley scores were excellent or good. Preservation of dorsal soft tissues gave rapid healing with a low incidence of tendon problems.
- RCT of 73 patients: 36 volar locking plate versus 37 closed reduction and cast. Plating gave better early DASH/PRWE and significantly better grip strength at every time point, plus better radiographic restoration (dorsal tilt, radial inclination, radial shortening). However ROM, pain and patient-rated scores were equivalent at 12 months, and complications were higher in the operative group (13 versus 5).
- Two-cohort comparative study (168 plated radii) that defined the Soong grading of plate prominence relative to the volar critical (watershed) line: Grade 0 (proximal/not volar to the line), Grade 1 (volar to line but proximal to rim) and Grade 2 (on or distal to the rim). All flexor tendon ruptures occurred with the more prominent plate design, and Grade 2 prominence was strongly over-represented in the rupture cases.
- Cohort of 594 (later 321) volar-plated distal radius fractures. Plate-attributable complications were relatively uncommon; the commonest late problem was flexor tendon irritation (one frank FPL rupture), with intra-articular screws and tendon rupture as the major complications (about 1.3% early, less than 1% late). Higher-energy injury and ipsilateral elbow injury predicted early complications; plate design and surgeon familiarity influenced later ones.
- Distal radius fractures are among the commonest fractures worldwide, with a bimodal age distribution: a peak in children/young adults from higher-energy trauma and a larger peak in older (predominantly female, osteoporotic) patients from low-energy falls. Prevalence has trended upward over four decades in both the paediatric and elderly populations.
- Cochrane review of 26 RCTs (1269 patients). Evidence for any specific rehabilitation regimen was low or very low quality; after volar plate fixation, a structured home exercise programme preceded by therapist instruction performed at least as well as routine supervised physiotherapy, and accelerated rehabilitation gave only a short-term benefit.
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Classic Smith Fracture Presentation
"A 32-year-old motorcyclist presents after low-speed fall onto his flexed left wrist. X-rays show a distal radius fracture with volar angulation. The fracture is extra-articular. How would you manage this patient?"
Scenario 2: Thomas Type II - Volar Barton Variant
"A 45-year-old woman presents after a fall with a distal radius fracture. The lateral X-ray shows volar angulation with the carpus subluxated volarly. The fracture involves only the volar rim of the distal radius. What is your diagnosis and management?"
Scenario 3: Smith Fracture with Flexor Tendon Complication
"You see a 55-year-old patient 8 months after volar plating of a Smith fracture. She reports sudden loss of ability to bend her thumb at the IP joint. Examination confirms no active FPL function. What is your diagnosis and management?"
MCQ Practice Points
Definition Question
Q: What distinguishes a Smith fracture from a Colles fracture? A: Smith fracture has volar angulation (apex dorsal), Colles has dorsal angulation (apex volar). Smith = reverse Colles.
Classification Question
Q: A distal radius fracture with volar subluxation of the carpus and fracture of the volar rim is classified as: A: Thomas Type II Smith fracture (also known as volar Barton fracture). This is the most unstable Smith fracture pattern.
Mechanism Question
Q: What is the typical mechanism for a Smith fracture? A: Fall on outstretched hand with wrist in flexion, or direct blow to the dorsum of the hand. This contrasts with Colles which occurs with wrist in extension.
Surgical Approach Question
Q: In the FCR approach for volar plating, which structure is retracted ulnarly? A: The FCR tendon is retracted ulnarly. This protects the median nerve which lies ulnar to FCR.
Complication Question
Q: What is the most significant complication of volar plating related to plate position? A: Flexor pollicis longus rupture due to plate extending beyond the watershed line. Presents with loss of thumb IP flexion.
Guidelines, Registries & Global Practice
Global epidemiology:
Distal radius fractures are among the commonest fractures worldwide, with a bimodal age distribution - a peak in children and young adults from higher-energy mechanisms and a larger peak in older (predominantly female, osteoporotic) patients from low-energy falls. Prevalence has risen over four decades in both groups. Smith (volar-displacing) fractures are far less common than the dorsally displacing Colles pattern, but the volar pattern is over-represented among younger, higher-energy injuries (sport, motorcycle, direct dorsal blow), which is why mechanism shapes the demographic. The figures below are PubMed-verifiable population data, not country-specific framing.
