Congenital undescended scapula with cosmetic deformity, limited abduction and important associated anomalies
- Sprengel deformity is failure of normal scapular descent, leaving the scapula high, small, rotated and often tethered to the cervical spine.
- Do not treat it as an isolated shoulder problem until cervical spine, scoliosis, rib, renal and cardiac associations have been considered.
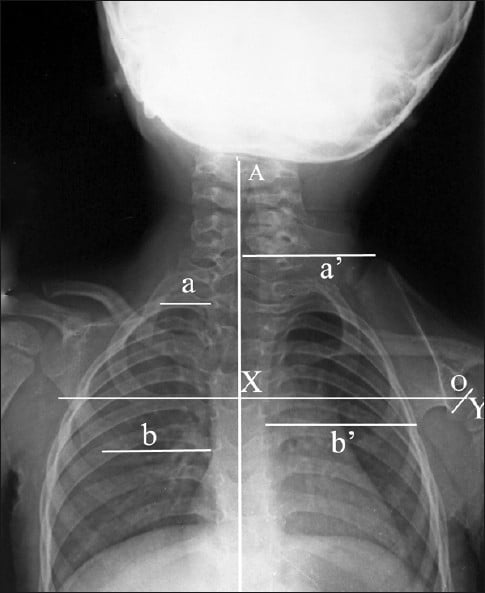
- Cavendish grade describes clinical appearance; Rigault classification describes radiographic vertical position of the scapula.
- The main functional loss is shoulder abduction because scapulothoracic rotation is restricted and the scapula is tethered.
- Surgery is mainly for significant cosmetic deformity or functional limitation, usually in younger children before stiffness and deformity are fixed.
- Woodward and modified Green procedures both aim to mobilise, lower and stabilise the scapula; clavicle osteotomy may be used when descent risks plexus stretch.
- “The safe first answer is: diagnose the elevated scapula, then look beyond the scapula for associated anomalies.
- “Mild deformity can be managed without surgery; severe visible deformity with motion loss is the usual reason to operate.
- “A high scapula plus short neck should make you look for Klippel-Feil syndrome before planning surgery.
- “Brachial plexus stretch is the feared intraoperative complication when the scapula is translated inferiorly.
Sprengel Deformity
Before planning scapular relocation, assess the cervical spine, ribs, scoliosis and syndromic associations. A technically successful shoulder operation is unsafe if cervical instability, rib deformity or systemic anomalies are missed.
- Low Concern
- Cavendish I or II
- Higher Concern
- Cavendish III or IV
- Practical Effect
- Higher grades are more likely to need surgery for cosmesis and motion.
- Low Concern
- Near-functional abduction
- Higher Concern
- Marked abduction loss or asymmetry
- Practical Effect
- Functional limitation strengthens the operative indication.
- Low Concern
- Young child with flexible soft tissues
- Higher Concern
- Older child, adolescent or adult
- Practical Effect
- Earlier correction usually gives better descent and easier mobilisation.
- Low Concern
- None or stable
- Higher Concern
- Klippel-Feil, scoliosis, rib, renal or cardiac anomalies
- Practical Effect
- Triggers imaging, anaesthetic planning and sometimes specialist input.
- Low Concern
- Absent or fibrous band only
- Higher Concern
- Rigid bony tether to cervical spine
- Practical Effect
- Must be defined before surgery and excised if limiting scapular descent.
