Perioperative Optimization | Pharmacotherapy | Timing Strategies
PHARMACOTHERAPY OPTIONS
Critical Must-Knows
- 4-8 weeks preoperative cessation reduces complications by 50-60%
- Nonunion risk 4-8x higher in smokers undergoing fusion/fracture fixation
- Surgical site infection 3-6x higher in smokers
- Varenicline most effective - triples quit rates compared to placebo
- Continue cessation postoperatively - 12+ weeks for bone healing
Clinical Pearls
- "Even brief cessation (3-4 weeks) improves wound healing
- "Nicotine replacement does NOT increase complications
- "Document smoking status and counseling in notes
- "Australian PBS subsidizes varenicline, NRT, bupropion
Critical Smoking Cessation Points
Fracture Healing
Nicotine reduces osteoblast function and impairs vascular supply. Nonunion rates 4-8 times higher in smokers. Particularly critical in tibial fractures, femoral neck, scaphoid.
Spinal Fusion
Pseudarthrosis rates 2-4x higher in smokers. Essential to achieve 4-8 weeks preoperative and 12+ weeks postoperative cessation for solid fusion.
Wound Complications
SSI risk 3-6x higher in smokers. Impaired tissue oxygenation, immune dysfunction. Particularly high-risk in total joint arthroplasty, open fractures.
Timing Strategy
Minimum 4 weeks preoperative cessation reduces complications. Optimal 8+ weeks. Continue 12+ weeks postoperatively for bone healing procedures.
At a Glance: Cessation Strategy by Procedure
| Procedure Type | Preoperative Cessation | Postoperative Duration | Priority |
|---|---|---|---|
| Spinal fusion | 8+ weeks ideal | 12+ weeks (fusion consolidation) | Critical - highest pseudarthrosis risk |
| Fracture fixation | 4-8 weeks | 12+ weeks (bone healing) | Critical - nonunion risk 4-8x |
| Total joint arthroplasty | 4-8 weeks | 6-12 weeks (wound healing) | High - infection risk 3-6x |
| Arthroscopy | 4 weeks | 2-4 weeks (tissue healing) | Moderate - lower but measurable risk |
| Elective soft tissue | 4 weeks | 4-6 weeks (wound healing) | Moderate - wound complications |
BONES FAILEffects of Smoking on Orthopaedic Healing
| B | Bone formation reduced Osteoblast dysfunction, decreased alkaline phosphatase |
| O | Oxygen delivery impaired Vasoconstriction, reduced tissue PO2 |
| N | Nonunion rates quadrupled 4-8x increased risk in fractures and fusions |
| E | Endothelial dysfunction Microvascular damage, impaired angiogenesis |
| S | Surgical site infections 3-6x increased SSI risk |
| F | Fibroblast function reduced Impaired collagen synthesis |
| A | Angiogenesis impaired Reduced VEGF expression |
| I | Immune dysfunction Reduced neutrophil function, complement |
| L | Longer hospital stay Increased complications, delayed mobilization |
| B | Bone formation reduced Osteoblast dysfunction, decreased alkaline phosphatase | E | Endothelial dysfunction Microvascular damage, impaired angiogenesis | A | Angiogenesis impaired Reduced VEGF expression |
| O | Oxygen delivery impaired Vasoconstriction, reduced tissue PO2 | S | Surgical site infections 3-6x increased SSI risk | I | Immune dysfunction Reduced neutrophil function, complement |
| N | Nonunion rates quadrupled 4-8x increased risk in fractures and fusions | F | Fibroblast function reduced Impaired collagen synthesis | L | Longer hospital stay Increased complications, delayed mobilization |
Hook:BONES FAIL - remember the catastrophic effects of smoking on healing!
VANPharmacotherapy Options
| V | Varenicline Most effective - partial nicotine agonist, 3x quit rate |
| A | Antidepressant (Bupropion) Alternative - doubles quit rate, avoid if seizure risk |
| N | Nicotine replacement therapy Patch/gum/lozenge - doubles quit rate, safe perioperatively |
| V | Varenicline Most effective - partial nicotine agonist, 3x quit rate |
| A | Antidepressant (Bupropion) Alternative - doubles quit rate, avoid if seizure risk |
| N | Nicotine replacement therapy Patch/gum/lozenge - doubles quit rate, safe perioperatively |
Hook:Get in the VAN to quit - Varenicline, Antidepressant, Nicotine replacement!
5 A'sCessation Counseling Framework
| A | Ask Screen all patients for tobacco use at every visit |
| A | Advise Strongly urge all smokers to quit with personalized message |
| A | Assess Determine willingness to make a quit attempt |
| A | Assist Help develop quit plan, provide pharmacotherapy, counseling |
| A | Arrange Schedule follow-up contact to support cessation |
| A | Ask Screen all patients for tobacco use at every visit | A | Assist Help develop quit plan, provide pharmacotherapy, counseling |
| A | Advise Strongly urge all smokers to quit with personalized message | A | Arrange Schedule follow-up contact to support cessation |
| A | Assess Determine willingness to make a quit attempt |
Hook:The 5 A's - standard framework endorsed by all major medical organizations!
WEEKSTiming of Cessation Benefits
| W | Wound healing starts 2-3 weeks - improved tissue oxygenation |
| E | Early benefits 4 weeks - reduced pulmonary complications by 50% |
| E | Extended benefit 8 weeks - optimal reduction in all complications |
| K | Keep going postop 12+ weeks for bone healing procedures |
| S | Sustained cessation best Permanent cessation eliminates long-term risks |
| W | Wound healing starts 2-3 weeks - improved tissue oxygenation | K | Keep going postop 12+ weeks for bone healing procedures |
| E | Early benefits 4 weeks - reduced pulmonary complications by 50% | S | Sustained cessation best Permanent cessation eliminates long-term risks |
| E | Extended benefit 8 weeks - optimal reduction in all complications |
Hook:Count the WEEKS - timing is everything for cessation benefits!
Overview and Epidemiology
Why This Topic Matters
Smoking is the single most modifiable risk factor for orthopaedic complications. Surgeons have a duty to counsel all patients and document smoking status. Effective cessation strategies can dramatically improve outcomes in fracture healing, spinal fusion, and arthroplasty.
Global Practice
- 16.5% of adults smoke (AIHW 2022)
- Higher rates in orthopaedic trauma patients (20-30%)
- PBS subsidies available for varenicline, NRT, bupropion
- Quitline 13 7848 - free telephone counseling service
Economic Impact
- AU$136.9 billion annual cost of smoking to Australian society
- Increased healthcare costs from orthopaedic complications
- Longer hospital stays with smoking-related complications
- Return to work delayed by healing complications
Smoking Prevalence in Orthopaedic Surgery
Smoking rates among orthopaedic patients are typically higher than the general population, particularly in trauma cohorts. Studies report smoking prevalence of 20-40% among patients presenting for fracture care or elective procedures. [1]
Documentation Requirements
Legal and professional responsibility to document:
- Current smoking status (pack-years)
- Cessation counseling provided
- Pharmacotherapy offered
- Patient response and quit plan
- Follow-up arranged
Failure to document may constitute substandard care.
