Solitary Plasmacytoma of Bone
A single biopsy-proven plasma-cell lesion, normal bone marrow, no other lesions on whole-body MRI/PET, and no CRAB end-organ damage. Treat with radiotherapy and survey long-term.
Clonal marrow plasma cells, additional lesions, or CRAB features mean the disease is systemic - it is multiple myeloma, needing systemic therapy, not localized RT alone. Mislabelling MM as solitary plasmacytoma undertreats the patient.
Overview & Spectrum
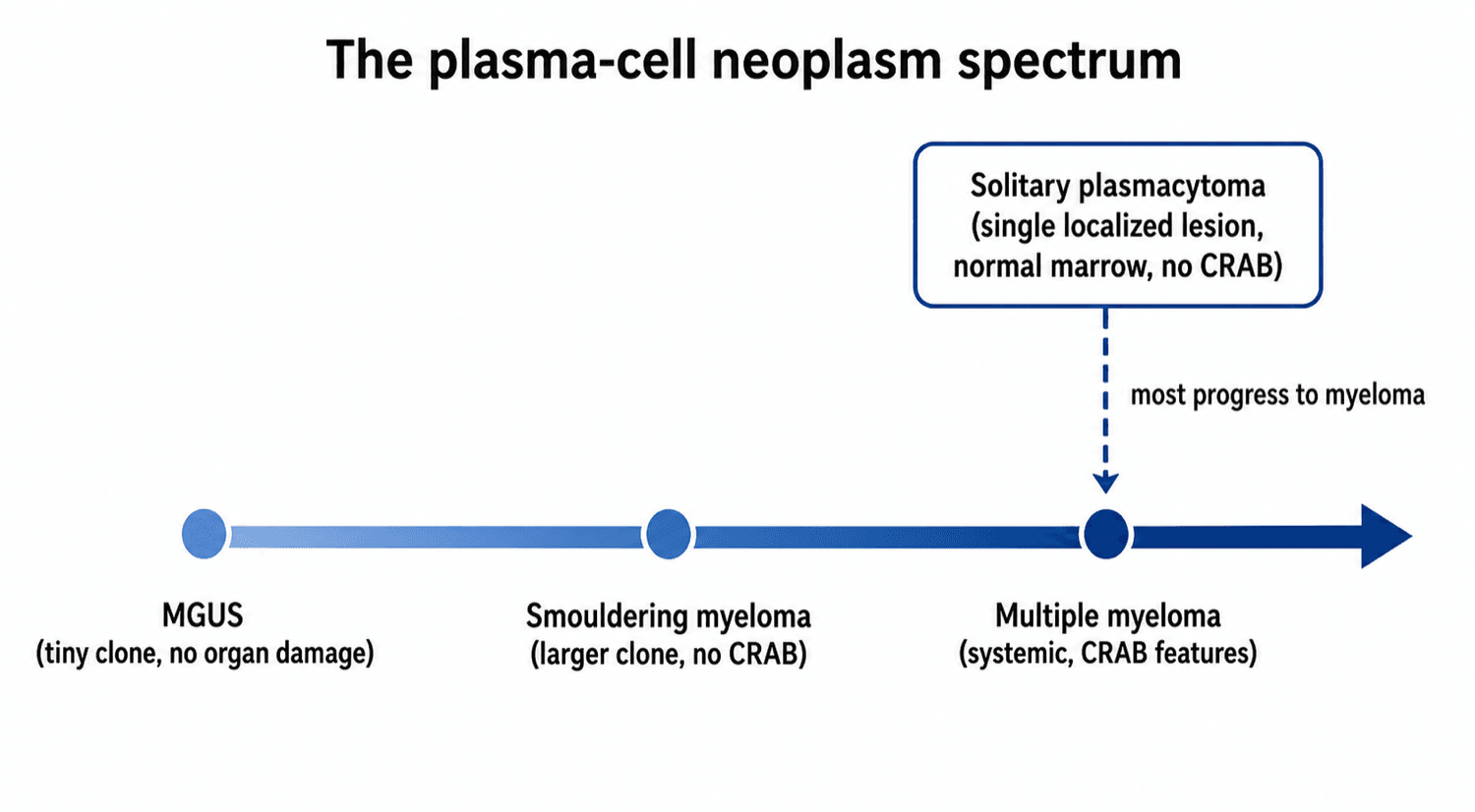
Solitary plasmacytoma is a rare neoplasm defined by a single, localized mass of clonal (monoclonal) plasma cells with no evidence of systemic disease. It is part of the plasma-cell neoplasm spectrum - the great majority (~95%) of which present as multiple myeloma. When the lesion is in bone it is a solitary bone plasmacytoma (SBP); when in soft tissue/extraosseous sites (commonly the head and neck) it is a solitary extramedullary plasmacytoma (SEP). SBP is more common than SEP and has a poorer prognosis because of its higher rate of progression to multiple myeloma, even though both respond well to treatment.
