ASIA Classification | MAP 85-90 | No Steroids | Early Surgery
ASIA IMPAIRMENT SCALE
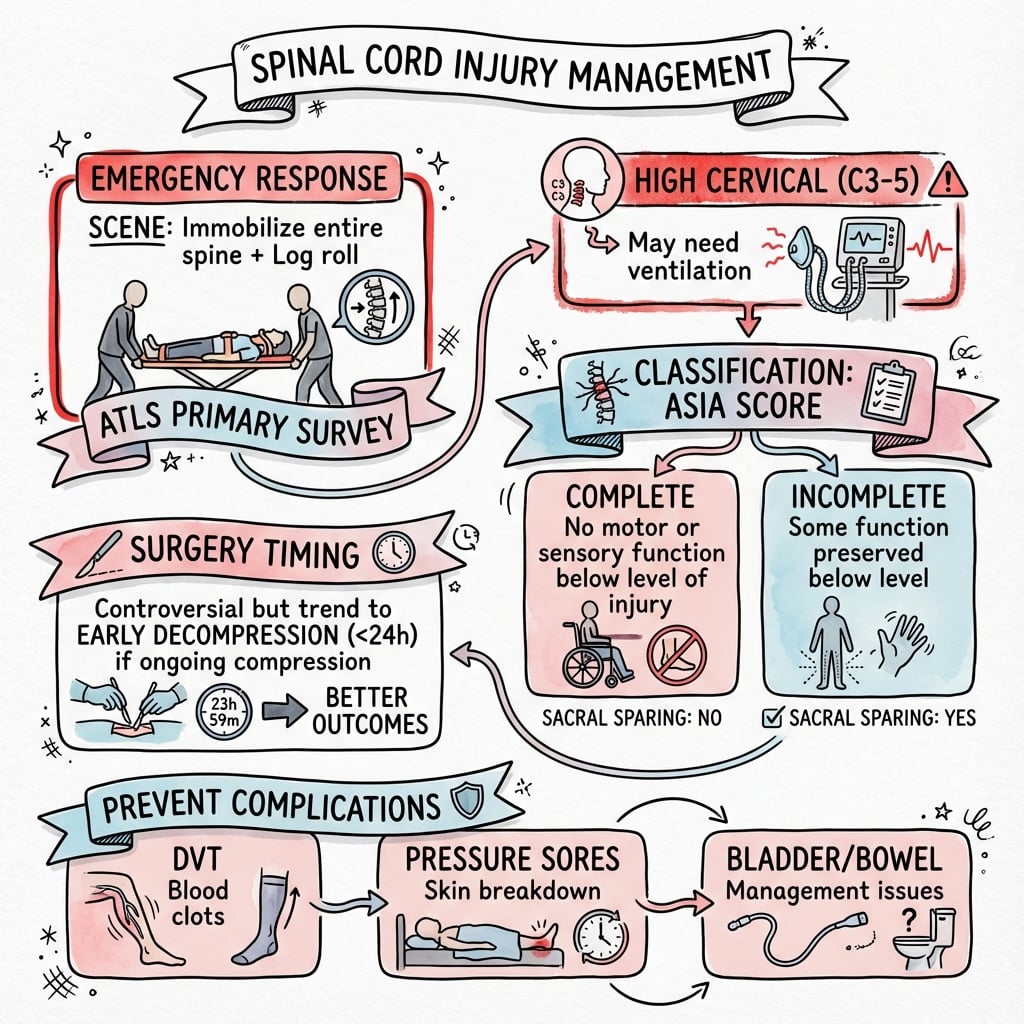
Critical Must-Knows
- ASIA classification is THE standard for neurological assessment in SCI
- MAP 85-90mmHg for 7 days improves outcomes in incomplete SCI
- Methylprednisolone is NOT recommended (NASCIS trials flawed)
- Early surgery (within 24h) for incomplete SCI improves outcomes
- Complete SCI (ASIA A) has poor prognosis regardless of treatment
Clinical Pearls
- "Neurogenic shock = bradycardia + hypotension (loss of sympathetic tone)
- "Spinal shock = transient areflexia, NOT hypotension
- "Sacral sparing = incomplete injury (better prognosis)
- "Bulbocavernosus reflex return signals end of spinal shock
Clinical Imaging
Imaging Gallery




Critical Spinal Cord Injury Exam Points
ASIA Grading
American Spinal Injury Association scale from A-E. ASIA A = complete (no motor or sensory below level). ASIA B-D = incomplete (sacral sparing present). ASIA B = sensory only. ASIA C = motor less than 3. ASIA D = motor 3 or more.