Pathophysiology of Smoking on Orthopaedic Healing
Cellular and Molecular Mechanisms
Effects on Fracture and Fusion Healing
Osteoblast Dysfunction:
- Reduced proliferation and differentiation
- Decreased alkaline phosphatase activity
- Impaired bone matrix production
- Reduced response to BMP-2 and growth factors [2,3]
Angiogenesis Impairment:
- Decreased VEGF (vascular endothelial growth factor) expression
- Reduced capillary formation in fracture callus
- Impaired hematoma organization
- Delayed revascularization [4]
Mechanical Consequences:
- Reduced callus strength and stiffness
- Delayed mineralization
- Increased time to radiographic union
- Higher rates of delayed union and nonunion [5]
This section covers the bone healing impairment caused by smoking.
Dose-Response Relationship
Smoking Intensity and Complication Risk
| Pack-Years | Nonunion Risk | Infection Risk | Cessation Urgency |
|---|---|---|---|
| Under 10 pack-years | 2-3x increased | 2x increased | Moderate priority |
| 10-20 pack-years | 4-5x increased | 3-4x increased | High priority |
| Over 20 pack-years | 6-8x increased | 5-6x increased | Critical priority |
| Current heavy smoker | Up to 8x increased | Up to 6x increased | Immediate intervention |
Classification
Smoking Status Classification
Smoking Status Categories
| Category | Definition | Risk Level | Intervention |
|---|---|---|---|
| Current Smoker | Smoked in past 30 days | Highest risk | Intensive cessation intervention |
| Recent Quitter (less than 1 year) | Quit within past 12 months | Elevated risk, high relapse | Relapse prevention, continued support |
| Former Smoker (greater than 1 year) | Quit greater than 12 months ago | Moderately elevated | Positive reinforcement, monitor |
| Never Smoker | Less than 100 cigarettes lifetime | Baseline risk | No intervention needed |
Quantifying Smoking Exposure
Pack-Years Calculation:
- Pack-years = (Cigarettes per day ÷ 20) × Years smoked
- Example: 20 cigarettes/day for 25 years = 25 pack-years
| Pack-Years | Risk Category | Surgical Implication |
|---|---|---|
| Less than 10 | Low exposure | Moderate complication risk |
| 10-20 | Moderate exposure | Significant complication risk |
| Greater than 20 | High exposure | Major complication risk, consider delay |
Clinical Assessment
Preoperative Smoking Assessment
Essential History:
- Current smoking status (current, former, never)
- Cigarettes per day and pack-years
- Previous quit attempts and methods used
- Reasons for relapse if applicable
- Readiness to quit (stages of change)
- Household/social smoking exposure
Physical Examination Findings:
- Tobacco staining of fingers/teeth
- Chronic cough or sputum production
- Signs of COPD (barrel chest, prolonged expiration)
- Peripheral vascular disease signs
- Wound healing quality from previous surgeries
Stages of Change Assessment
| Stage | Description | Intervention |
|---|---|---|
| Precontemplation | Not considering quitting | Motivational interviewing, 5 R's |
| Contemplation | Thinking about quitting | Explore ambivalence, discuss benefits |
| Preparation | Planning to quit soon | Set quit date, prescribe pharmacotherapy |
| Action | Actively quitting | Support, manage withdrawal |
| Maintenance | Sustained abstinence | Relapse prevention strategies |
Differential Diagnosis of Impaired Bone/Wound Healing
When healing fails in a smoker, smoking is rarely the only contributor. The examiner expects a structured differential so that smoking is not used as a lazy catch-all and reversible co-factors are not missed.
Differential Diagnosis: Causes of Nonunion / Impaired Healing
| Category | Key Examples | Distinguishing Features | How It Changes Management |
|---|---|---|---|
| Patient/biological | Smoking, diabetes, malnutrition, vitamin D deficiency, NSAIDs, steroids | Multiple modifiable factors; smoking confirmed by history/cotinine | Optimise all factors, not smoking alone; glycaemic and nutritional correction |
| Mechanical/technical | Inadequate fixation, excessive fracture gap, instability, malreduction | Hardware loosening or motion on imaging; gap visible on radiographs | Revision fixation or grafting - not solved by cessation alone |
| Biological/vascular | Open/high-energy injury, soft-tissue stripping, atrophic nonunion, AVN | Avascular bone ends, atrophic callus on imaging | Biological augmentation (graft, BMP), vascularised options |
| Infection | Septic (infected) nonunion, low-grade biofilm infection | Pain, raised inflammatory markers, sinus, positive cultures | Debridement, targeted antibiotics, staged reconstruction |
| Endocrine/metabolic | Hypothyroidism, hyperparathyroidism, hypogonadism | Abnormal metabolic bone screen | Treat underlying endocrinopathy before revision |
Investigations
Smoking Status Verification
Self-Report:
- Standard in clinical practice
- Generally accurate when patient trusts provider
- May underreport in settings where consequences exist
Biochemical Markers:
| Test | Sample | Detection Window | Sensitivity | Use |
|---|---|---|---|---|
| Exhaled CO | Breath | 4-6 hours | High for recent use | Point-of-care |
| Cotinine | Blood/urine/saliva | 3-4 days | Very high | Gold standard |
| Thiocyanate | Blood | 1-2 weeks | Moderate | Research only |
Preoperative Workup in Smokers
Consider Based on Smoking History:
- Chest X-ray (if greater than 20 pack-years or symptoms)
- Spirometry (if COPD suspected)
- ECG (if cardiac risk factors)
- Blood gas or SpO2 at rest (if respiratory symptoms)
Management
Cessation Management Algorithm
Cessation Approach by Clinical Scenario
| Scenario | Time to Surgery | Pharmacotherapy | Behavioral Support |
|---|---|---|---|
| Elective surgery - motivated | 8+ weeks | Varenicline (first-line) | Quitline + regular follow-up |
| Elective surgery - limited time | 4-8 weeks | NRT (immediate start) | Brief intervention + Quitline |
| Semi-urgent surgery | 1-4 weeks | NRT (patch + short-acting) | Brief intervention, postop focus |
| Emergency surgery | Less than 24 hours | NRT postoperatively | Counseling when stable, 12-week postop focus |
First-Line Approach
- Brief counseling (5 A's framework)
- Pharmacotherapy - offer to ALL motivated smokers
- Quitline referral (13 7848)
- Set quit date - ideally 8+ weeks before surgery
- Follow-up - within 1 week of quit date
Intraoperative Considerations
Intraoperative Management of Smokers
Anesthetic Considerations:
- Increased airway reactivity - higher risk of bronchospasm
- May need higher oxygen concentrations
- Impaired mucociliary clearance - secretion management
- Carbon monoxide displaces O2 - optimize oxygenation
Surgical Technique Modifications:
- Meticulous hemostasis (impaired wound healing)
- Consider tissue-sparing approaches when possible
- Avoid excessive tension on wound closure
- Thoughtful incision placement away from pressure points
