Anterior/Posterior Spinal Arteries & the Artery of Adamkiewicz
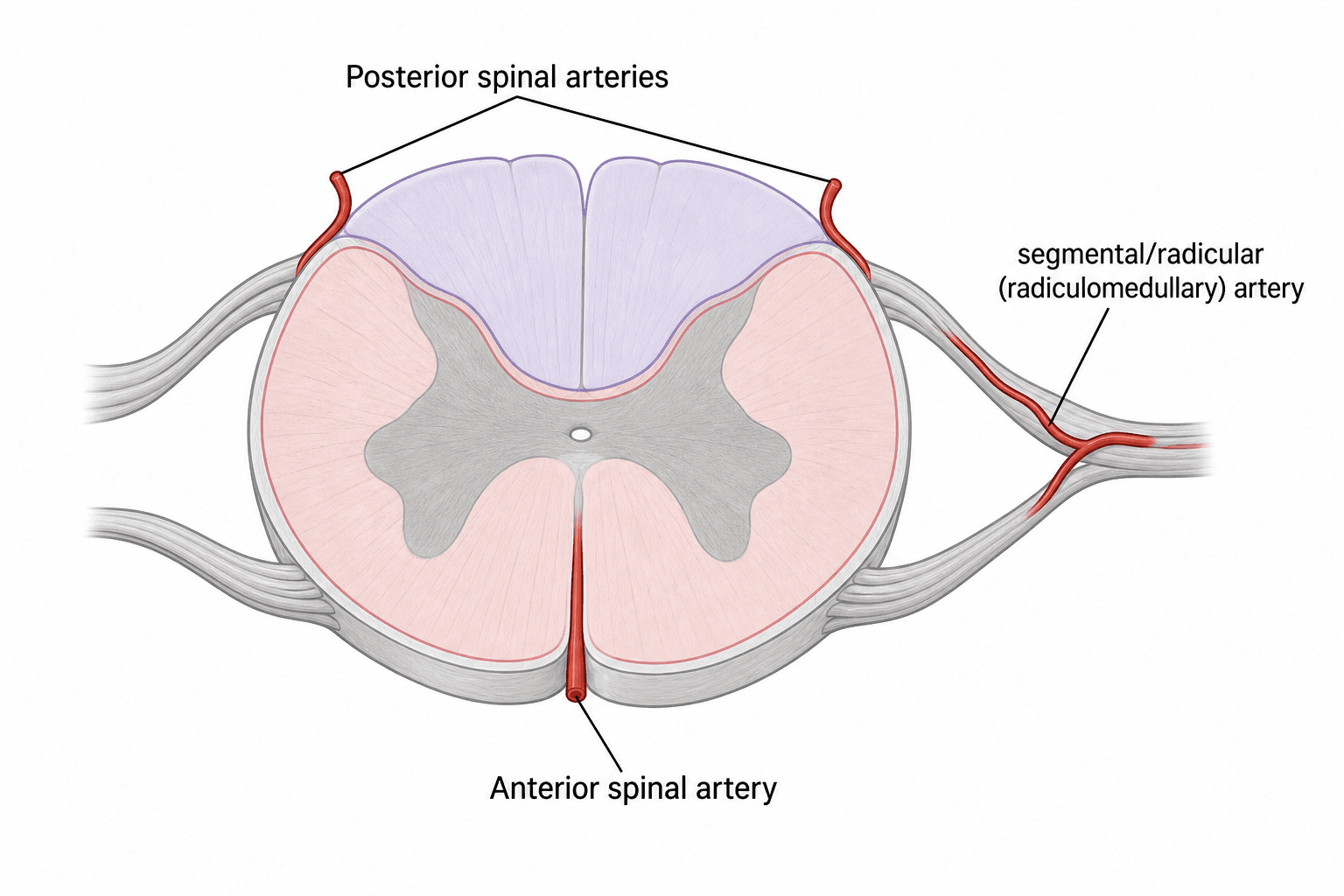
- The spinal cord is supplied by ONE ANTERIOR SPINAL ARTERY (in the anterior median fissure, formed from branches of the vertebral arteries) which feeds the ANTERIOR TWO-THIRDS of the cord, and TWO PAIRED POSTERIOR SPINAL ARTERIES (posterolateral) which feed the POSTERIOR ONE-THIRD (the dorsal columns).
- These longitudinal arteries are REINFORCED at intervals by SEGMENTAL (RADICULOMEDULLARY) arteries arising from the vertebral, posterior intercostal and lumbar arteries - so the cord is NOT fed by one continuous column but depends on these feeders, creating VULNERABLE WATERSHED zones (classically the MID-THORACIC cord, ~T4-T9).