Neurogenic vs Spinal Shock
Neurogenic shock = cardiovascular (hypotension + bradycardia) from loss of sympathetic tone. Spinal shock = neurological (areflexia below injury level). Spinal shock ends when bulbocavernosus reflex returns.
Methylprednisolone
No longer recommended. NASCIS II/III trials were flawed (post-hoc analysis). Guidelines now recommend AGAINST steroids in SCI. If asked in exam, know the controversy and current stance.
MAP Goals
Maintain MAP 85-90mmHg for 5-7 days in incomplete SCI. This ensures adequate spinal cord perfusion. Use vasopressors (norepinephrine) if needed. Critical for preventing secondary injury.
Quick Decision Guide
| ASIA Grade | Definition | Prognosis | Management Priority |
|---|---|---|---|
| ASIA A (Complete) | No motor/sensory below level | Less than 5% motor recovery | Stabilization, prevent secondary injury |
| ASIA B (Incomplete) | Sensory only, no motor | 50% regain walking ability | Urgent surgery if compression |
| ASIA C (Incomplete) | Motor grade less than 3 | 75% improve one grade | Priority for early decompression |
| ASIA D (Incomplete) | Motor grade 3 or more | 95% maintain walking | Surgery based on instability |
ASIAASIA Impairment Scale
| A | Absent function Complete injury, no motor/sensory below |
| B | Below sensory only Incomplete, sensory preserved |
| C | Cannot move well Motor less than grade 3 |
| D | Decent motor Motor grade 3 or more |
| E | Everything normal Full recovery |
| A | Absent function Complete injury, no motor/sensory below | D | Decent motor Motor grade 3 or more |
| B | Below sensory only Incomplete, sensory preserved | E | Everything normal Full recovery |
| C | Cannot move well Motor less than grade 3 |
Hook:ASIA A is complete and BAD prognosis. ASIA B-D are incomplete with better outcomes!
SPINALSpinal Shock Signs
| S | Sphincter tone absent Loss of anal tone |
| P | Peripheral reflexes absent Below injury level |
| I | Injury level flaccidity No spasticity yet |
| N | No bulbocavernosus reflex Initially absent |
| A | Areflexia below injury Transient loss |
| L | Lasts 24-72 hours typically Resolves with reflex return |
| S | Sphincter tone absent Loss of anal tone | I | Injury level flaccidity No spasticity yet | A | Areflexia below injury Transient loss |
| P | Peripheral reflexes absent Below injury level | N | No bulbocavernosus reflex Initially absent | L | Lasts 24-72 hours typically Resolves with reflex return |
Hook:SPINAL shock is neurological (areflexia), NOT cardiovascular - ends when bulbocavernosus returns!
MAPMAP Goals for SCI
| M | Maintain blood pressure Prevent secondary injury |
| A | Aim for 85-90 mmHg Target range for 5-7 days |
| P | Perfuse the cord Vasopressors if needed |
| M | Maintain blood pressure Prevent secondary injury |
| A | Aim for 85-90 mmHg Target range for 5-7 days |
| P | Perfuse the cord Vasopressors if needed |
Hook:MAP 85-90 for 7 days prevents secondary cord injury from hypoperfusion!
Overview and Epidemiology
Definition
Spinal cord injury (SCI) is damage to the spinal cord resulting in temporary or permanent changes to motor, sensory, or autonomic function below the level of injury. The distinction between complete (ASIA A) and incomplete (ASIA B-E) injuries is crucial for prognosis.