Nicotine Replacement Perioperatively
| Timing | Recommendation |
|---|---|
| Night before surgery | Apply nicotine patch as usual |
| Morning of surgery | Continue patch (or apply new one) |
| Intraoperatively | Leave patch in place |
| PACU | Monitor, continue NRT |
| Postoperatively | Resume/continue all NRT forms as tolerated |
Complications
Smoking-Related Surgical Complications
Complication Rates: Smokers vs Non-Smokers
| Complication | Non-Smoker Rate | Smoker Rate | Relative Risk |
|---|---|---|---|
| Nonunion (fracture/fusion) | 5-10% | 20-40% | 4-8x |
| Surgical site infection | 1-3% | 5-15% | 3-6x |
| Wound dehiscence | 1-2% | 5-10% | 3-5x |
| Pulmonary complications | 3-5% | 10-20% | 2-4x |
| DVT/PE | 1-2% | 3-6% | 2-3x |
Management of Complications in Smokers
Nonunion:
- Address smoking BEFORE revision surgery
- Bone stimulation may help (limited evidence)
- Consider biologics (BMP, bone graft)
- Higher index of suspicion at follow-up
Wound Infection:
- Lower threshold for deep samples
- May need longer antibiotic courses
- Wound healing support measures
Postoperative Care
Postoperative Cessation Support
Immediate Postoperative (Day 0-3):
- Continue or resume NRT as soon as tolerated
- If patch removed for surgery, reapply in PACU
- Acknowledge difficulty of quitting during recovery
- Provide short-acting NRT for breakthrough cravings
Hospital Stay:
- Smoke-free environment supports abstinence
- Address pain adequately (pain increases relapse risk)
- Offer ongoing behavioral support
- Consider inpatient smoking cessation consultation
Duration of Postoperative Cessation
| Procedure Type | Minimum Duration | Rationale |
|---|---|---|
| Fracture fixation | 12+ weeks | Complete bone healing |
| Spinal fusion | 12+ weeks | Fusion consolidation |
| Total joint arthroplasty | 6-12 weeks | Wound and osseointegration |
| Soft tissue procedures | 4-6 weeks | Wound healing completion |
Outcomes
Outcomes with Smoking Cessation
Complication Reduction:
- 50-60% reduction in overall surgical complications with 6-8 week preoperative cessation
- Wound complications reduced from 31% to 5% (Møller RCT)
- Lumbar fusion nonunion reduced from 26.5% (continued smokers) to 17.1% with postoperative cessation, approaching the 14.2% nonsmoker rate (Glassman)
Quit Rates with Intervention:
- Brief advice alone: 3-5% at 1 year
- Varenicline: 25-30% at 1 year
- NRT: 15-20% at 1 year
- Combination (behavioral + pharmacotherapy): 30-40% at 1 year
Benefits of Cessation by Duration
| Cessation Duration | Physiological Benefits |
|---|---|
| 24-48 hours | CO levels normalize, O2 delivery improves |
| 2-4 weeks | Circulation improves, nicotine eliminated |
| 4-8 weeks | Wound healing approaches non-smoker |
| 12+ weeks | Bone healing capacity improved |
| 1 year+ | Risk approximates non-smoker for many outcomes |
Evidence Base for Cessation
Evidence by Procedure Type
Spinal Fusion Outcomes
Landmark Studies:
- Glassman et al. (2000): instrumented lumbar fusion nonunion 26.5% in persistent smokers vs 14.2% in nonsmokers, falling to 17.1% in those who quit greater than 6 months postoperatively [12]
- Andersen et al. (2001): smoking an independent predictor of negative outcome (impaired fusion) in lumbar spinal fusion [13]
- Møller et al. (2002): Intensive smoking cessation intervention reduced overall complications from 52% to 18% (RCT in hip/knee arthroplasty) [14]
Key Findings:
- Pseudarthrosis rates 2-4x higher in smokers
- Effect most pronounced in posterolateral fusion (uninstrumented)
- Interbody fusion somewhat more resistant but still affected
- Dose-dependent effect - heavier smokers worse outcomes
Cessation Benefits:
- 4-8 weeks preoperative cessation reduces pseudarthrosis risk
- 12+ weeks postoperative continuation essential for fusion consolidation
- Even brief cessation provides measurable benefit
This completes the spinal fusion evidence.
Timing of Cessation: Critical Evidence
Some benefit but suboptimal. Still strongly recommend - better than continued smoking.
Improved tissue oxygenation beginning. Insufficient for maximal complication reduction.
50% reduction in pulmonary complications. Measurable improvement in wound healing. Minimum acceptable for elective procedures. [21]
60% reduction in all complications. Approaching non-smoker baseline for some outcomes. Target for elective surgery. [14]
Essential for fracture union and spinal fusion. Continue cessation through healing period.
The 4-8 Week Window
Minimum 4 weeks, optimal 8 weeks preoperative cessation is the evidence-based standard. Shorter durations provide some benefit but do not maximize complication reduction. For elective procedures, consider delaying surgery to achieve 8-week cessation if patient is motivated.
Pharmacotherapy for Smoking Cessation
First-Line Pharmacological Options
Pharmacotherapy Options Comparison
| Agent | Mechanism | Efficacy (vs Placebo) | Adverse Effects | PBS Coverage |
|---|---|---|---|---|
| Varenicline | Partial nicotinic agonist | 3x quit rate (NNT=10) | Nausea, vivid dreams, rare mood changes | Yes - restricted benefit |
| NRT (patch/gum/lozenge) | Nicotine replacement | 2x quit rate (NNT=20) | Local irritation, insomnia | Yes - general benefit |
| Bupropion | Antidepressant, dopamine/NE reuptake inhibitor | 2x quit rate (NNT=20) | Insomnia, dry mouth, seizure risk | Yes - restricted benefit |
| Combination NRT | Patch + short-acting NRT | Higher than single NRT | Similar to single NRT | Yes |
Varenicline (Champix)
Mechanism:
- Partial agonist at alpha-4 beta-2 nicotinic acetylcholine receptors
- Reduces craving and withdrawal (partial agonist effect)
- Blocks rewarding effects of nicotine (competitive antagonism)
Efficacy:
- Most effective pharmacotherapy available
- Triples quit rates compared to placebo (30% vs 10% at 1 year) [22]
- Superior to bupropion and single-agent NRT [23]
- NNT = 10 (number needed to treat to achieve one additional quitter)
Dosing:
- Standard course: 12 weeks
- Start 1 week before quit date
- Days 1-3: 0.5mg once daily
- Days 4-7: 0.5mg twice daily
- Day 8 onwards: 1mg twice daily
- Can extend to 24 weeks for relapse prevention
Adverse Effects:
- Nausea (30% - usually transient, dose with food)
- Vivid dreams or insomnia (20%)
- Headache (15%)
- Neuropsychiatric concerns: Rare mood changes, depression (FDA black box warning removed 2016 after safety review)
Contraindications:
- Severe renal impairment (dose reduction required)
- Pregnancy (insufficient data - use only if benefit outweighs risk)
- History of serious psychiatric illness (use with caution, monitor closely)
Australian Context:
- PBS listed - restricted benefit (requires certain criteria)
- Typically AU$42.50 per script (general patient)
- Cost-effective given efficacy
This completes the varenicline section.