SCAREAssessment | LOWEROperation Aim | TRAPSPitfalls |
|---|---|---|
S Scapula High, small, rotated and often prominent superomedially. | L Loosen tether Excise omovertebral bone or fibrous tether. | T Too much descent Can stretch the brachial plexus. |
C Cervical spine Look for Klippel-Feil, neck webbing and cervical motion limits. | O Open safe planes Protect spinal accessory, dorsal scapular and brachial plexus structures. | R Rigid ribs Rib cage abnormality may limit correction. |
A Abduction Measure active and passive shoulder abduction and scapular rotation. | W Woodward or Green Choose a relocation technique based on deformity and surgeon experience. | A Associated syndromes Missing Klippel-Feil or renal/cardiac anomalies is unsafe. |
R Ribs and renal Rib anomalies and renal anomalies can coexist. | E Ease plexus tension Use clavicle osteotomy or limited descent if nerve stretch risk is high. | P Persistent limitation Abduction may improve but may not become normal. |
E Expectation Clarify whether the family priority is cosmesis, motion or both. | R Reattach and rehab Secure muscle origins and restore shoulder motion gradually. | S Scar and shoulder contour Counsel about scar, asymmetry and possible correction loss. |
The shoulder finding should scare you into looking wider. | The operation lowers and releases the scapula. | Do not chase cosmesis blindly. |
Overview and Epidemiology
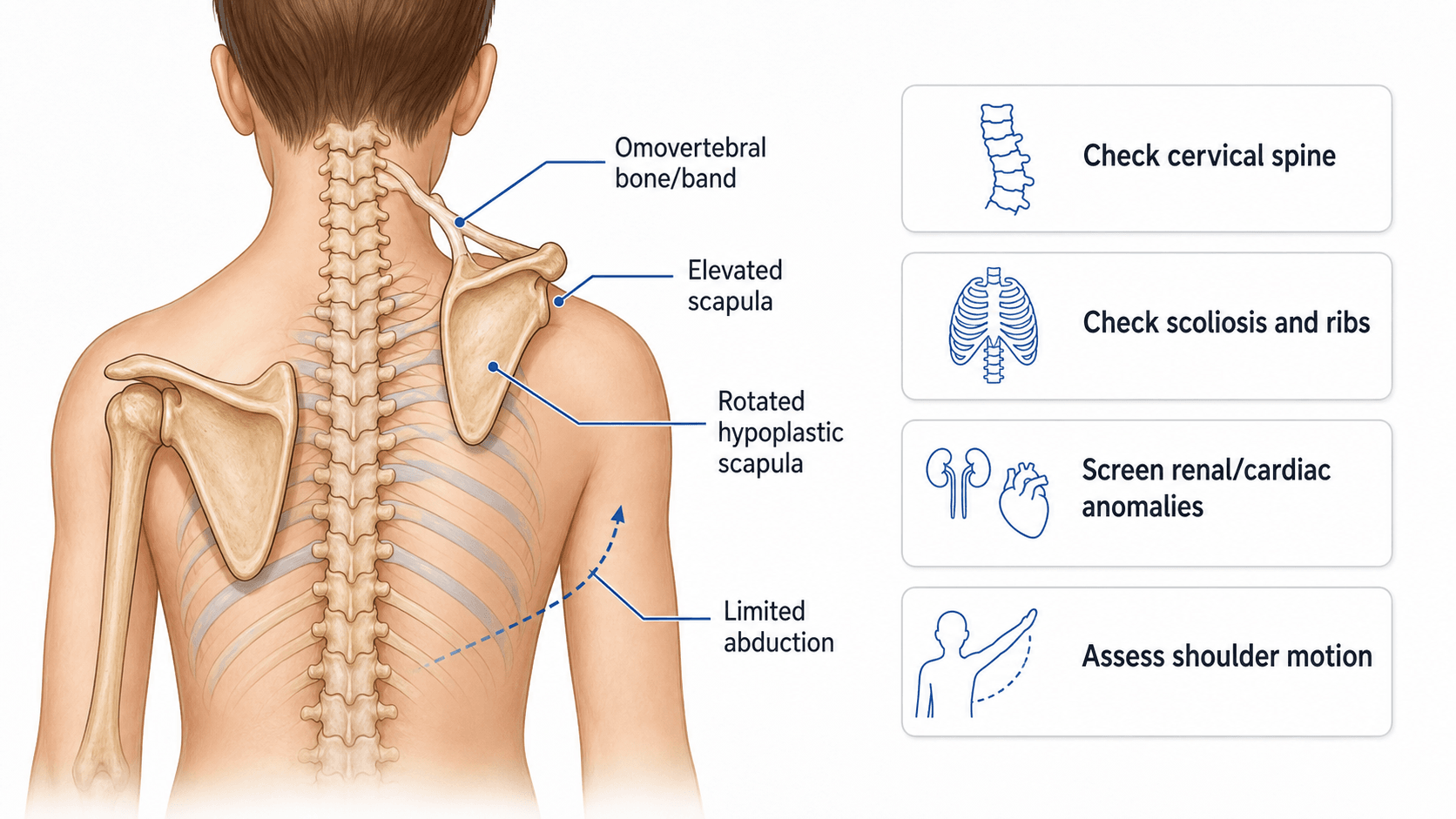
Sprengel deformity is congenital elevation of the scapula due to failure of normal scapular descent during embryological development. The affected scapula remains high in the neck, is often hypoplastic and malrotated, and may be connected to the cervical spine by an omovertebral bone, cartilage or fibrous band.