Etiology
Mechanism of Injury:
- Motor vehicle accidents (39%)
- Falls (31%) - increasing in elderly
- Violence (14%) - gunshot wounds predominant
- Sports (8%) - diving injuries common
- Medical/surgical complications (5%)
Level Distribution:
- Cervical (55%) - most common, worst outcomes
- Thoracic (30%) - high velocity injuries
- Lumbar (15%) - often associated with burst fractures
Bimodal Age Distribution
Two peaks: Young adults (15-29 years) from trauma, and elderly (over 65 years) from falls with pre-existing cervical stenosis. The elderly population is growing as a proportion of SCI patients.
Global Burden
Global incidence of traumatic SCI is roughly 8 to 50 per million per year, with the highest rates in regions with high road-traffic and fall burdens. Wherever you practise, the principle is the same: rapid transfer to a specialist spinal cord injury centre with retrieval-service support improves outcomes. Document a clear baseline neurological examination before transfer.
Anatomy and Pathophysiology
Spinal Cord Anatomy
Key Anatomical Points:
- Cord ends at L1-L2 (conus medullaris)
- Cervical cord enlargement (C4-T1) for upper limb
- Lumbar enlargement (L1-S2) for lower limb
- Central grey matter (motor anterior, sensory posterior)
- Peripheral white matter (tracts)
Spinal Cord Tracts
Major Spinal Cord Tracts
| Tract | Function | Location | Clinical Syndrome |
|---|---|---|---|
| Corticospinal (lateral) | Motor - voluntary movement | Lateral column | Weakness below level |
| Spinothalamic (lateral) | Pain and temperature | Anterior-lateral | Contralateral loss |
| Dorsal columns | Proprioception, vibration | Posterior column | Ipsilateral loss |
| Autonomic tracts | Sympathetic/parasympathetic | Intermediolateral | Neurogenic shock |
Pathophysiology of Injury
Primary Injury:
- Mechanical disruption at time of trauma
- Compression, contusion, transection
- Not reversible
Secondary Injury (Preventable):
- Ischemia from hypotension (target MAP 85-90)
- Edema and inflammation
- Excitotoxicity (glutamate release)
- Apoptosis (programmed cell death)
- Occurs over hours to days
Secondary Injury Prevention
The goal of acute SCI management is to prevent secondary injury. This is achieved through: MAP goal 85-90mmHg, early decompression if compressed, avoiding hypoxia, and maintaining normothermia. The primary injury is done - focus on preventing further damage.
Classification
American Spinal Injury Association Impairment Scale
The standard classification for SCI worldwide:
ASIA A - Complete:
- No motor or sensory function in sacral segments S4-S5
- No voluntary anal contraction
- No perianal sensation
- Prognosis: less than 5% regain functional ambulation
ASIA B - Incomplete (Sensory Only):
- Sensory function preserved below level including S4-S5
- No motor function below level
- Prognosis: 50% regain some walking ability
ASIA C - Incomplete (Motor less than 3):
- Motor function preserved below level
- Half of key muscles below level have grade less than 3
- Prognosis: 75% improve at least one ASIA grade
ASIA D - Incomplete (Motor 3 or more):
- Motor function preserved below level
- Half or more of key muscles grade 3 or greater
- Prognosis: 95% maintain community ambulation
ASIA E - Normal: Full motor and sensory function. May have abnormal reflexes.
Differential Diagnosis
The patient who cannot move their limbs after trauma is not always a structural cord injury. Distinguishing true SCI from its mimics changes management entirely, and confusing complete with incomplete patterns alters prognosis and surgical urgency.