PBS Prescribing in Australia
PBS subsidies available for smoking cessation medications:
- Varenicline: Restricted benefit - maximum 2 courses per year
- Bupropion: Restricted benefit - maximum 2 courses per year
- NRT: General benefit - patches, gum, lozenges
Authority approval may be required. Check PBS website for current requirements.
Behavioral Counseling and Support
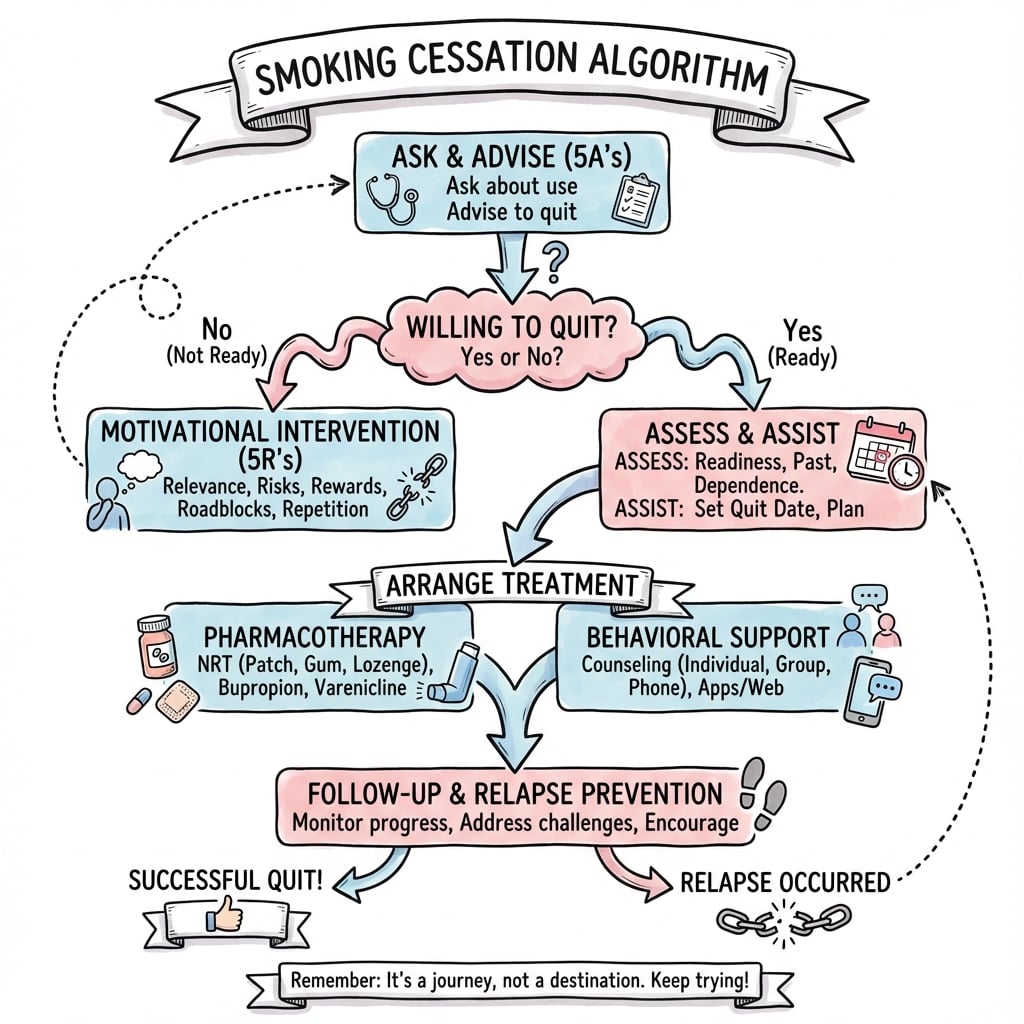
The 5 A's Framework
1. ASK
Screen all patients for tobacco use at every clinical encounter.
- "Do you currently smoke or use tobacco?"
- "How many cigarettes per day? For how many years?"
- Calculate pack-years (packs per day multiplied by years)
- Document in medical record
2. ADVISE
Strongly urge all smokers to quit with clear, personalized message.
- "Quitting smoking is the single most important thing you can do to improve your surgical outcome."
- Relate to specific orthopaedic risks: "Smoking increases your risk of nonunion/infection by 4-6 times."
- Be direct but empathetic
3. ASSESS
Determine willingness to make a quit attempt.
- "Are you willing to quit smoking before your surgery?"
- Assess readiness to change (precontemplation, contemplation, preparation, action)
- If not ready: use motivational interviewing techniques
- If ready: proceed to assist
4. ASSIST
Help develop quit plan and provide resources.
- Set quit date (ideally 8+ weeks before surgery)
- Recommend pharmacotherapy (varenicline, NRT, bupropion)
- Provide behavioral support (Quitline referral)
- Address triggers and develop coping strategies
- Enlist social support (family, friends)
5. ARRANGE
Schedule follow-up to support cessation effort.
- First follow-up within 1 week of quit date
- Regular contact during first month (highest relapse risk)
- Monitor at preoperative visits
- Continue support postoperatively through healing period
- Celebrate successes, troubleshoot challenges
Brief Intervention (Under 5 minutes)
For time-limited clinical encounters, use Ask-Advise-Refer model:
- Ask: Screen for smoking status
- Advise: Clear personalized message to quit
- Refer: Give Quitline number (13 7848) and/or prescribe pharmacotherapy
Effectiveness: Even brief interventions (under 3 min) increase quit rates by 30-40% when combined with pharmacotherapy. [25]
Motivational Interviewing Techniques
For patients not ready to quit:
Explore ambivalence:
- "What do you like about smoking?"
- "What concerns do you have about smoking?"
- Elicit change talk - patient's own reasons to quit
Address the 5 R's:
- Relevance: Personalize risks to patient's situation
- Risks: Short-term (surgical) and long-term (cancer, COPD, CVD)
- Rewards: Benefits of quitting (better healing, save money, health)
- Roadblocks: Identify barriers (withdrawal, weight gain, stress)
- Repetition: Repeat intervention at each visit (don't give up!)