It is rare, but it is the most common congenital anomaly of the shoulder girdle. The child usually presents because one shoulder looks high, the neck appears webbed or asymmetric, or shoulder abduction is restricted. Pain is not usually the main complaint in childhood; appearance and motion are the key issues.
The condition matters because it is often not isolated. It may coexist with Klippel-Feil syndrome, scoliosis, rib anomalies, congenital renal anomalies, cardiac anomalies and other syndromic findings. The assessment therefore starts at the scapula but must not stop there.
Congenital undescended scapula with scapular elevation, hypoplasia, malrotation and variable omovertebral tethering.
Limited scapulothoracic rotation reduces shoulder abduction and creates cosmetic asymmetry.
The great majority of Sprengel deformity is sporadic, so the recurrence risk for future siblings or offspring is generally low. A rare autosomal-dominant familial form has been reported, so a positive family history or a clear syndromic context should prompt clinical genetics review. The practical counselling line is: usually a one-off developmental event with low recurrence risk, but check the family history and broader syndromic features (especially Klippel-Feil) before quoting a risk.
Pathophysiology and Anatomy
The scapula forms in the cervical region and normally descends caudally during early development. Sprengel deformity reflects incomplete descent. The scapula is not simply sitting high; it is often structurally abnormal.
The scapula begins development opposite the lower cervical spine (around C4-C6) at about the 5th week of gestation and normally descends to its final position over the upper thorax (about T2-T7) by roughly the 12th week. Sprengel deformity is an arrest of this caudal descent, so the scapula remains abnormally high - and because it never left the cervical region, the omovertebral connection runs to the cervical spine. This developmental arrest also explains the frequent coexistence of cervical (Klippel-Feil) and upper-rib anomalies, which form over the same window.
Key anatomical features:
- High scapula: the superior angle sits abnormally high in the neck.
- Hypoplastic scapula: the affected scapula is often smaller than the opposite side.
- Malrotation: the glenoid and body are rotated, impairing scapulothoracic movement.
- Omovertebral connection: a bone, cartilage or fibrous band may connect the superomedial scapula to cervical vertebrae.
- Muscle abnormalities: trapezius, rhomboids, levator scapulae and periscapular muscles may be hypoplastic, contracted or abnormally inserted.
- Rib cage limitation: rib and thoracic deformity may restrict how far the scapula can be lowered safely.
The limitation of abduction is mechanical. The glenohumeral joint may be structurally normal, but the scapula cannot rotate upward normally on the thorax. This is why shoulder abduction improves only if the scapula is mobilised and positioned more favourably.
Classification
Classification is used to describe severity and guide discussion. It does not replace the clinical decision: treatment still depends on function, appearance, age, associated anomalies and family priorities.
- Clinical Appearance
- Very mild; shoulders nearly level when clothed
- Practical Meaning
- Usually observation.
- Clinical Appearance
- Mild; visible lump or shoulder asymmetry after inspection
- Practical Meaning
- Usually non-operative unless function or cosmesis is important.
- Clinical Appearance
- Moderate; shoulder elevated with obvious deformity
- Practical Meaning
- Often considered for surgery if age and workup are favourable.
- Clinical Appearance
- Severe; high scapula with neck webbing or marked asymmetry
- Practical Meaning
- Strongest cosmetic indication, but also highest nerve and correction-risk planning burden.
Associated Anomalies
Associated anomalies decide how safe treatment is. A high scapula should trigger a structured screen rather than a narrow shoulder assessment.
- What to Look For
- Klippel-Feil syndrome, fused cervical vertebrae, short neck, low hairline, limited neck movement
- Why It Matters
- Affects airway, positioning, neurological risk and operative planning.
- What to Look For
- Scoliosis, rib fusion, rib absence, chest wall asymmetry
- Why It Matters
- May limit correction and alter respiratory or anaesthetic planning.
- What to Look For
- Renal agenesis, ectopia or other congenital renal anomaly
- Why It Matters
- Renal ultrasound is reasonable when syndromic features are present.
- What to Look For
- Congenital cardiac disease, murmur, syndromic features
- Why It Matters
- Cardiology or echocardiography may be needed before anaesthesia.