Pathophysiology & Epidemiology
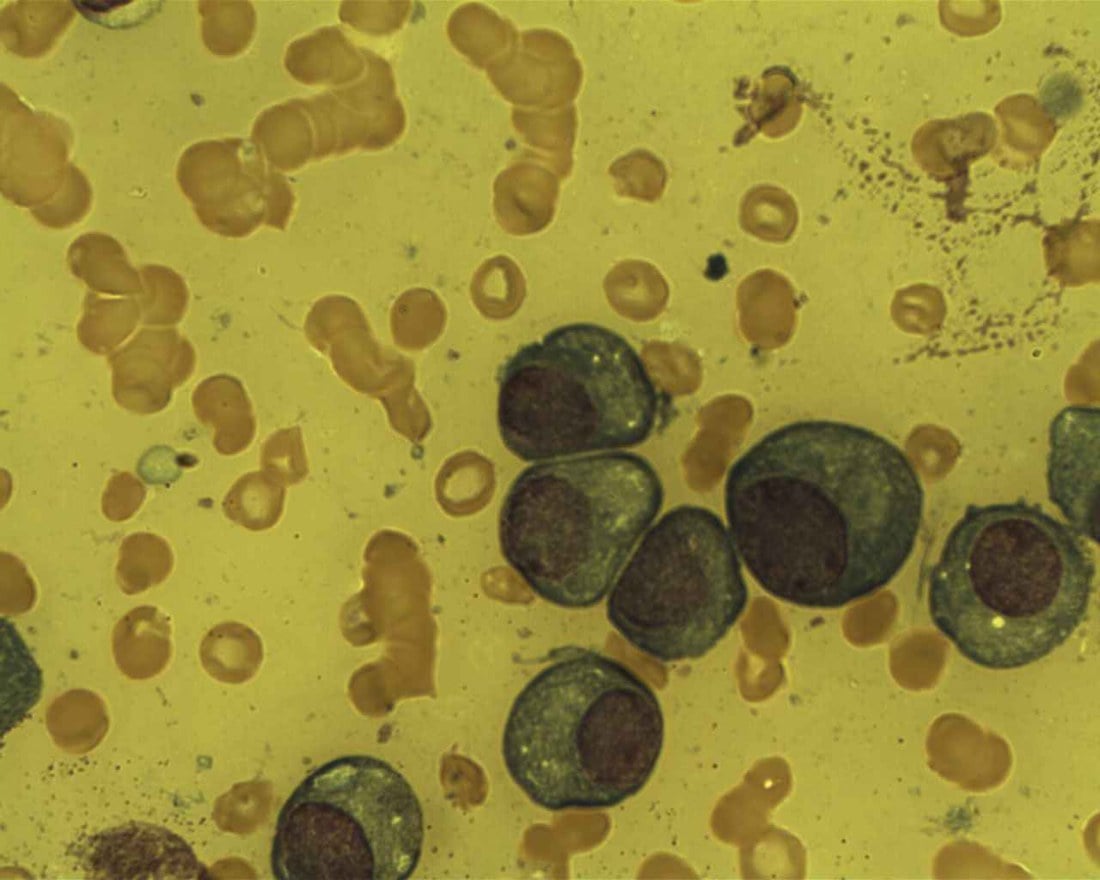
A solitary plasmacytoma is a localized expansion of a single clone of plasma cells - terminally differentiated B cells that normally secrete antibody. The clone usually produces a monoclonal immunoglobulin or light chain (the paraprotein / M-protein), which is why a small serum or urine paraprotein is often detectable even when the disease looks confined to one bone. The cells home to the bone marrow microenvironment, and the same osteoimmunological machinery that drives myeloma bone disease operates locally: plasma-cell-derived and stromal signals raise RANKL relative to OPG and other osteoclast-activating factors, so osteoclasts resorb bone faster than osteoblasts can repair it - producing the characteristic lytic ('punched-out') lesion and the risk of pathological fracture.