Quitline Referral
Quitline (13 7848) - Free national telephone counseling service:
- Evidence-based behavioral support
- Trained counselors
- Multiple callback sessions
- Free NRT in some jurisdictions
- Effective: Increases quit rates by 50-100% [26]
Referral process:
- Give patient the number: 13 7848
- Encourage active call
- Consider fax referral (patient consent) - Quitline calls patient
Perioperative Smoking Cessation Protocol
Preoperative Optimization Protocol
- Screen all patients for smoking status
- Document pack-years in medical record
- Provide 5 A's counseling (Ask, Advise, Assess, Assist, Arrange)
- Explain orthopaedic-specific risks (nonunion, infection)
- Set quit date (target 8+ weeks before surgery)
- Prescribe pharmacotherapy (varenicline first-line)
- Refer to Quitline (13 7848)
- Provide written information
- Start varenicline 1 week before quit date (or NRT/bupropion on quit date)
- Patient quits smoking
- First follow-up within 1 week (phone or in-person)
- Address withdrawal symptoms
- Reinforce behavioral strategies
- Monitor pharmacotherapy adherence and side effects
- Highest relapse risk period - frequent contact essential
- Troubleshoot challenges (cravings, withdrawal, side effects)
- Adjust pharmacotherapy if needed (dose, combination therapy)
- Reinforce benefits already achieved
- Continue behavioral support
- Minimum 4 weeks, optimal 8 weeks achieved
- Patient physiologically optimized for surgery
- Complications reduced by 50-60%
- Continue pharmacotherapy through surgery
- DO NOT stop NRT perioperatively - safe and reduces relapse risk
- Verify abstinence (patient report, consider cotinine testing if high-stakes)
- Document cessation duration in preoperative note
- Confirm plan for postoperative continuation
- Consider incentive spirometry teaching (reduce pulmonary complications)
Intraoperative and Postoperative Management
Perioperative Nicotine Replacement:
- Continue NRT through surgery - apply patch morning of surgery
- Safe for wound healing (no combustion products)
- Reduces postoperative relapse risk
- For non-patch users: restart short-acting NRT as soon as tolerated postop
Postoperative Continuation:
- Critical period: Bone healing takes 12+ weeks for fractures/fusions
- Continue pharmacotherapy for minimum 12 weeks (standard), longer for bone healing procedures
- Regular follow-up at postoperative visits
- Monitor for relapse (pain, stress, boredom in hospital)
- Address pain adequately (inadequate pain control increases relapse risk)
Relapse Prevention:
- Identify high-risk situations (alcohol, social settings, stress)
- Develop coping strategies for cravings
- Enlist social support
- Consider extended pharmacotherapy (24 weeks vs 12 weeks) for relapse prevention
- Long-term cessation reduces lifetime orthopaedic complication risk
Special Clinical Scenarios
Acute Trauma and Urgent Surgery
Challenge: Limited time for preoperative cessation in acute fractures or urgent procedures.
Approach:
- Still counsel to quit even if surgery imminent
- Emphasize postoperative cessation for bone healing (12+ weeks)
- Initiate pharmacotherapy immediately (NRT can start same day)
- Even brief cessation provides benefit - every day counts
- For urgent surgery (within 24-48 hours): focus on postoperative plan
Evidence:
- Quitting at time of injury still reduces complications vs continued smoking
- 12-week postoperative cessation critical for fracture union
- Provide intensive support during hospitalization (captive audience)
Specific Recommendations:
- Open fractures: Infection risk paramount - aggressive cessation counseling
- Tibial fractures: Nonunion risk 4-8x - emphasize critical importance
- Femoral neck: AVN and nonunion risk - strongly advise cessation
This covers urgent/trauma scenarios.
Verification of Smoking Status
Objective Verification Methods
Biochemical Verification of Smoking Status
| Test | Marker | Sensitivity | Specificity | Half-Life | Clinical Use |
|---|---|---|---|---|---|
| Serum/urine cotinine | Nicotine metabolite | Very high | Very high | 16-20 hours | Gold standard for verification |
| Exhaled CO | Carbon monoxide | High | Moderate | 4-6 hours | Point-of-care, immediate result |
| Salivary cotinine | Nicotine metabolite | Very high | Very high | 16-20 hours | Non-invasive alternative |
| Urine anabasine | Tobacco alkaloid | High | Very high | Variable | Distinguishes tobacco from NRT |
When to Use Biochemical Verification:
- Research studies (standard requirement)
- High-stakes situations (e.g., prerequisite for elective surgery in some protocols)
- Suspected non-disclosure
- Generally NOT required for routine clinical care - patient self-report adequate
Cotinine Testing:
- Cutoff typically under 10 ng/mL = non-smoker
- Detects smoking in past 3-4 days
- False positives: Heavy secondhand smoke exposure
- Important: NRT use will cause positive cotinine (use anabasine to differentiate)
Exhaled CO Testing:
- Handheld device (e.g., Bedfont Smokerlyzer)
- Cutoff typically under 6-8 ppm = non-smoker
- Immediate result at point-of-care
- Short half-life (4-6 hours) - only detects very recent smoking
- False positives: Air pollution, COPD
Self-Report vs Verification
Evidence: Self-report of abstinence is reasonably accurate in most clinical settings. Biochemical verification adds little in routine practice but may be considered for:
- Research protocols
- Programs where cessation is prerequisite for intervention
- Suspected deception
Approach: Trust but verify when stakes are high (e.g., delaying elective surgery contingent on cessation).