Differentiating SCI from Its Mimics
| Condition | Key Distinguishing Features | Sacral Function | Imaging / Test |
|---|---|---|---|
| Complete SCI (ASIA A) | No motor or sensory below level, including S4-S5 | Absent | MRI: cord disruption, haemorrhage |
| Incomplete SCI (ASIA B-D) | Any preserved function below level | Preserved (sacral sparing) | MRI: oedema, compression, partial signal |
| Spinal shock (phase, not diagnosis) | Transient global areflexia and flaccidity | May be temporarily absent | Clinical: BCR returns as it resolves |
| SCIWORA | Neurological deficit with normal radiographs/CT | Variable | MRI shows cord signal change |
| Cauda equina syndrome | LMN signs, saddle anaesthesia, retention; lesion below L1-L2 conus | Often impaired | MRI: canal compression below conus |
| Conus medullaris syndrome | Mixed UMN/LMN, early bladder/bowel, symmetrical | Impaired early | MRI: T12-L2 cord/conus lesion |
| Non-traumatic myelopathy | No trauma; infection, tumour, infarct, transverse myelitis | Variable | MRI with contrast; CSF; bloods |
| Functional / non-organic | Non-anatomical, inconsistent, normal reflexes/tone | Preserved | Normal MRI; inconsistent examination |
SCIWORA
Spinal Cord Injury WithOut Radiographic Abnormality is classically a paediatric phenomenon (ligamentous laxity, large head, horizontal facets) but also occurs in adults with pre-existing cervical stenosis. Plain films and CT are normal; MRI is mandatory and may show cord oedema or haemorrhage. A normal CT does NOT exclude cord injury in a patient with neurological signs.
Clinical Assessment
Primary Survey
- Airway: C-spine controlled, may need intubation
- Breathing: Diaphragm function (C3-5), assess respiratory
- Circulation: Neurogenic shock? Bradycardia, hypotension
- Disability: GCS, pupils, gross neuro
- Exposure: Complete spine exam, log roll
ASIA Examination
- Motor: 10 key muscles bilaterally (0-5 scale)
- Sensory: Light touch + pinprick at 28 dermatomes
- Sacral sparing: Perianal sensation, voluntary anal contraction
- Reflexes: Bulbocavernosus for spinal shock
- Document clearly: Neurological level and ASIA grade
Key Examination Findings
Neurogenic Shock:
- Hypotension (loss of sympathetic vascular tone)
- Bradycardia (unopposed parasympathetic to heart)
- Warm, dry peripheries (vasodilation)
- Occurs with lesions above T6
- NOT the same as spinal shock
Spinal Shock:
- Transient areflexia below injury level
- Flaccid paralysis (even if complete injury)
- Absent bulbocavernosus reflex initially
- Resolves over 24-72 hours typically
- Reflex return signals end of spinal shock
Sacral Sparing = Incomplete Injury
Always check for sacral sparing - perianal sensation and voluntary anal contraction. Any sacral function preserved means incomplete injury (ASIA B or better), which has significantly better prognosis than complete injury.
Investigations
MRI Findings and Prognosis
| MRI Finding | Description | Prognostic Significance |
|---|---|---|
| Hemorrhage | T1 hyperintense, T2 variable | Poor prognosis - irreversible damage |
| Edema only | T2 hyperintense, normal T1 | Better prognosis - may recover |
| Cord transection | Complete cord disruption | Complete injury, no recovery |
| Compression without signal | Mechanical compression, normal cord | Best prognosis if decompressed |
MRI Timing
MRI should not delay resuscitation or surgery in unstable patients. However, for incomplete injuries with unclear pathology, MRI within 24 hours helps guide surgical planning. Hemorrhage on MRI predicts poor outcome regardless of ASIA grade.
Management
Initial Management Priorities
Immobilization:
- Rigid cervical collar until cleared
- Log roll precautions
- Spinal board for transport only (pressure injury risk)
Airway and Breathing:
- Early intubation if GCS impaired or respiratory compromise
- C5 injury and above may need ventilatory support
- Avoid neck extension during intubation (fiber-optic if available)
Circulation - MAP Goals:
- Arterial line for continuous monitoring
- Target MAP 85-90mmHg for 5-7 days
- Vasopressors (norepinephrine first line)
- Avoid hypotension at all costs - causes secondary injury
NO Methylprednisolone: Previously given based on NASCIS trials but now recognized as flawed evidence. Current guidelines recommend AGAINST steroids due to no proven benefit and potential harm (infection, GI bleed).