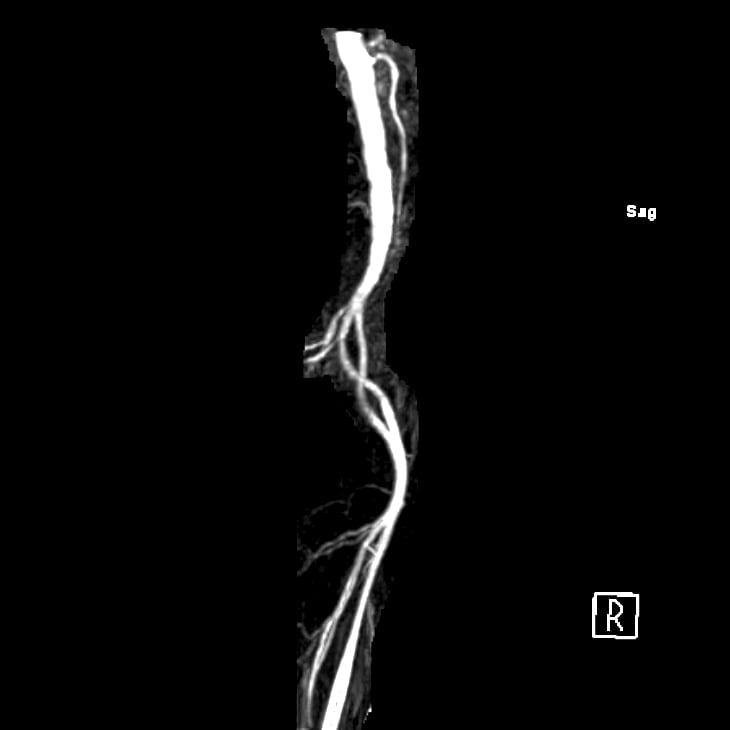
- The dominant feeder of the lower (thoracolumbar) cord is the ARTERY OF ADAMKIEWICZ (the great anterior radiculomedullary artery / arteria radicularis magna): it is present in ~85% of people, usually a SINGLE artery (~87%), most often on the LEFT (~77%), and arises between T8 and L1 (~89%) - it makes a characteristic 'HAIRPIN' as it joins the anterior spinal artery.
- Compromise of the ANTERIOR spinal artery (or the Adamkiewicz feeder) causes ANTERIOR SPINAL ARTERY (ANTERIOR CORD) SYNDROME: loss of MOTOR function and PAIN/TEMPERATURE below the level (corticospinal + spinothalamic tracts), with PRESERVED dorsal-column function (proprioception, vibration, light touch) - it has the WORST prognosis of the cord syndromes.
- This anatomy is critical in ORTHOPAEDICS and vascular surgery: correction of severe spinal DEFORMITY (especially kyphosis/vertebral column resection), thoracic/thoracolumbar spine surgery, and AORTIC (aneurysm/cross-clamp) surgery can injure the Adamkiewicz/anterior spinal supply and cause paraplegia - anterior spinal artery syndrome complicates ~0.1-0.2% of abdominal aortic operations.
- Protection relies on AWARENESS, maintaining adequate MEAN ARTERIAL PRESSURE/cord perfusion, avoiding prolonged ischaemia, and INTRAOPERATIVE NEUROMONITORING (MEP monitors the anterior/motor cord that the anterior spinal artery supplies).
- “1 anterior spinal artery = anterior 2/3 (motor + pain/temperature); 2 posterior spinal arteries = posterior 1/3 (dorsal columns).
- “Artery of Adamkiewicz: dominant thoracolumbar feeder - usually SINGLE, LEFT, T8-L1 (~85% present); a 'hairpin' joining the ASA.
- “Anterior cord syndrome (ASA territory): lose motor + pain/temperature, KEEP proprioception/vibration - worst prognosis; risk in deformity/aortic surgery (protect MAP + neuromonitor).
ONE vessel for the anterior two-thirds (corticospinal + spinothalamic tracts, anterior horns). A single artery with watershed dependence makes the anterior cord the vulnerable territory - hence anterior cord syndrome.
TWO vessels with a richer pial collateral plexus supply the posterior one-third (dorsal columns) - more resilient, so isolated posterior cord syndrome is rare.