Key Evidence for Smoking Cessation
Glassman et al. - Smoking Cessation and Spinal Fusion
- Retrospective review of 357 patients undergoing instrumented posterior lumbar fusion (L4-L5 or L4-S1)
- Nonunion 14.2% in nonsmokers vs 26.5% in patients who continued to smoke after surgery (p less than 0.05)
- Patients who quit for greater than 6 months postoperatively had a nonunion rate of 17.1%
- Return-to-work: 71% nonsmokers, 53% persistent smokers, 75% quitters; preoperative smoking quantity did not predict nonunion
Møller et al. - Preoperative Smoking Intervention (RCT)
- Multicentre RCT of 120 patients undergoing elective hip or knee replacement, randomised 6-8 weeks before surgery
- Overall complication rate 18% (intervention) vs 52% (control), p=0.0003
- Wound complications 5% vs 31% (p=0.001); cardiovascular complications 0% vs 10%
- Intervention was counselling plus nicotine replacement, aiming for cessation or at least 50% reduction
Scolaro et al. - Smoking and Fracture Healing (Systematic Review)
- Systematic review and meta-analysis of 19 cohort studies (7 prospective, 12 retrospective) on long-bone fractures
- Adjusted odds ratio of nonunion 2.32 (95% CI 1.76-3.06) in smokers overall
- Tibial fracture nonunion OR 2.16 (95% CI 1.55-3.01); open fracture nonunion OR 1.95
- Mean healing time longer in smokers (30.2 vs 24.1 weeks; not statistically significant)
Cahill et al. - Nicotine Receptor Partial Agonists (Cochrane)
- Cochrane review of 39 varenicline trials (25,290 participants)
- Varenicline (standard dose) vs placebo: pooled RR 2.24 (95% CI 2.06-2.43; high-quality evidence)
- Varenicline vs bupropion RR 1.39; varenicline vs NRT RR 1.25; number needed to treat ~11
- Nausea most common adverse effect; early neuropsychiatric concerns not confirmed (see EAGLES)
Singh et al. - Smoking and Arthroplasty Outcomes (Veterans)
- National Veterans Affairs cohort of 33,336 patients undergoing elective primary THA/TKA (2001-2008), multivariable-adjusted 30-day outcomes
- Current smokers vs never smokers: surgical site infection OR 1.41 (95% CI 1.16-1.72)
- Pneumonia OR 1.53, stroke OR 2.61, and 1-year mortality OR 1.63 in current smokers
- Prior smokers also had increased pneumonia, stroke, and urinary tract infection
Anthenelli et al. (EAGLES) - Neuropsychiatric Safety of Cessation Drugs
- Double-blind RCT of 8,144 smokers (half with stable psychiatric disorders) across 16 countries
- No significant excess of moderate-to-severe neuropsychiatric adverse events with varenicline or bupropion vs patch or placebo
- Varenicline most effective for confirmed abstinence (OR 3.61 vs placebo; 1.68 vs patch; 1.75 vs bupropion)
- Bupropion and nicotine patch both superior to placebo
Mills et al. - Cessation Reduces Postoperative Complications (Meta-analysis)
- Systematic review of 6 RCTs and 15 observational studies of preoperative smoking cessation
- Pooled RCT data: 41% relative risk reduction in postoperative complications (95% CI 15-59%)
- Each additional week of cessation increased the treatment effect by ~19%
- Trials of at least 4 weeks cessation showed significantly larger benefit; observational RR for total complications 0.76
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Preoperative Counseling for Spinal Fusion
"You are seeing a 52-year-old male smoker (40 pack-years, currently 1 pack per day) with degenerative spondylolisthesis L4/5 in your clinic. You have recommended L4/5 posterolateral fusion. How do you counsel him about smoking?"
Scenario 2: Acute Tibial Fracture in a Smoker
"A 35-year-old male smoker presents to the emergency department with a closed mid-shaft tibial fracture after a motorcycle accident. He smokes 15 cigarettes per day. You are planning surgical fixation with intramedullary nailing. How does his smoking status affect your management and counseling?"
Scenario 3: Smoking Cessation Pharmacotherapy Selection
"A 60-year-old female patient is scheduled for total knee arthroplasty in 3 months. She smokes 10 cigarettes per day and is motivated to quit. She has a history of depression treated with an SSRI and had a seizure 20 years ago related to alcohol withdrawal, but no seizures since. What pharmacotherapy do you recommend for smoking cessation?"
Scenario 4: Patient Refuses to Quit Smoking
"You have counseled a 45-year-old male smoker about the need to quit before his elective rotator cuff repair. He states he does not want to quit and becomes frustrated that you keep bringing it up. How do you proceed?"
MCQ Practice Points
Clinical Pearl
Q: What is the minimum recommended duration of preoperative smoking cessation to reduce wound healing complications?
A: Minimum 4 weeks (ideally 6-8 weeks). Wound complications (infection, dehiscence) are reduced by 50% after 4 weeks cessation. Carbon monoxide levels normalize within 24-48 hours, improving tissue oxygenation. Nicotine's vasoconstrictive effects persist for 2-4 weeks after cessation. Longer cessation periods show incremental benefit, but even brief cessation (24-48 hours) improves oxygenation.
Clinical Pearl
Q: By what factor does smoking increase the risk of nonunion following fracture fixation?
A: Smoking doubles (2x) the risk of nonunion. Studies show nonunion rates of 6-12% in smokers vs 3-6% in non-smokers. The mechanism involves impaired osteoblast function, reduced bone blood flow, and altered growth factor expression. The effect is dose-dependent. Smoking also increases infection risk (2x), DVT/PE (3-4x), and delays wound healing.
Clinical Pearl
Q: What is the most effective pharmacological intervention for smoking cessation in the perioperative period?
A: Varenicline (Champix) is most effective (quit rate approximately 25-30% at 12 months) but requires 1-2 week lead time. It is a partial nicotinic receptor agonist that reduces cravings and withdrawal symptoms. Nicotine replacement therapy (NRT) is second-line but can be started immediately. Bupropion is an option for patients with depression. Combination NRT (patch + rapid-acting) equals varenicline efficacy.
Clinical Pearl
Q: What is the impact of smoking on total hip arthroplasty outcomes?
A: Smokers have 2-3x higher risk of revision at 10 years. Specific complications: higher infection rate (superficial and deep), increased aseptic loosening, more frequent dislocation (due to poor soft tissue healing), and greater wound complications. Current smokers have worse patient-reported outcomes (PROMs). Smoking cessation before THA improves outcomes even with short cessation periods.
Clinical Pearl
Q: What counseling approach is recommended for smoking cessation intervention by orthopaedic surgeons?
A: Brief intervention using the 5A's model: Ask (smoking status), Advise (clear advice to quit), Assess (readiness to quit), Assist (pharmacotherapy referral, Quitline 13 7848), Arrange (follow-up). Brief advice (3-5 minutes) doubles quit rates. Documenting preoperative smoking status is mandatory. Linking cessation to surgical outcomes enhances motivation ("teachable moment").