Epidemiology and Demographics (evidence-based)
| Feature | Pattern | Source / Note |
|---|---|---|
| Overall distal radius burden | Among the commonest fractures globally; rising prevalence over 40 years | Nellans 2012 epidemiology review |
| Age distribution | Bimodal: young high-energy peak and larger elderly fragility peak | Nellans 2012 |
| Smith vs Colles | Smith is the minority volar-displacing pattern; Colles dominates overall | Volar pattern skews to younger, higher-energy injury |
| Sport-related distal radius | Wrist/hand fractures are the commonest sport fractures; male predominance in young adults | Court-Brown 2008 sports-fracture epidemiology |
Major guidelines, side by side:
There is no Smith-specific international guideline; recommendations come from the broader distal radius literature and society guidance. The unifying message across bodies is that an unstable, displaced, volarly translating distal radius fracture is poorly controlled by cast alone and is a strong indication for fixation, while low-demand elderly extra-articular fractures may be managed conservatively.
Guideline and Consensus Positions on Distal Radius Fixation
| Body | Position relevant to Smith / volar shear | Evidence basis |
|---|---|---|
| AAOS (USA) CPG | Surgery favoured for fractures with post-reduction radial shortening, dorsal/volar tilt or articular step beyond accepted thresholds; in over-55s evidence does not strongly favour one fixation method | Guideline synthesis, mostly moderate/limited strength |
| NICE / BOA-BOAST (UK) | Definitive fixation within accepted time windows; surgery for unstable or irreducible patterns; shared decision-making, especially in older adults | Consensus + RCT evidence |
| AO Foundation | Volar shear (reverse Barton / Thomas II) is intrinsically unstable and is a surgical lesion; buttress/locked volar plate is the standard construct | Mechanistic + outcome evidence |
| EFORT / European consensus | Anatomic reduction and stable fixation for displaced unstable patterns; early mobilisation after rigid fixation | Consensus + RCT/meta-analysis |
Registry and trial evidence:
National joint registries (NJR, AJRR, AOANJRR, SHAR and others) primarily capture arthroplasty rather than fracture fixation, so distal radius implant-survival data come chiefly from trials and large cohorts rather than registries. The key high-level evidence is therefore:
- Arora 2011 RCT - volar plating gives better early function, grip strength and radiographic restoration than casting in patients 65 and older, but equivalent patient-rated outcomes at 12 months with more complications; this is the central plate-versus-cast trial.
- Soong 2011 - defined the watershed-line plate-prominence grading that governs flexor tendon rupture risk and is now a global benchmark for plate position.
- Handoll & Elliott 2015 Cochrane - no rehabilitation regimen is clearly superior; coached home exercise after stable plating performs at least as well as routine supervised physiotherapy.
Global practice variation:
- High-resource settings: volar locking plate fixation is the default for displaced/unstable Smith and volar-shear (Thomas II) fractures, enabling early motion.
- Limited-resource settings: closed reduction with sugar-tong/cast or K-wire fixation remains common where locking plates or image intensifiers are scarce; for a truly unstable volar-shear pattern this carries a higher redisplacement risk, so buttress fixation is prioritised when available.
- Older, low-demand patients: more variation - acceptance of a degree of malunion in exchange for avoiding surgery is reasonable for extra-articular patterns, but volar-shear instability with carpal translation still favours fixation in any setting.
Implant note (vendor-neutral):
Multiple anatomically pre-contoured volar locking plate systems are available worldwide, with fragment-specific options for complex articular patterns. The principle (a fixed-angle buttress proximal to the watershed line) matters far more than the manufacturer.
How Examiners Probe This Topic
Smith fractures are a favoured topic across boards (FRACS, FRCS Tr & Orth, EBOT, ABOS, DNB) because they test: (1) distinguishing Smith from Colles on the lateral radiograph, (2) the Thomas classification and why Type II (volar Barton) is a surgical lesion, (3) the FCR approach and median-nerve safety, and (4) plate-position complications via the Soong grading. Expect a probe on plate-versus-cast evidence in the elderly (Arora) and on flexor tendon rupture mechanism (watershed line).