The Arterial Anatomy
The cord has three longitudinal arteries: a single ANTERIOR SPINAL ARTERY running in the anterior median fissure (formed superiorly from branches of both vertebral arteries) supplying the anterior two-thirds of the cord, and two PAIRED POSTERIOR SPINAL ARTERIES on the posterolateral surface supplying the posterior one-third (dorsal columns). These longitudinal vessels are not sufficient on their own - they are reinforced segmentally by radiculomedullary (segmental) arteries from the vertebral, ascending/deep cervical, posterior intercostal and lumbar arteries, which enter via the intervertebral foramina along the nerve roots. Because reinforcement is intermittent, there are WATERSHED zones of relatively poor perfusion - classically the mid-thoracic cord (around T4-T9).
The Artery of Adamkiewicz
The artery of Adamkiewicz - the great anterior radiculomedullary artery (arteria radicularis magna) - is the dominant segmental feeder of the anterior thoracolumbar cord (the enlargement supplying the lumbar plexus). Its anatomy is high-yield because injuring it causes cord ischaemia: on meta-analysis it is present in ~85% of people, is usually a SINGLE vessel (~87%), arises most often on the LEFT (~77%), and originates between T8 and L1 in ~89% of cases (occasionally higher). It makes a characteristic 'HAIRPIN' turn as it ascends with a nerve root and then joins the anterior spinal artery (a recognisable sign on spinal angiography/MRA). Because it can arise over a range of levels and is usually solitary, it is vulnerable to inadvertent injury during thoracolumbar and aortic surgery.
Anterior Spinal Artery (Anterior Cord) Syndrome
Compromise of the anterior spinal artery (or its dominant feeder) infarcts the anterior two-thirds of the cord, producing ANTERIOR SPINAL ARTERY (ANTERIOR CORD) SYNDROME:
- LOST below the level: motor function (corticospinal tracts) and pain/temperature (spinothalamic tracts), with autonomic dysfunction (bladder/bowel).
- PRESERVED: proprioception, vibration and fine touch (dorsal columns - supplied by the posterior spinal arteries). It has the WORST prognosis of the incomplete cord syndromes. Causes include aortic surgery/ cross-clamping, profound hypotension, embolism/atheroma, thrombosis, and iatrogenic injury during spine deformity correction.
Anterior spinal artery syndrome complicates about 0.1-0.2% of abdominal aortic operations and is a feared complication of thoracic/thoracolumbar aortic repair and major spinal deformity correction (especially kyphosis correction and vertebral column resection, where the cord is shortened/manipulated and segmental vessels sacrificed). Protective measures: awareness of the Adamkiewicz anatomy (sometimes pre-operative angiographic localisation), maintaining an adequate MEAN ARTERIAL PRESSURE / cord perfusion, avoiding prolonged ischaemia, staged/limited vessel ligation, and intraoperative neuromonitoring - where motor evoked potentials specifically watch the anterior (motor) cord that the anterior spinal artery supplies.
The Venous Side: Batson's Plexus
The title promises the vascular anatomy, but the arteries are only half of it. The cord drains through anterior and posterior spinal veins into a pial venous plexus, then via radicular (medullary) veins into the internal vertebral venous plexus (Batson's plexus) in the epidural space; this communicates with the external vertebral plexus and the basivertebral veins draining the vertebral bodies, and freely with the segmental, azygos/hemiazygos, caval and pelvic veins.
The defining property is that this system is valveless and low-pressure, so flow can reverse - particularly when intra-abdominal or intrathoracic pressure rises (Valsalva, coughing, prone positioning). That explains three high-yield clinical points:
- Haematogenous spread: valveless retrograde flow lets pelvic/abdominal tumour (e.g. prostate, breast) and infection (pyogenic discitis / vertebral osteomyelitis) reach the spine - the classic explanation for vertebral and pelvic metastasis.
- Epidural venous bleeding: engorgement of the plexus - worsened by abdominal compression in the prone position - causes troublesome bleeding in spine surgery, which is why patients are positioned to keep the abdomen free (frame/bolsters) to decompress the plexus.
- Collateral return when the inferior or superior vena cava is obstructed.
The cord and spine drain via the valveless internal/external vertebral venous plexus (Batson's), communicating with the caval/azygos/pelvic veins - retrograde flow spreads pelvic/abdominal tumour and infection to the spine, and engorgement (prone abdominal compression) causes epidural bleeding, so keep the abdomen free.
