- SINS predicts spinal instability from neoplastic disease and guides whether to refer for surgical stabilisation.
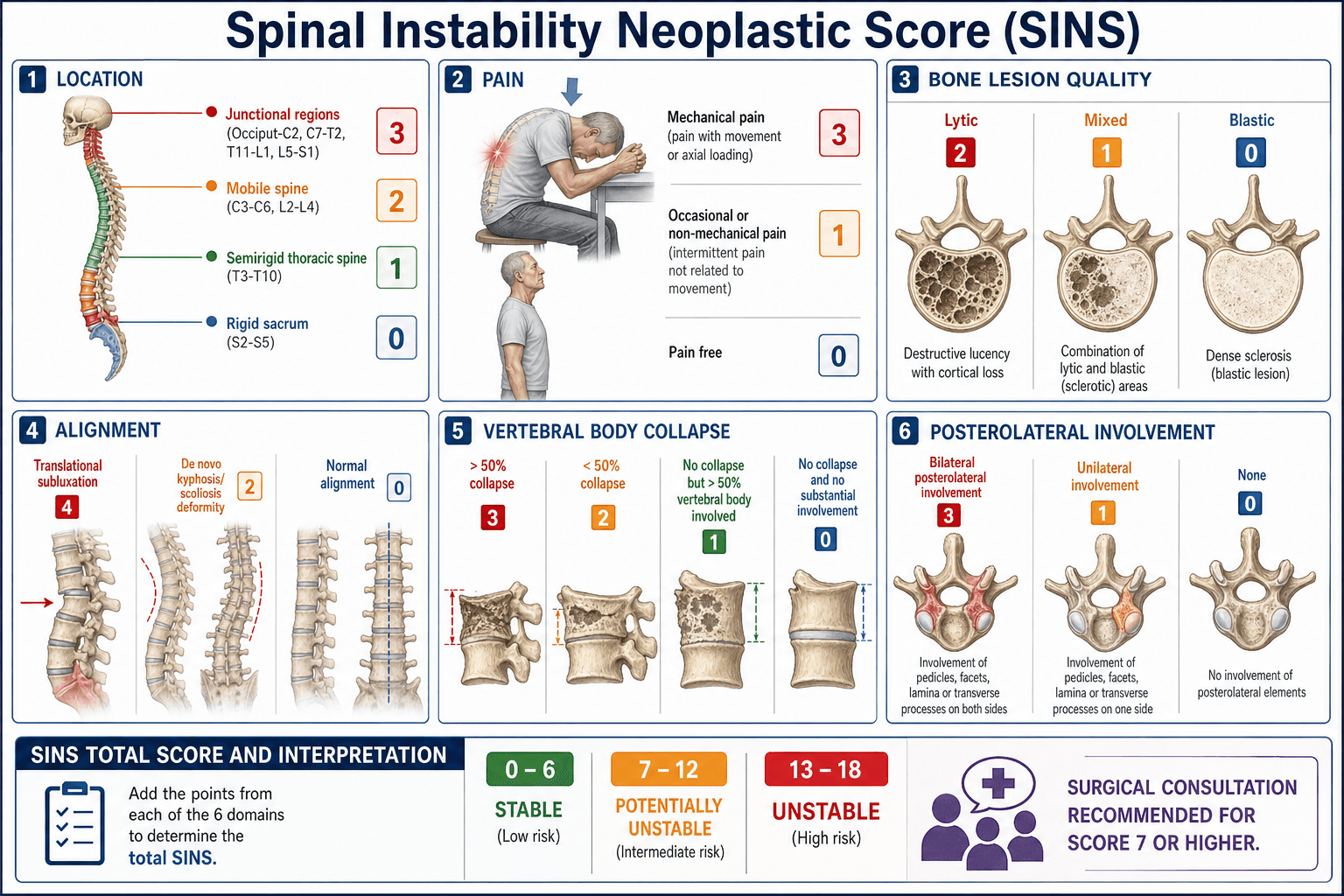
- Six parameters: location (0–3), pain (0–3), bone lesion (0–2), alignment (0–4), vertebral body collapse (0–3), posterolateral involvement (0–3). The highest-risk values are junctional location, mechanical pain, lytic lesion, subluxation, greater than 50 percent collapse, and bilateral posterolateral involvement.
- Act on the total: 0–6 stable (radiotherapy or observe), 7–12 indeterminate (consider surgery or close monitoring), 13–18 unstable (surgical referral).
- Mechanical pain and junctional location are the strongest single predictors — a patient with mechanical pain at the thoracolumbar junction almost always warrants surgical discussion regardless of the remaining arithmetic.
A SINS score of 13 or greater is an indication for surgical referral for stabilisation. A score of 0–6 is stable and can usually be managed non-operatively with radiotherapy, bracing or observation. Scores of 7–12 are indeterminate and require individualised multidisciplinary discussion; many of these patients benefit from surgery if they have mechanical pain, reasonable life expectancy and good performance status. Always remember that SINS addresses mechanical stability only — it does not replace oncological staging or assessment of neurological deficit.