- What to Look For
- Cervical cord symptoms, brachial plexus symptoms, weakness or abnormal reflexes
- Why It Matters
- Changes urgency and imaging; do not ignore neurological signs.
- What to Look For
- Poland syndrome, VACTERL-like pattern, 22q11.2 features or multiple congenital anomalies
- Why It Matters
- Genetics and multidisciplinary review may be appropriate.
Neck pain, neurological symptoms, marked cervical stiffness, severe scoliosis, respiratory symptoms, cardiac murmur, renal history or multiple congenital anomalies should slow the plan down and broaden the workup.
Clinical Presentation
The usual presentation is a child with a visibly high shoulder or asymmetric shoulder contour. The deformity may be noticed at birth, during early childhood, or when the child begins activities requiring overhead motion.
History should define:
- age at recognition and whether the deformity is progressive in appearance;
- family concern: cosmesis, shoulder function, sport, clothing, teasing or pain;
- shoulder function: overhead reach, dressing, hair care, sport and fatigue;
- neck symptoms: stiffness, pain, limited rotation or neurological symptoms;
- birth history and other congenital anomalies;
- previous physiotherapy, bracing or investigations;
- family goals and tolerance for scar, recurrence risk and prolonged follow-up.
Examination should be deliberate:
- Inspect from behind with the trunk exposed. Compare shoulder height, scapular height, neck webbing, trapezial contour and scoliosis.
- Palpate the superior angle and medial border of the scapula. Look for a prominent superomedial corner.
- Measure active and passive shoulder forward elevation and abduction on both sides.
- Observe scapulothoracic rhythm. The scapula may fail to upwardly rotate as the arm elevates.
- Assess glenohumeral motion separately from scapulothoracic motion.
- Examine cervical range of motion and signs of Klippel-Feil syndrome.
- Screen neurological status in the upper limb, especially if there are cervical abnormalities.
- Examine the spine and chest wall for scoliosis and rib anomalies.
- Look for renal, cardiac or syndromic clues from the history and general examination.
If passive glenohumeral motion is good but active overhead motion is limited by scapular tethering, the problem is scapulothoracic mechanics rather than a frozen shoulder or isolated glenohumeral disorder.
Investigations and Imaging
Investigations should answer four questions:
- How severe is the scapular elevation and malrotation?
- Is there an omovertebral bone or other tether?
- Are the cervical spine, ribs and thorax abnormal?
- Are there renal, cardiac or syndromic features that change safety?
- What It Shows
- Scapular height, clavicles, ribs, thoracic symmetry
- When It Helps
- Baseline radiographic severity and rib assessment.
- What It Shows
- Fused vertebrae, alignment, Klippel-Feil pattern
- When It Helps
- Any short neck, low hairline, limited neck motion or planned surgery.
- What It Shows
- Scoliosis and global trunk alignment
- When It Helps
- Clinical scoliosis or asymmetry.
- What It Shows
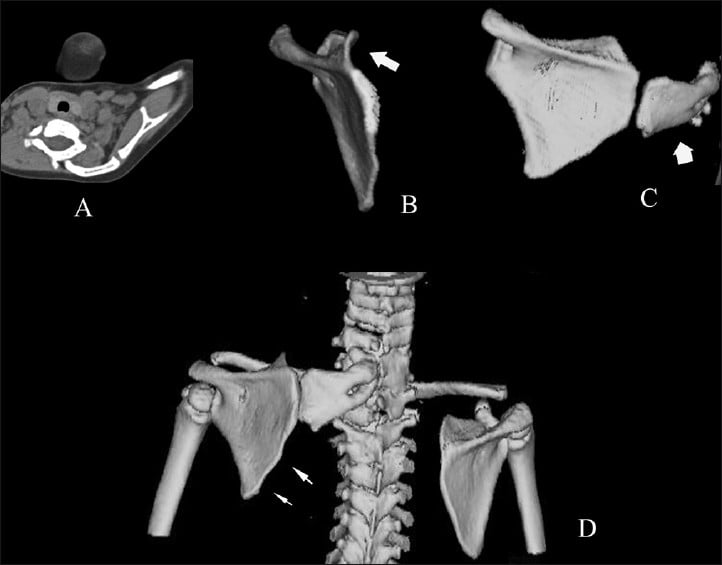
- Omovertebral bone, scapular morphology, rib cage anatomy
- When It Helps
- Preoperative planning, severe deformity or uncertain bony tether.