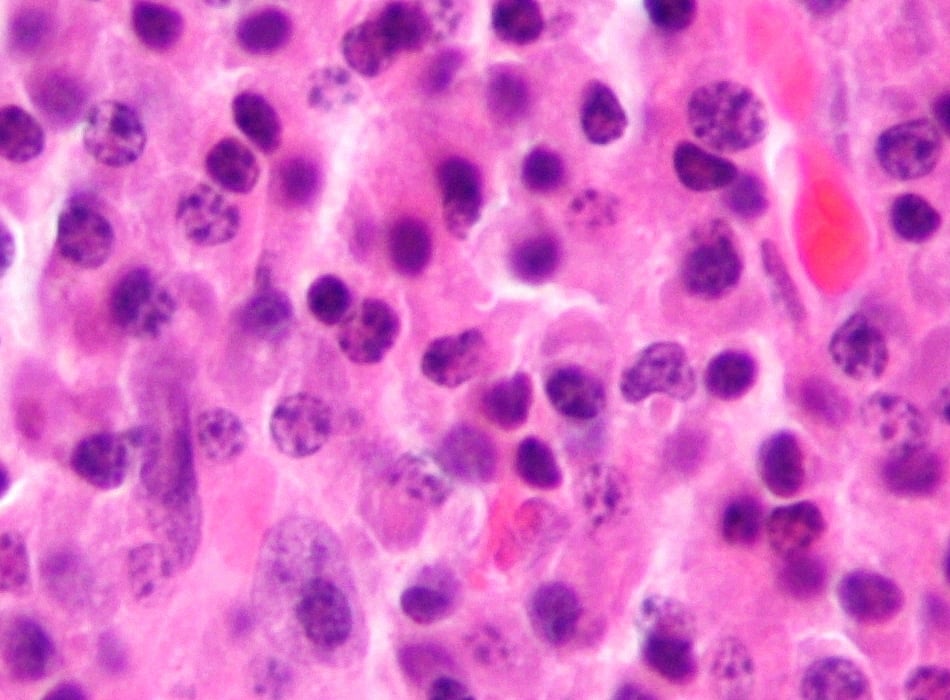
Proving clonality is what turns "plasma cells" into a neoplastic diagnosis. Plasma cells are CD138 (syndecan-1) positive on immunohistochemistry, and clonality is shown by light-chain restriction - the population expresses either kappa or lambda, not the normal polyclonal mix (assessed by immunohistochemistry, in-situ hybridisation or flow cytometry). The clone is typically CD19-negative and CD56-positive, distinguishing it from normal plasma cells.
Plasma-cell neoplasms form a continuum from MGUS (a tiny clone, no organ damage) through smouldering myeloma to multiple myeloma (systemic, with CRAB or myeloma-defining biomarkers). Solitary plasmacytoma sits apart as a localized clone. It is rare (well under ~500 cases a year in a country the size of the USA), tends to present a little younger than multiple myeloma (median around the early 60s), and is commoner in men. Solitary bone plasmacytoma is more common than the extramedullary form and, crucially, behaves as an early/limited-stage myeloma in many patients - which is why the defining clinical question is not "is this cancer?" but "is it really still localized?"
Presentation
- Bone pain at the lesion (often the spine, also pelvis/proximal long bones)
- Pathological fracture or vertebral collapse
- Spinal cord / nerve-root compression with a vertebral lesion
- Usually a slightly younger age than typical multiple myeloma; more common in men
- A solitary lytic ("punched-out") bone lesion, often well-defined
- MRI to define soft-tissue extent/cord involvement and screen the marrow
- Whole-body MRI or 18F-FDG PET-CT to confirm it is truly solitary (more sensitive than plain skeletal survey)

The hallmark above is a LYTIC lesion, but examiners love the exception — a plasmacytoma can be osteosclerotic, and that variant carries a named association:
- An osteosclerotic plasmacytoma (single or multiple sclerotic bony lesions) is the bone lesion of POEMS syndrome — Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal protein (characteristically a lambda light chain), and Skin changes — typically with a raised VEGF.