The SINS Scoring System
Each of the six variables is scored from 0 up to a maximum of 4 points. The total (0–18) stratifies the degree of instability.
| Variable | 0 points | 1 point | 2 points | 3 points | 4 points |
|---|---|---|---|---|---|
| Location | Rigid (S2–S5) | Semi-rigid (T3–T10) | Mobile (C3–C6, L2–L4) | Junctional (occiput–C2, C7–T2, T11–L1, L5–S1) | |
| Pain | Pain-free | Occasional non-mechanical | Mechanical (movement-related) | ||
| Bone lesion | Blastic | Mixed | Lytic | ||
| Alignment | Normal | Deformity (kyphosis or scoliosis) | Subluxation or dislocation | ||
| Vertebral body collapse | None | No collapse but greater than 50 percent body involved | Less than 50 percent collapse | Greater than 50 percent collapse | |
| Posterolateral involvement | None | Unilateral | Bilateral |
Location • Pain • Lesion • Alignment • Collapse • PosterolateralThe six variables
Stable 0–6 • Indeterminate 7–12 • Unstable 13–18Stability thresholds
Mechanical pain is pain that is provoked by movement, axial loading or change in position and relieved by recumbency. It is the single most important clinical predictor of instability and scores the maximum three points. Constant tumour-related pain that does not vary with activity scores only one point.
Score Interpretation and Action
| Total Score | Stability | Recommended Action | Key Consideration |
|---|---|---|---|
| 0–6 | Stable | Radiotherapy, bracing or observation | Reassess if new mechanical pain or neurological change develops |
| 7–12 | Indeterminate | Individualised MDT discussion | Consider surgery if mechanical pain, solitary metastasis, good performance status or expected survival greater than three months |
| 13–18 | Unstable | Surgical referral for stabilisation | Surgery before radiotherapy when possible; protect the construct with post-operative radiotherapy |
Surgical stabilisation of an unstable neoplastic spine is technically easier and safer before a pathological fracture or progressive deformity occurs. The purpose of SINS is to identify patients who will benefit from early surgical consultation rather than waiting for frank instability or neurological deterioration.
Limitations and Modern Context
- SINS is a stability score only. It does not incorporate neurological deficit, systemic disease burden, life expectancy or radiosensitivity of the tumour. These factors must be weighed separately in the MDT.
- Inter-observer reliability is moderate to good for the total score but lower for individual components such as alignment and posterolateral involvement; always confirm radiographic findings with a spine surgeon.
- The score was derived and validated predominantly in patients with solid-tumour metastases. Haematological malignancies (myeloma, lymphoma) may behave differently and often respond dramatically to radiotherapy or systemic therapy.
- Modern separation surgery plus stereotactic body radiotherapy (SBRT) has changed the threshold for surgery in many centres; patients with high SINS scores but limited life expectancy may still be managed with radiotherapy alone after careful discussion.
- SINS does not replace clinical judgement. A patient with a score of 10 who has intractable mechanical pain and a solitary metastasis may be offered surgery, while a patient with a score of 14 who is moribund may appropriately receive palliative care only.
Evidence Base
A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group
- Original derivation and reliability study introducing the six-parameter SINS in 30 patients with spinal metastases
- Inter-observer and intra-observer reliability were substantial for total score and for the binary stable-versus-unstable decision
- Junctional location, mechanical pain and greater than 50 percent collapse emerged as the strongest predictors of perceived instability
Spinal instability neoplastic score: an analysis of reliability and validity from the spine oncology study group
- Prospective validation across 12 international centres confirming substantial reliability of the total SINS
- A threshold of 13 or greater identified patients judged to require surgical stabilisation with high sensitivity
- The indeterminate category (7–12) captured the majority of cases where surgical judgement varied most between observers
Reliability of the spinal instability neoplastic scale among radiologists: an assessment of instability secondary to spinal metastases
- Radiologist reliability study showing substantial agreement on total SINS and on the stable-versus-unstable binary classification
- The alignment and posterolateral involvement components had the lowest inter-observer agreement
- Radiologists tended to score slightly lower than surgeons on the same images
Spinal Instability Neoplastic Score component validation using patient-reported outcomes
- Validation study linking individual SINS components to patient-reported outcomes in spinal metastases
- Mechanical pain and junctional location showed the strongest correlation with worse quality of life scores
- Higher total SINS predicted greater functional impairment and need for intervention
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 58-year-old man with known renal-cell carcinoma presents with new thoracolumbar pain. MRI shows a lytic lesion at T12 with 40 percent vertebral body collapse and unilateral pedicle involvement. He reports pain that is worse when standing and walking but settles when he lies flat. What is his SINS score and what is your recommendation?”
“A 72-year-old woman with breast cancer and known bone metastases has a SINS score of 14 at L1 with greater than 50 percent collapse, bilateral posterolateral involvement and mechanical pain. She has lower-limb weakness (ASIA D) and a life expectancy estimated at four months. What factors influence your surgical decision?”
The six variables and points
- Location: rigid S2–S5 (0), semi-rigid T3–T10 (1), mobile C3–C6 or L2–L4 (2), junctional (3)
- Pain: pain-free (0), occasional non-mechanical (1), mechanical (3)
- Bone lesion: blastic (0), mixed (1), lytic (2)
- Alignment: normal (0), deformity (2), subluxation or dislocation (4)
- Vertebral body collapse: none (0), greater than 50 percent body involved no collapse (1), less than 50 percent collapse (2), greater than 50 percent collapse (3)
- Posterolateral involvement: none (0), unilateral (1), bilateral (3)
Stability thresholds and action
- 0–6 stable: radiotherapy, brace or observe; reassess if pain or neurology changes
- 7–12 indeterminate: MDT discussion; surgery if mechanical pain, good prognosis or solitary lesion
- 13–18 unstable: surgical referral for stabilisation; operate before radiotherapy when feasible
- Always factor in neurology, life expectancy and performance status alongside the numeric score
Key clinical pearls
- Mechanical pain is the strongest predictor and scores three points
- Junctional levels (especially T11–L1) carry higher instability risk than semi-rigid thoracic segments
- Bilateral posterolateral involvement and greater than 50 percent collapse drive high scores
- SINS addresses only mechanical stability — combine with neurological examination and oncological staging