- What It Shows
- Cord, canal, intraspinal anomalies and soft-tissue tether
- When It Helps
- Neurological signs, complex cervical anomalies or uncertain soft-tissue connection.
- What It Shows
- Associated congenital renal/cardiac anomalies
- When It Helps
- Syndromic features, multiple anomalies or local protocol.
Do not order CT only to label the condition. CT is most valuable when it changes operative planning: omovertebral bone excision, scapular osteotomy planning, rib anatomy, and safe corridor planning.
Differential Diagnosis
A high or asymmetric shoulder is not always Sprengel deformity. The distinction matters because management differs and some mimics carry their own systemic risk.
- Distinguishing Features
- Congenital, high small malrotated scapula, prominent superomedial angle, restricted abduction, possible omovertebral bone
- Key Discriminator
- Fixed elevated scapula present from birth with scapulothoracic motion loss.
- Distinguishing Features
- Short neck, low hairline, limited neck rotation, fused cervical vertebrae
- Key Discriminator
- Cervical synostosis is the primary finding; may coexist with Sprengel.
- Distinguishing Features
- Mobile scapula, normal shape, asymmetry corrects with posture, full abduction
- Key Discriminator
- No fixed scapular elevation and normal scapular morphology.
- Distinguishing Features
- Rib and vertebral anomalies, curve on imaging, shoulder height follows the curve
- Key Discriminator
- Spinal deformity drives the asymmetry, not a tethered scapula.
- Distinguishing Features
- Medial or lateral winging that worsens on resisted protraction, normal scapular height at rest
- Key Discriminator
- Dynamic winging from nerve palsy, not a congenitally elevated scapula.
- Distinguishing Features
- Internal rotation contracture, glenohumeral dysplasia, posterior shoulder subluxation
- Key Discriminator
- History of birth palsy with glenohumeral, not scapulothoracic, pathology.
Management Decision-Making
Management is based on severity, function, age and safety. The aim is not to make every scapula look normal; the aim is to improve meaningful cosmesis and shoulder motion without creating neurological injury.
Non-operative care is appropriate when the deformity is mild, shoulder function is acceptable, the family concern is low, or surgery would carry excessive risk.
It includes:
- education that the condition is congenital and usually not painful;
- physiotherapy to maintain shoulder range, posture and periscapular strength;
- monitoring of shoulder motion and cosmetic concern during growth;
- assessment of associated anomalies when clinically indicated;
- practical reassurance that mild deformity can have good function without surgery.
Non-operative care does not make a high scapula descend. Its role is to maintain function, support adaptation and avoid unnecessary surgery in mild cases.
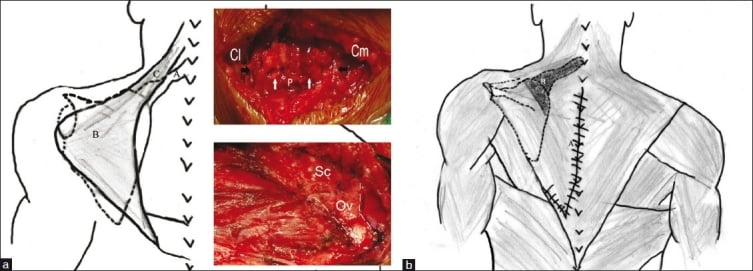
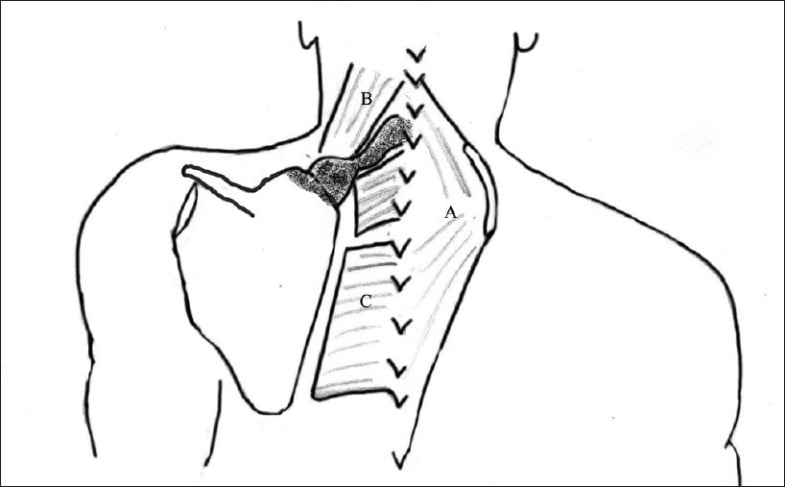
Operative Technique
The operative plan must be explicit before the incision: expected descent, omovertebral excision, soft-tissue release, need for clavicle osteotomy, nerve monitoring plan, and postoperative immobilisation.