- The dominant clinical feature is a chronic progressive demyelinating peripheral neuropathy, so a patient with a sclerotic bone lesion, a small lambda paraprotein and a neuropathy should prompt the POEMS work-up rather than a "simple lytic plasmacytoma" label.
- Importantly, directing radiotherapy at a solitary osteosclerotic lesion can improve the polyneuropathy — so recognising the variant changes both the diagnosis and what the treatment is expected to achieve.
So when the lesion is sclerotic rather than punched-out, think POEMS and screen for the neuropathy/VEGF.
Investigations & Diagnostic Workup
Diagnosis of a solitary bone plasmacytoma requires all of:
- A single lesion of biopsy-proven clonal plasma cells.
- A normal bone marrow (no, or only minimal/limited, clonal plasma cells - more than a defined low threshold suggests myeloma).
- No other lesions on whole-body imaging (MRI/PET).
- No myeloma-related end-organ damage - i.e. no CRAB (hyperCalcaemia, Renal impairment, Anaemia, other Bone lesions). A small clonal marrow population with an otherwise solitary lesion is sometimes termed plasmacytoma with minimal marrow involvement and behaves more aggressively.
- Purpose
- Confirm clonal plasma cells (the diagnosis)
- Purpose
- Detect and quantify a paraprotein (M-protein)
- Purpose
- Sensitive clonality marker; prognostic if persistent
- Purpose
- Exclude systemic marrow clonal plasma cells
- Purpose
- Screen for CRAB (anaemia, hypercalcaemia, renal impairment)
- Purpose
- Confirm the lesion is truly solitary (more sensitive than skeletal survey)
A solitary lytic lesion in an adult is non-specific, so the examiner expects a structured differential before you commit to "plasmacytoma":
- Metastasis - the commonest lytic lesion over ~40 (lung, breast, kidney, thyroid); always consider a primary elsewhere.
- Multiple myeloma - the key plasma-cell mimic; the whole work-up above exists to separate it from solitary disease.
- Lymphoma of bone (and, in the right setting, leukaemic deposit).
- Primary bone tumour - e.g. giant cell tumour (epiphyseal, after physeal closure), and the aggressive primaries (osteosarcoma, Ewing sarcoma, chondrosarcoma) depending on age and site.
- Infection - subacute osteomyelitis / Brodie's abscess can mimic a lytic lesion.
- The decisive step is the same in every case: biopsy for tissue diagnosis plus staging to establish whether the lesion is solitary or part of systemic disease.
Management
Definitive radiotherapy to the lesion is the standard treatment for solitary plasmacytoma - it provides durable long-term local control in solitary bone plasmacytoma and is potentially curative in the extramedullary form (which has a lower tendency to disseminate). Treatment volumes and dose follow specialist (e.g. ILROG) guidance. Surgery is not the primary treatment of the tumour itself; it is reserved for structural indications - impending or actual pathological fracture, spinal instability, or neurological compromise requiring decompression/stabilisation - usually combined with RT. The role of systemic chemotherapy is debated and not routine for true solitary disease.
Definitive radiotherapy to the lesion is the standard treatment - it gives durable local control in solitary bone plasmacytoma (local control around 90% in modern series) and is potentially curative in the extramedullary form. Typical doses are in the region of 40-50 Gy, with volumes and dose/fractionation following specialist (ILROG) guidance. Always complete whole-body imaging first to be certain the disease is truly solitary before committing to localized RT.
When surgery IS indicated (impending/actual pathological fracture, spinal instability, cord compression), the orthopaedic principle differs from a routine metastasis:
- Build for a survivor. Plasmacytoma is radiosensitive and patients are often long-term survivors (5-year OS ~78%), so the reconstruction must be durable, not just palliative — stable internal fixation for a fixable fracture, and endoprosthetic/segmental replacement where bone destruction is too extensive to fix; in the spine, decompression with instrumented stabilisation (± cement augmentation/vertebroplasty for a contained vertebral lesion).
- Sequence surgery and RT. Radiotherapy is generally given after the surgical wound has healed (around 2-3 weeks postoperatively) to avoid wound-healing complications; for acute cord compression the priority is urgent decompression/stabilisation first, then RT to the lesion. Surgery never replaces the radiotherapy — the tumour is still irradiated.