Vertebral-Body Supply & Safe Segmental Ligation
The title also covers the vertebral column, and the safety advice to "limit and stage vessel sacrifice" needs the underlying anatomy. Each posterior intercostal/lumbar segmental artery runs around the vertebral body and gives periosteal/nutrient branches to the vertebral body, branches to the posterior elements and paraspinal muscles, and a spinal (radicular) branch that enters the foramen and supplies the radiculomedullary feeder to the cord (the dominant anterior one being the artery of Adamkiewicz).
In anterior/lateral thoracolumbar approaches the segmental vessels over the vertebral bodies are ligated to expose the spine. To avoid cord ischaemia:
- Ligate over the mid-vertebral body, away from the foramen, preserving the foraminal anastomosis and collateral network.
- Avoid sacrificing multiple consecutive segmentals, and especially the segmental carrying the Adamkiewicz feeder.
- In high-risk cases, temporarily clamp the segmental vessels and check neuromonitoring before permanent ligation, and maintain mean arterial pressure.
The vertebral body itself has a rich collateral supply and tolerates segmental ligation - but the cord does not if its dominant feeder is lost. (Intraoperative neuromonitoring detail is covered in our Spinal Cord Monitoring topic; the point here is the segmental anatomy and where to ligate.)
Each segmental (intercostal/lumbar) artery supplies the vertebral body, posterior elements and the radiculomedullary cord branch. In anterior thoracolumbar surgery ligate over the mid-vertebral body (not the foramen), avoid consecutive or Adamkiewicz-carrying segmentals, and temporarily clamp with neuromonitoring before dividing in high-risk cases.
Mnemonics & Memory Aids
1-AND-2
Hook:ONE anterior (2/3), TWO posterior (1/3) - and Adamkiewicz feeds the anterior thoracolumbar cord.
ADAM-LEFT
Hook:ADAMkiewicz is on the LEFT (mostly), single, T8-L1, the dominant thoracolumbar feeder.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the arterial blood supply of the spinal cord and the artery of Adamkiewicz. Why does this matter in spinal and aortic surgery?”
“What is anterior spinal artery syndrome, how does it present, and how would you reduce the risk during major spinal deformity surgery?”
Arteries
- 1 anterior spinal artery (anterior median fissure) -> anterior 2/3 (corticospinal + spinothalamic)
- 2 posterior spinal arteries (posterolateral) -> posterior 1/3 (dorsal columns)
- Segmental radiculomedullary feeders reinforce them -> watershed (mid-thoracic T4-T9)
Artery of Adamkiewicz
- Great anterior radiculomedullary artery; dominant thoracolumbar feeder
- Present ~85%; usually single (~87%); LEFT (~77%); T8-L1 (~89%)
- Hairpin turn joining the anterior spinal artery (angiography/MRA)
Anterior cord syndrome
- Lose motor + pain/temperature below level; KEEP proprioception/vibration
- Worst prognosis of incomplete cord syndromes
- Causes: aortic surgery/cross-clamp, hypotension, embolism, deformity correction
Protection
- Awareness (+/- pre-op Adamkiewicz localisation in aortic/complex cases)
- Maintain MAP/cord perfusion; avoid prolonged ischaemia; limit vessel sacrifice
- Intraoperative neuromonitoring (MEP watches the anterior/motor cord)
Evidence & Key Studies
Artery of Adamkiewicz: a meta-analysis of anatomical characteristics
- Across 60 studies (5437 subjects), the artery of Adamkiewicz was present in 84.6% of people.
- It was most frequently a SINGLE artery (87.4%), on the LEFT side (76.6%), originating between T8 and L1 (89%).
- Because it supplies the major anterior thoracolumbar cord and is usually solitary, surgeons operating in the thoracolumbar region must understand its anatomy to avoid spinal-cord ischaemia.
Mechanisms and prevention of anterior spinal artery syndrome following abdominal aortic surgery
- Anterior spinal artery syndrome is the most common neurological complication after abdominal aortic surgery, with an incidence of 0.1-0.2%.
- Aetiological factors include intra-operative hypotension, embolisation and prolonged aortic cross-clamping, all acting via altered spinal-cord blood supply.
- The anterior spinal artery, the great radicular artery of Adamkiewicz and the pelvic collateral circulation are central to cord perfusion; complete recovery is uncommon, so awareness and prevention are key.
The Adamkiewicz prevalence/laterality/level data come from the cited Taterra meta-analysis, and the anterior-spinal-artery-syndrome incidence and aetiology from the cited Aydin review. The anterior/posterior spinal artery territories, the watershed concept, and the anterior-cord-syndrome pattern are standard, well-established neuroanatomy. (See also our Spinal Cord Injury / Cord Syndromes and Spinal Cord Monitoring topics.)