Guidelines, Registries & Global Practice
Global Epidemiology
According to PubMed, the Global Burden of Disease Study 2019 estimated 1.14 billion current smokers worldwide in 2019, consuming 7.41 trillion cigarette-equivalents. Smoking accounted for 7.69 million deaths and 200 million disability-adjusted life-years, and was the leading risk factor for death among males (20.2% of male deaths). Age-standardised prevalence has fallen significantly since 1990 (males 27.5% reduction, females 37.7% reduction), but population growth means the absolute number of smokers has risen from 0.99 billion in 1990. [27]
Smoking Prevalence by Setting (Adults)
| Population | Approximate Prevalence | Source |
|---|---|---|
| Global adult (age-standardised) | Falling but ~20% in many regions | GBD 2019 |
| Australia (adults) | 10.6% daily smoking (2022-23) | AIHW NDSHS 2022-23 |
| UK (adults) | ~12-13% | ONS / NHS data |
| Orthopaedic trauma cohorts | 20-40% (higher than general) | Scolaro 2014 and cohort series |
| Aboriginal and Torres Strait Islander | ~40% (much higher) | AIHW |
Side-by-Side Guideline Comparison
Perioperative / Cessation Guidance Across Bodies
| Body (Region) | Core Recommendation | First-line Pharmacotherapy | Evidence Level |
|---|---|---|---|
| RACGP / eTG (Australia) | Brief intervention (Ask-Advise-Help) for all smokers; offer pharmacotherapy plus behavioural support | Varenicline, NRT, or combination NRT | Strong (Grade A) |
| NICE NG209 (UK) | Offer cessation support at every contact; varenicline/NRT/cytisine as options; treat tobacco dependence in all settings | Varenicline or combination NRT (cytisine an option) | Strong |
| US PHS / AAOS perioperative guidance | 5 A's; counsel and treat all surgical smokers; document status | Varenicline or combination NRT | Strong (RCT-supported) |
| WHO Framework Convention on Tobacco Control | Population-level control plus brief advice and pharmacotherapy access | NRT, varenicline, bupropion, cytisine | Strong |
| Cochrane / EAGLES evidence base | Varenicline most effective single agent; safe in stable psychiatric disease; combination NRT effective | Varenicline; combination NRT | Level I |
Practice Variation
The core principles converge globally: screen every patient, deliver brief advice, offer pharmacotherapy (varenicline or combination NRT first-line) plus behavioural support, and continue cessation through the bone-healing period. Variation lies mainly in reimbursement and access - the PBS in Australia, NHS-funded services in the UK, and out-of-pocket or insurance models elsewhere - rather than in the underlying clinical recommendation. Cytisine is widely available and inexpensive in parts of Eastern Europe and increasingly in the UK, but not in Australia.
Registry and Outcome Data
No dedicated smoking-cessation registry exists for orthopaedics, but national joint replacement registries inform the smoking-outcome link:
- The Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) and the National Joint Registry (NJR, UK) capture revision and infection outcomes against which modifiable risk factors such as smoking are analysed.
- Large cohort and registry-linked studies (e.g. Singh 2011, 33,336 arthroplasties) consistently show higher adjusted surgical site infection and mortality in current smokers, supporting preoperative cessation pathways.
Australian Resources (PBS, Quitline, eTG)
Quitline: 13 7848 - free, confidential, multilingual telephone counselling available across all Australian states and territories, with callback sessions and free NRT starter packs in some jurisdictions. Telephone counselling increases quit rates compared with self-directed quitting. [26]
PBS Coverage for Smoking Cessation
| Medication | PBS Status | Authority Required | Notes |
|---|---|---|---|
| Varenicline | Restricted benefit | May be required | Limited courses per year |
| Bupropion | Restricted benefit | May be required | Limited courses per year |
| NRT (patches, gum, lozenges) | General benefit | No | Multiple brands; also available over the counter |
Note: PBS restrictions and patient co-payments change periodically. Consult the current PBS schedule at pbs.gov.au for up-to-date prescribing requirements and authority thresholds.
Other Australian resources: RACGP "Supporting smoking cessation: a guide for health professionals" and Australian Therapeutic Guidelines (eTG) both endorse the brief-intervention framework with pharmacotherapy plus behavioural support; quitnow.gov.au and the My QuitBuddy app provide patient-facing support. The Tackling Indigenous Smoking (TIS) Program provides culturally appropriate, community-based support for Aboriginal and Torres Strait Islander peoples, in whom prevalence (~40%) is substantially higher.
References
-
Nolan J, Jenkins DH, Kurz LT, Horwitz DS. The acute management of the open fracture. J Orthop Trauma. 2009;23(suppl 1):S76-S91.
-
Fang MA, Frost PJ, Iida-Klein A, Hahn TJ. Effects of nicotine on cellular function in UMR 106-01 osteoblast-like cells. Bone. 1991;12(4):283-286.
-
Chen Y, Guo Q, Pan X, Qin L, Zhang P. Smoking and impaired bone healing: will activation of cholinergic anti-inflammatory pathway be the bridge? Int Orthop. 2011;35(10):1555-1561.
-
Silverstein P. Smoking and wound healing. Am J Med. 1992;93(1A):22S-24S.
-
Hernigou J, Schuind F. Tobacco and bone fractures: A review of the facts and issues that every orthopaedic surgeon should know. Bone Joint Res. 2013;2(11):255-265.
-
Jensen JA, Goodson WH, Hopf HW, Hunt TK. Cigarette smoking decreases tissue oxygen. Arch Surg. 1991;126(9):1131-1134.
-
Holt PG. Immune and inflammatory function in cigarette smokers. Thorax. 1987;42(4):241-249.
-
Mosely LH, Finseth F. Cigarette smoking: impairment of digital blood flow and wound healing in the hand. Hand. 1977;9(2):97-101.
-
Singh JA, Houston TK, Ponce BA, et al. Smoking as a risk factor for short-term outcomes following primary total hip and total knee replacement in veterans. Arthritis Care Res (Hoboken). 2011;63(10):1365-1374.
-
Namba RS, Inacio MC, Paxton EW. Risk factors associated with deep surgical site infections after primary total knee arthroplasty: an analysis of 56,216 knees. J Bone Joint Surg Am. 2013;95(9):775-782.
-
Lee SM, Landry J, Jones PM, Buhrmann O, Morley-Forster P. Long-term quit rates after a perioperative smoking cessation randomized controlled trial. Anesth Analg. 2015;120(3):582-587.
-
Glassman SD, Anagnost SC, Parker A, Burke D, Johnson JR, Dimar JR. The effect of cigarette smoking and smoking cessation on spinal fusion. Spine (Phila Pa 1976). 2000;25(20):2608-2615.
-
Andersen T, Christensen FB, Laursen M, Høy K, Hansen ES, Bünger C. Smoking as a predictor of negative outcome in lumbar spinal fusion. Spine (Phila Pa 1976). 2001;26(23):2623-2628.
-
Møller AM, Villebro N, Pedersen T, Tønnesen H. Effect of preoperative smoking intervention on postoperative complications: a randomised clinical trial. Lancet. 2002;359(9301):114-117.
-
Hernigou J, Schuind F. Smoking as a predictor of negative outcome in diaphyseal fracture healing. Int Orthop. 2013;37(5):883-887.
-
Scolaro JA, Schenker ML, Yannascoli S, Baldwin K, Mehta S, Ahn J. Cigarette smoking increases complications following fracture: a systematic review. J Am Acad Orthop Surg. 2014;22(5):295-304.
-
Calori GM, Albisetti W, Agus A, Iori S, Tagliabue L. Risk factors contributing to fracture non-unions. Injury. 2007;38 Suppl 2:S11-S18.
-
Singh JA, Houston TK, Ponce BA, Maddox G, Bishop MJ, Richman J, et al. Smoking as a risk factor for short-term outcomes following primary total hip and total knee replacement in veterans. Arthritis Care Res (Hoboken). 2011;63(10):1365-1374.
-
Singh JA. Smoking and outcomes after knee and hip arthroplasty: a systematic review. J Rheumatol. 2011;38(9):1824-1834.