Surgical Technique
Anterior Cervical Decompression and Fusion
Indications:
- Anterior compression (disc herniation, vertebral body)
- Corpectomy required
- Kyphotic deformity
Technique: Position supine with head in neutral. Approach through Smith-Robinson interval (medial to SCM). Perform discectomy or corpectomy as required. Decompress spinal cord under microscope. Place structural graft or cage. Apply anterior plate. Confirm alignment on fluoroscopy.
Advantages: Direct anterior decompression, restoration of lordosis.
Risks: Recurrent laryngeal nerve, esophageal injury, dysphagia.
Complications
Complications of Spinal Cord Injury
| Complication | Timeframe | Prevention/Management |
|---|---|---|
| Respiratory failure | Acute | Early intubation if C5+, pulmonary toilet |
| DVT/PE | Days to weeks | LMWH + mechanical, IVC filter if needed |
| Pressure ulcers | Days to weeks | Turn q2h, specialty mattress, early mobilization |
| Autonomic dysreflexia | Chronic (T6+) | Identify and remove noxious stimulus |
| Heterotopic ossification | Weeks to months | NSAIDs prophylaxis, radiation if high risk |
| Spasticity | Chronic | Physiotherapy, baclofen, botulinum toxin |
Autonomic Dysreflexia
Medical emergency in chronic SCI above T6. Caused by noxious stimulus below injury (full bladder, constipation). Presents with hypertension, bradycardia, headache, sweating. Treatment: sit upright, identify and remove trigger. May need antihypertensives if severe.
Postoperative Care
Early Rehabilitation
Transfer to spinal rehabilitation unit as soon as medically stable. Multidisciplinary care (physio, OT, psychology, social work) significantly improves functional outcomes. Most neurological recovery occurs in first 6-12 months.
Outcomes and Prognosis
Neurological Recovery
ASIA A (Complete):
- Less than 5% regain functional ambulation
- Recovery plateaus within 1 year
- Focus is on maximizing function at level of injury
ASIA B (Sensory Incomplete):
- 50% regain some walking ability
- Better prognosis than complete injury
- Early surgery may improve outcomes
ASIA C (Motor Incomplete):
- 75% improve at least one ASIA grade
- Most will achieve some ambulation
- Priority for early decompression
ASIA D (Good Motor):
- 95% maintain community ambulation
- Excellent functional prognosis
MRI Hemorrhage = Poor Prognosis
Cord hemorrhage on MRI is the strongest predictor of poor outcome, regardless of initial ASIA grade. Edema without hemorrhage has better recovery potential.
Controversies and Areas of Uncertainty
SCI management contains several genuinely unresolved questions. Examiners reward a candidate who can articulate both sides rather than reciting a single dogmatic answer.
Methylprednisolone: dead or optional?
Most bodies (AANS/CNS, Congress of Neurological Surgeons) recommend against routine steroids. The 2017 AOSpine guideline is more nuanced: it suggests a 24-hour high-dose infusion may be offered as an option within 8 hours of injury, while recommending against starting after 8 hours and against any 48-hour regimen. Bottom line: not standard of care, but not universally prohibited.
How early is early surgery?
STASCIS supports decompression within 24 hours. Emerging data and meta-analyses argue for an even tighter less than 8 to 12 hour "ultra-early" window, especially for cervical injuries. The counter-argument is logistical feasibility and the risk of operating on a haemodynamically unstable patient.
Optimal MAP target and duration
MAP 85-90 mmHg for 5-7 days is widely cited but rests on small case series, not RCTs. Some argue the threshold should be individualised using spinal cord perfusion pressure (MAP minus intrathecal pressure) measured via an intrathecal catheter, an investigational approach.
Central cord syndrome timing
Traditional teaching favoured conservative management given good spontaneous recovery. The 2017 AOSpine guideline now suggests early surgery as an option even in central cord syndrome, though on low-quality evidence. Practice remains genuinely divided.