- Don't forget the diagnosis comes first. If the lesion is undiagnosed, obtain tissue (and stage) before definitive fixation — fixing an unbiopsied lesion as if it were a simple fracture is the classic error.
Complications & Prognosis
Most patients with a solitary bone plasmacytoma will eventually progress to multiple myeloma (substantially more often than the extramedullary form), sometimes years later - around half within 5 years in bone disease. Persistence of the paraprotein after radiotherapy predicts progression. Patients therefore need long-term haematological follow-up (serial paraprotein/free light chains, blood counts, calcium/renal function, and imaging as indicated) - reassurance that they are "cured" after RT is unsafe.
- Detail
- Pathological fracture, vertebral collapse, spinal cord/nerve-root compression - the orthopaedic burden of the lesion
- Detail
- The dominant long-term risk: roughly half of bone SP at 5 years, far higher than extramedullary SP
- Detail
- Bone (vs extramedullary) site and a serum paraprotein at diagnosis; persistence of paraprotein after RT
- Detail
- Excellent with definitive radiotherapy (around 90%); local failure is uncommon
- Detail
- Radiotherapy field effects; surgical/anaesthetic risk when fixation or decompression is needed
Mnemonics & Memory Aids
SOLITARY
Hook:SOLITARY: prove it is single, exclude myeloma, irradiate, and watch it long-term.
PROVE
Hook:PROVE it is solitary before you treat: the work-up that excludes occult myeloma.
CRAB
Hook:No CRAB = compatible with solitary; any CRAB feature points to multiple myeloma.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old man has a painful solitary lytic lesion in a vertebra; biopsy shows clonal plasma cells. How do you confirm the diagnosis of solitary plasmacytoma, and why does it matter?”
“How would you treat a confirmed solitary bone plasmacytoma, when is surgery indicated, and what do you tell the patient about prognosis?”
Definition
- Single localized clonal plasma-cell tumour, no systemic disease
- Solitary bone (SBP) vs solitary extramedullary (SEP); SBP commoner, worse prognosis
- Part of the plasma-cell neoplasm spectrum (~95% present as MM)
Diagnosis
- Single biopsy-proven clonal lesion + normal marrow + no other lesions + no CRAB
- Workup: SPEP/UPEP + free light chains, FBC/Ca/renal, marrow biopsy, whole-body MRI/PET
- Whole-body MRI/PET more sensitive than skeletal survey
Management
- Radiotherapy = treatment of choice (durable local control; SEP potentially curative)
- Surgery only for fracture/instability/cord compression (+ RT)
- Chemotherapy role debated; not routine for true solitary disease
Prognosis
- High progression to multiple myeloma (more with SBP than SEP)
- Persistent paraprotein after RT predicts progression
- Needs long-term haematological surveillance
Evidence & Key Studies
Solitary plasmacytoma
- Solitary plasmacytoma is a localized clonal plasma-cell proliferation without systemic disease; solitary bone plasmacytoma is more common than the extramedullary form.
- Solitary bone plasmacytoma has poorer overall and progression-free survival than extramedullary disease because of its higher rate of evolution to multiple myeloma.
- Flow cytometry and MRI/18F-FDG PET refine diagnosis and exclude occult myeloma; radiotherapy is the treatment of choice, with the roles of surgery and chemotherapy still debated.
Radiation therapy for solitary plasmacytoma and multiple myeloma: guidelines from the International Lymphoma Radiation Oncology Group
- Definitive radiotherapy is the standard treatment for localized plasmacytoma; it provides long-term local control in solitary bone plasmacytomas and is potentially curative in extramedullary cases.
- Provides standardized work-up, target-volume and dose/fractionation recommendations for solitary plasmacytoma.
- Outlines the supportive (palliative) role of radiotherapy in multiple myeloma in the era of novel systemic agents.
The SBP-versus-SEP distinction and diagnostic refinements come from the Grammatico review (Grammatico et al., DOI), the role of radiotherapy from the ILROG guideline (Tsang et al., DOI), the myeloma-defining criteria used to exclude systemic disease from the IMWG consensus (Rajkumar et al., DOI), and the local-control and progression figures from the MD Anderson series (Reed et al., DOI). The diagnostic criteria (single lesion, normal marrow, no other lesions, no CRAB) follow standard plasma-cell-neoplasm definitions. (See also our Multiple Myeloma and Enneking Staging topics.)