Purpose: lower the scapula by releasing trapezius and rhomboid origins from the spinous processes, excising tethers, translating the scapula inferiorly and reattaching the muscle origins lower.
Stepwise technique:
- Position: prone or lateral/prone variant with the entire shoulder girdle, neck and thoracic spine accessible.
- Preparation: mark spinous processes, scapular borders, scapular spine, superior angle and planned midline/parascapular exposure.
- Exposure: posterior incision along the upper thoracic/cervical midline or planned approach; raise skin flaps carefully.
- Identify muscle origins: trapezius and rhomboids are elevated from the spinous processes as a sleeve.
- Release tether: identify and excise omovertebral bone or fibrous band if present.
- Scapular mobilisation: release tight levator scapulae, periscapular tethering and superomedial restriction as needed.
- Inferior translation: lower the scapula gradually. Avoid aggressive forced descent.
- Nerve protection: monitor brachial plexus clinically or with neuromonitoring; consider clavicle osteotomy if tension is concerning.
- Fixation and reattachment: reattach the muscle sleeve at a lower level to maintain correction.
- Closure: meticulous haemostasis, drain as needed, layered closure and immobilisation.
Complications
Complications can be early, structural or expectation-related.
- Mechanism
- Excessive inferior translation and traction
- Prevention or Response
- Limit descent, use neuromonitoring or wake-up test, consider clavicle osteotomy.
- Mechanism
- Soft-tissue tension, growth, inadequate fixation or rigid deformity
- Prevention or Response
- Secure repair, realistic correction target and follow-up.
- Mechanism
- Muscle release, hypoplastic muscles or poor reattachment
- Prevention or Response
- Careful muscle handling and rehabilitation.
- Mechanism
- Posterior exposure and soft-tissue tension
- Prevention or Response
- Meticulous closure, drain decisions and scar care.
- Mechanism
- Nonunion, malunion, hardware irritation or scar
- Prevention or Response
- Use only when needed; stabilise and follow union.
- Mechanism
- Glenohumeral or scapulothoracic mechanics remain abnormal
- Prevention or Response
- Preoperative counselling and realistic rehabilitation goals.
- Mechanism
- Narrow shoulder-only assessment
- Prevention or Response