Neuroprotection and regeneration
Riluzole, hepatocyte growth factor, anti-Nogo antibodies, cell-based therapies and CSF drainage are all under investigation. None is established standard of care. A safe exam answer: "Current management is supportive and surgical; pharmacological neuroprotection and regenerative therapies remain experimental."
Evidence Base and Key Trials
NASCIS II: Methylprednisolone or Naloxone in Acute SCI
- Multicentre double-blind RCT: 487 patients (162 methylprednisolone, 154 naloxone, 171 placebo)
- Primary analysis: no overall benefit of methylprednisolone or naloxone
- Post-hoc subgroup: benefit only when methylprednisolone started within 8 hours
- Mortality and major morbidity similar across groups
NASCIS III: 24h vs 48h Methylprednisolone vs Tirilazad
- Double-blind RCT: 499 patients across 16 North American SCI centres
- All received a 30 mg/kg bolus; then 24h or 48h methylprednisolone, or 48h tirilazad
- 48h regimen gave modest motor gains only in the post-hoc 3-8 hour subgroup
- 48h regimen increased severe sepsis and severe pneumonia
STASCIS: Early vs Delayed Decompression in Cervical SCI
- Prospective multicentre cohort: 313 patients with acute cervical SCI
- Early (less than 24h, mean 14.2h) vs late (mean 48.3h) decompression
- At 6 months, 19.8% of early vs 8.8% of late patients improved by 2 or more AIS grades
- Adjusted odds of 2-grade AIS improvement 2.8 times higher with early surgery; complication rates similar
AOSpine Guideline: Methylprednisolone in Acute SCI
- GRADE-based systematic review and multidisciplinary guideline
- No difference in motor score change overall with methylprednisolone vs no steroid
- Suggests NOT offering 24h high-dose MPSS to patients presenting after 8 hours
- Suggests a 24h infusion MAY be offered within 8 hours as an option; recommends against any 48h regimen
AOSpine Guideline: Timing of Decompression (incl. Central Cord)
- GRADE-based guideline on surgical timing (24h or less vs over 24h)
- Suggests early surgery be offered as an option for acute SCI regardless of level
- Suggests early surgery be considered as an option in traumatic central cord syndrome
- Quality of evidence rated low for both recommendations
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
"A 25-year-old male is brought to ED after a diving accident. He has no motor or sensory function below C5 level. His BP is 80/50 and heart rate is 48. How would you manage this patient?"
"A 68-year-old man with known cervical spondylosis falls backwards and presents with weakness affecting his upper limbs more than lower limbs. Describe the syndrome and management."
"Discuss the evidence for and against methylprednisolone in acute spinal cord injury."
"A 30-year-old man with a chronic complete T4 spinal cord injury presents with a sudden severe pounding headache, flushing and sweating above the level of injury, and a blood pressure of 200/110. What is happening and how do you manage it?"
MCQ Practice Points
ASIA A Definition Question
Q: What defines an ASIA A spinal cord injury? A: Complete injury with no motor or sensory function below the level, including S4-S5. Less than 5% will regain functional ambulation regardless of treatment timing.
Sacral Sparing Question
Q: What is the clinical significance of sacral sparing after spinal cord injury? A: Sacral sparing indicates incomplete injury (ASIA B or better). Check perianal sensation, deep anal pressure, and voluntary anal contraction. Prognosis is significantly better than complete injury.
Neurogenic vs Spinal Shock Question
Q: What is the difference between neurogenic shock and spinal shock? A: Neurogenic shock = cardiovascular (hypotension + bradycardia from sympathetic loss). Spinal shock = neurological (areflexia and flaccidity below level). They often coexist but are distinct entities.
MAP Goals Question
Q: What is the target MAP in acute spinal cord injury and for how long? A: MAP 85-90 mmHg for 5-7 days to optimize spinal cord perfusion and prevent secondary ischemic injury. Norepinephrine is preferred vasopressor.
Methylprednisolone Question
Q: What is the current recommendation regarding methylprednisolone in acute SCI? A: NOT recommended. NASCIS trials were methodologically flawed with post-hoc analysis only. Current AANS/CNS guidelines recommend against routine steroid use.