-
Mallon WJ, Misamore G, Snead DS, Denton P. The impact of preoperative smoking habits on the results of rotator cuff repair. J Shoulder Elbow Surg. 2004;13(2):129-132.
-
Warner DO. Perioperative abstinence from cigarettes: physiologic and clinical consequences. Anesthesiology. 2006;104(2):356-367.
-
Cahill K, Lindson-Hawley N, Thomas KH, Fanshawe TR, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2016;(5):CD006103.
-
Anthenelli RM, Benowitz NL, West R, et al. Neuropsychiatric safety and efficacy of varenicline, bupropion, and nicotine patch in smokers with and without psychiatric disorders (EAGLES): a double-blind, randomised, placebo-controlled clinical trial. Lancet. 2016;387(10037):2507-2520.
-
Ramon JM, Nerin I, Comino A, Pinet C, Abella F, Carreras JM, et al. A multicentre randomized trial of combined individual and telephone counselling for smoking cessation. Prev Med. 2013;57(3):183-188.
-
Stead LF, Buitrago D, Preciado N, Sanchez G, Hartmann-Boyce J, Lancaster T. Physician advice for smoking cessation. Cochrane Database Syst Rev. 2013;(5):CD000165.
-
Stead LF, Hartmann-Boyce J, Perera R, Lancaster T. Telephone counselling for smoking cessation. Cochrane Database Syst Rev. 2013;(8):CD002850.
-
GBD 2019 Tobacco Collaborators. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990-2019: a systematic analysis from the Global Burden of Disease Study 2019. Lancet. 2021;397(10292):2337-2360.
Key Australian Guidelines
- Royal Australian College of General Practitioners (RACGP). Supporting smoking cessation: A guide for health professionals. Updated 2014.
- Australian Therapeutic Guidelines (eTG). Smoking Cessation. Accessed December 2025.
- Australian Institute of Health and Welfare (AIHW). National Drug Strategy Household Survey 2022.
Suggested Further Reading
- Møller AM, Pedersen T, Villebro N, Nørgaard P. Impact of lifestyle on perioperative smoking cessation and postoperative complication rate. Prev Med. 2003;36(6):704-709.
- Theadom A, Cropley M. Effects of preoperative smoking cessation on the incidence and risk of intraoperative and postoperative complications in adult smokers: a systematic review. Tob Control. 2006;15(5):352-358.
- Mills E, Eyawo O, Lockhart I, Kelly S, Wu P, Ebbert JO. Smoking cessation reduces postoperative complications: a systematic review and meta-analysis. Am J Med. 2011;124(2):144-154.
This comprehensive topic on smoking cessation for orthopaedic surgery is now complete.
Smoking Cessation - Exam Day Quick Reference
Clinical summary
Key Statistics to Memorize
- •Fracture nonunion: OR 2.32 in smokers (tibia OR 2.16) - Scolaro meta-analysis
- •Lumbar fusion nonunion: 26.5% persistent smokers vs 14.2% nonsmokers (Glassman)
- •Arthroplasty SSI: adjusted OR 1.41 in current smokers (Singh, n=33,336)
- •Cessation: 41% relative risk reduction in postop complications (Mills RCT pooled)
- •Minimum cessation: 4 weeks, optimal 8+ weeks preoperatively
- •Postoperative cessation: 12+ weeks for bone healing procedures
- •Varenicline: most effective single agent (RR 2.24 vs placebo, NNT ~11); NRT/bupropion double quit rate
- •Smoking prevalence: 1.14 billion globally (GBD 2019); ~10-13% adults in Australia/UK; 20-40% ortho trauma
Mechanisms of Smoking Harm
- •Osteoblast dysfunction: reduced proliferation, decreased alkaline phosphatase
- •Vasoconstriction: nicotine causes alpha-adrenergic stimulation and tissue hypoxia
- •Carbon monoxide: reduced oxygen delivery (competes with O2 for hemoglobin)
- •Impaired angiogenesis: reduced VEGF expression
- •Fibroblast impairment: reduced collagen synthesis
- •Immune dysfunction: reduced neutrophil function, complement activation
- •Dose-response: worse outcomes with higher pack-years
5 A's Framework
- •ASK: Screen all patients for tobacco use at every visit
- •ADVISE: Strongly urge to quit with personalized message
- •ASSESS: Determine willingness to make quit attempt
- •ASSIST: Help develop quit plan, provide pharmacotherapy, Quitline referral
- •ARRANGE: Schedule follow-up within 1 week of quit date
Pharmacotherapy Quick Reference
- •First-line: Varenicline (most effective, 3x quit rate, NNT=10)
- •Varenicline dosing: Start 1 week before quit date, 0.5mg to 1mg BID
- •Varenicline contraindications: Severe renal impairment, pregnancy
- •NRT: Safe perioperatively, continue through surgery, double quit rate
- •Combination NRT (patch + gum/lozenge) more effective than single
- •Bupropion: Contraindicated in seizure disorder, eating disorder
- •All PBS subsidized in Australia (varenicline/bupropion restricted benefit)
Procedure-Specific Approach
- •Spinal fusion: 8 weeks preop + 12+ weeks postop, highest pseudarthrosis risk
- •Fracture fixation: 4-8 weeks preop + 12+ weeks postop (bone healing period)
- •TJA: 4-8 weeks preop + 6-12 weeks postop, infection risk 3-6x
- •Acute trauma: Counsel to quit immediately, focus on 12-week postop period
- •Rotator cuff repair: Increased re-tear and infection risk
Documentation Essentials
- •Current smoking status and pack-years in every note
- •5 A's counseling provided (Ask, Advise, Assess, Assist, Arrange)
- •Procedure-specific risks discussed with patient
- •Pharmacotherapy prescribed (drug, dose, duration)
- •Quitline referral (13 7848) offered
- •Patient response: willing to quit / attempted / refused
- •If refused: informed consent about increased complication risk
Australian Context
- •Quitline: 13 7848 (free telephone counseling, evidence-based)
- •PBS subsidies: varenicline, bupropion (restricted), NRT (general)
- •AIHW 2022: 16.5% Australian adults smoke
- •Higher rates in Aboriginal/Torres Strait Islander peoples (39%)
- •eTG recommendations: 5 A's + pharmacotherapy for all smokers
High-Yield Exam Answers
- •Q: Most effective pharmacotherapy? A: Varenicline (3x quit rate)
- •Q: Minimum preop cessation? A: 4 weeks (optimal 8 weeks)
- •Q: Is NRT safe perioperatively? A: Yes - no combustion products, reduces relapse
- •Q: Patient refuses to quit - proceed? A: Yes if medically necessary, document counseling and informed consent
- •Q: Mechanism of smoking harm? A: Tissue hypoxia (vasoconstriction + CO), osteoblast dysfunction, impaired angiogenesis, immune dysfunction
- •Q: Evidence for cessation? A: 50% complication reduction with 6-8 week preop cessation + NRT