- Structured cervical, spine, rib, renal and cardiac screening.
Practical Case Approach
When shown a child with a high scapula, structure the answer in this order:
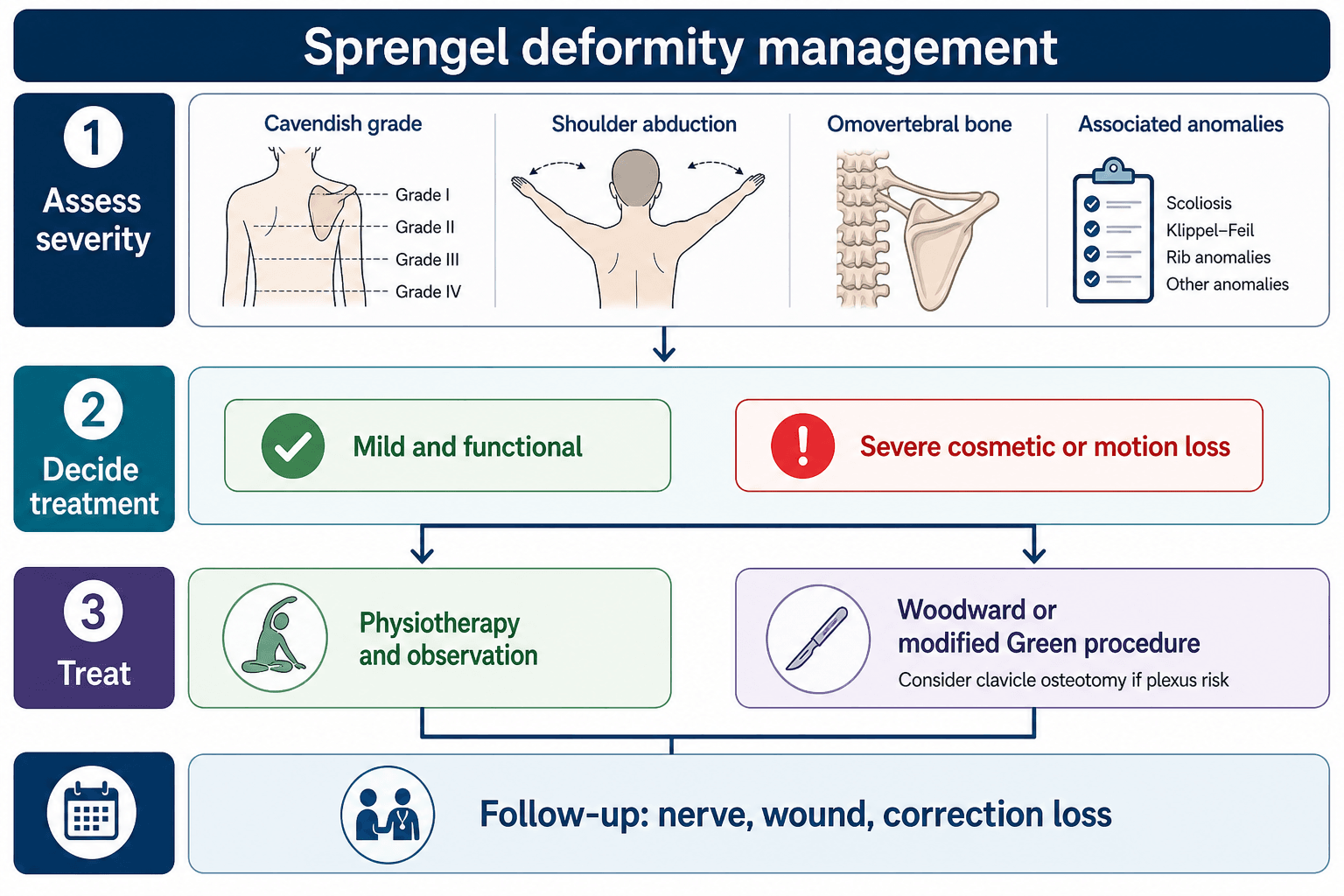
- Diagnosis: congenital elevated scapula consistent with Sprengel deformity.
- Severity: describe clinical appearance, Cavendish grade, shoulder abduction and functional limitation.
- Associated anomalies: specifically mention cervical spine, Klippel-Feil, scoliosis, ribs, renal and cardiac screening.
- Imaging: AP shoulder/chest, cervical spine films, spine imaging if needed, CT or 3D CT for omovertebral bone.
- Treatment choice: mild functional deformity can be observed; severe cosmetic or motion loss may need surgery.
- Operation: Woodward or modified Green procedure, omovertebral excision, safe inferior translation, possible clavicle osteotomy and nerve monitoring.
- Counselling: improvement rather than normality, scar, correction loss, nerve injury and persistent limitation.
Postoperative Care and Rehabilitation
Postoperative care protects the correction and then restores motion.
Typical care includes:
- observation of upper-limb neurological status after surgery;
- wound and drain monitoring;
- shoulder immobilisation according to surgeon preference and fixation stability;
- analgesia and scar care;
- early elbow, wrist and hand motion;
- gradual shoulder range after soft tissues have healed;
- physiotherapy for scapular control, posture and overhead function;
- serial review for correction loss, recurrence, winging and shoulder motion.
The family should know that improvement is expected, but the shoulder may not become perfectly level or perfectly mobile. Persistent asymmetry, scar and some abduction limitation may remain.
Guidelines, Registries and Global Practice
There is no high-level society guideline or implant registry specific to Sprengel deformity; it is a rare, non-arthroplasty congenital condition, so practice is guided by paediatric orthopaedic principles, narrative reviews and surgical series rather than registry data. The points below frame a globally consistent approach.
Global epidemiology
- Sprengel deformity is rare but is the most common congenital anomaly of the shoulder girdle; it is more often unilateral and is reported slightly more frequently in girls in several series.