Incomplete Syndrome Prognosis Question
Q: Which incomplete SCI syndrome has the best and worst prognosis? A: Best: Brown-Sequard syndrome (90% ambulatory). Worst: Anterior cord syndrome (only 10-20% recovery; only dorsal columns spared). Central cord has intermediate but favorable prognosis.
Guidelines, Registries & Global Practice
Global Epidemiology
- Reported incidence of traumatic SCI varies widely, roughly 8 to 50 per million population per year, reflecting differences in road safety, violence and ascertainment.
- Bimodal age distribution: young adults (high-energy trauma) and an expanding elderly group (low-energy falls on a stenotic, often degenerate cervical spine).
- Worldwide the cervical spine is the commonest level injured, and males predominate, though the elderly fall cohort narrows this gap.
- High-income settings have seen falling SCI prevalence (Global Burden of Disease 2017 reported a decline in US SCI prevalence), while road-traffic SCI remains a major and rising burden in many low- and middle-income countries.
Major Guidelines Side by Side
How the Major Bodies Compare
| Issue | AOSpine / AANS-CNS (2017) | Practical Global Position |
|---|---|---|
| Methylprednisolone | AOSpine: 24h within 8h is an option only, no 48h. AANS/CNS: not recommended | Not standard of care anywhere; if used, only a 24h course within 8h with informed consent |
| Timing of surgery | Early decompression (within 24h) suggested regardless of level | Decompress within 24h where resources allow; ultra-early (under 12h) increasingly favoured for cervical injury |
| Haemodynamic target | Maintain MAP to support cord perfusion (commonly 85-90 mmHg, 5-7 days) | Avoid hypotension and hypoxia above all; individualise duration |
| MRI | Recommended to assess cord, ligaments and compression | Obtain MRI before or soon after surgery where available; never delay resuscitation |
| VTE prophylaxis | Pharmacological prophylaxis recommended once safe | Combined mechanical and LMWH; very high VTE risk in SCI |
High-Resource vs Limited-Resource Practice
High-Resource Settings
- Rapid pre-hospital retrieval to a dedicated spinal cord injury unit
- Around-the-clock MRI and emergency decompression capability
- ICU haemodynamic monitoring and arterial-line MAP targeting
- Multidisciplinary rehabilitation and long-term community reintegration
Limited-Resource Settings
- Emphasis on prevention (road safety, fall prevention) and safe transfer
- Decompression timing constrained by theatre and imaging access
- Pressure-injury and bladder care become dominant survival determinants
- Outcomes hinge on basic nursing, catheter care and contracture prevention
Transfer Considerations
Early transfer to a specialised spinal cord centre improves outcomes worldwide. Contact retrieval services early for cervical and complete injuries, maintain spinal precautions and MAP support in transit, and document a clear baseline neurological examination for handover.
SPINAL CORD INJURY
Clinical summary
ASIA Classification
- •A = Complete (no motor/sensory S4-S5)
- •B = Sensory only incomplete
- •C = Motor incomplete (less than grade 3)
- •D = Motor incomplete (grade 3+)
- •E = Normal
Neurogenic vs Spinal Shock
- •Neurogenic: Hypotension + bradycardia (cardiovascular)
- •Spinal: Areflexia below level (neurological)
- •Spinal shock ends when bulbocavernosus returns
- •Neurogenic shock occurs with T6 and above injuries
Acute Management
- •MAP 85-90mmHg for 5-7 days
- •NO methylprednisolone (NASCIS flawed)
- •Early surgery within 24h for incomplete SCI
- •DVT prophylaxis essential
Incomplete Syndromes
- •Central cord: UL worse than LL, best prognosis
- •Brown-Sequard: Hemisection, good prognosis
- •Anterior cord: Worst prognosis (dorsal spared)
- •Posterior cord: Rare, proprioception loss
Prognosis by ASIA Grade
- •ASIA A: Less than 5% functional ambulation
- •ASIA B: 50% regain walking
- •ASIA C: 75% improve one grade
- •ASIA D: 95% maintain community walking