SMITH'S FRACTURES
Clinical summary
DEFINING FEATURE
- •Distal radius fracture with VOLAR angulation (apex dorsal)
- •Reverse Colles - Smith = Sunrise (apex up)
- •Less common than Colles (approximately 5% of distal radius fractures)
- •Mechanism: FOOSH with flexed wrist or direct dorsal blow
THOMAS CLASSIFICATION
- •Type I: Extra-articular transverse
- •Type II: Intra-articular volar Barton (most unstable)
- •Type III: Extra-articular oblique
- •Type II ALWAYS needs surgery
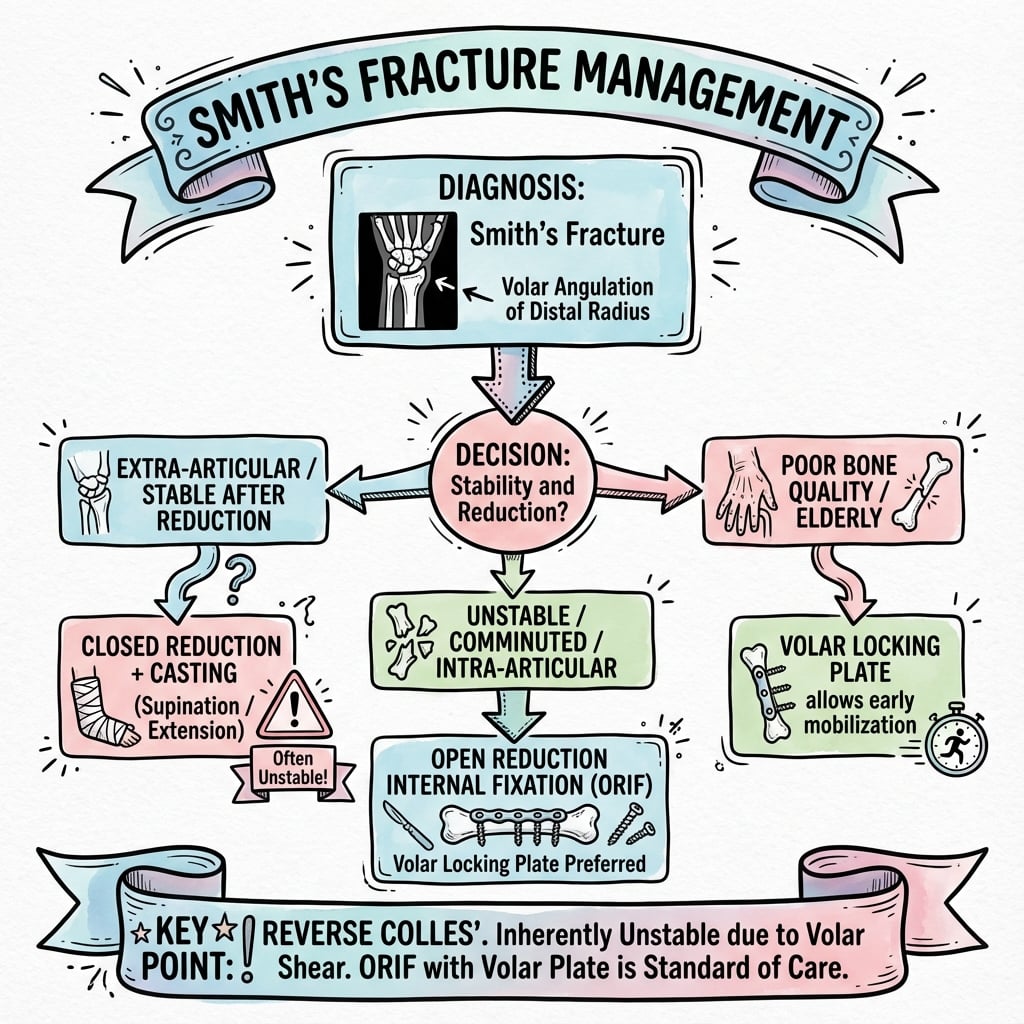
MANAGEMENT
- •Most displaced Smith fractures require surgical fixation
- •Volar locking plate is standard treatment
- •FCR approach: retract FCR ulnarly (protects median nerve)
- •Plate provides BUTTRESS against volar displacement
KEY TECHNICAL POINTS
- •Plate MUST be below watershed line
- •Distal locking screws capture dorsal cortex
- •Confirm with lateral fluoroscopy
- •Repair pronator quadratus over plate
COMPLICATIONS
- •FPL rupture (plate beyond watershed line)
- •Median nerve injury (protect during approach)
- •Malunion (ensure anatomic reduction)
- •Hardware irritation (consider removal if symptomatic)
EXAM TRAPS
- •Confusing Smith with Colles - CHECK LATERAL X-RAY
- •Recommending casting for displaced Smith - high failure rate
- •Missing Type II (volar Barton) pattern
- •Plate placed too distal causing tendon problems