- Klippel-Feil syndrome, congenital scoliosis and rib anomalies are the most consistently reported associations across populations; congenital renal and cardiac anomalies are described and justify screening when syndromic features are present.
Side-by-side principles across practice settings
- Emphasis
- Screen for associated anomalies; grade with Cavendish and Rigault
- Practical Position
- Observe mild deformity; reserve surgery for significant cosmetic or functional deformity in young children.
- Emphasis
- Cosmesis and function as operative indications
- Practical Position
- Resection of the protruding scapula plus inferior translation; long-term gains maintained.
- Emphasis
- Modified Green or Woodward with patient-reported outcomes
- Practical Position
- Selective clavicle osteotomy and structured follow-up with shoulder PROs.
- Emphasis
- Protect neurovascular structures during correction
- Practical Position
- Controlled descent, define the omovertebral bone, accept partial correction to avoid plexus injury.
Registry note
- Arthroplasty registries (NJR, AJRR, AOANJRR, SHAR, NZJR) do not capture Sprengel deformity because no implant is used. Outcome evidence comes from single-centre and multicentre surgical cohorts, which is why reporting is heterogeneous and major-complication rates, although low, are imprecise.
High- versus limited-resource practice variation
- In well-resourced settings, 3D CT for omovertebral and scapular morphology and intraoperative neuromonitoring or clavicle osteotomy are increasingly used to allow safer, larger correction.
- In limited-resource settings, plain radiographs and clinical grading drive decisions, neuromonitoring may be unavailable, and surgeons may favour conservative correction targets and selective clavicle osteotomy to protect the plexus without advanced monitoring. The core safety principle — screen widely and do not over-correct — is universal.
Controversies and Areas of Uncertainty
Much of the Sprengel evidence base is observational, so several practical questions remain genuinely unsettled. Examiners reward a candidate who can name the uncertainty rather than overstate the data.
- Optimal age to operate. Most series favour correction in younger children (often under 8 years) for better descent and remodelling, but the evidence is observational and confounded by deformity severity. There is no randomised threshold age.
- Woodward versus modified Green. Both relocate the scapula and report broadly similar improvements; comparative data are weak, and procedure choice largely reflects surgeon training rather than proven superiority.
- Routine clavicle osteotomy. Some surgeons add it selectively only when descent threatens the plexus, while others use it routinely with neuromonitoring to allow larger, safer correction. The trade-off of added clavicle morbidity against safer descent is not resolved.
- Role and necessity of neuromonitoring. Reported intraoperative alerts are uncommon, so whether neuromonitoring should be universal or reserved for major planned descent remains debated.
- Vertical scapular osteotomy and bony resections. These address rotational and superomedial prominence but add muscle and contour morbidity; their place outside specialised practice is uncertain.
- How far to correct. Aggressive cosmetic descent risks brachial plexus injury and contour problems. The consensus principle is that a safe partial correction is preferable to a neurologically unsafe complete one.
Clinical Reasoning Scenarios
Practise clinical reasoning and management decisions out loud
“A 5-year-old child is referred with one high shoulder, restricted overhead reach and a short neck. How do you assess the child?”
“The child has Cavendish grade IV deformity, shoulder abduction to 80 degrees and CT shows an omovertebral bone. What treatment would you recommend?”
“During scapular descent in a Woodward procedure, neuromonitoring signals fall. What do you do?”
“A 7-year-old has a mild visible high scapula, full functional use and no family concern. What is your management?”
Definition
- Congenital undescended scapula.
- High, hypoplastic, malrotated scapula.
- May have omovertebral bone or fibrous tether.
Must Screen
- Klippel-Feil and cervical spine.
- Scoliosis and rib anomalies.
- Renal/cardiac anomalies when syndromic features exist.
Classification
- Cavendish = clinical appearance.
- Rigault = radiographic scapular height.
- Omovertebral bone changes operative planning.
Treatment
- Mild and functional: observation and physiotherapy.
- Severe cosmetic or motion loss: Woodward or modified Green.
- Protect brachial plexus; consider neuromonitoring and clavicle osteotomy.
Complications
- Brachial plexus stretch injury.
- Correction loss or recurrence.
- Scapular winging, scar and persistent motion limitation.
Evidence Base
Pathogenesis and management review
- Sprengel deformity is rare but is the most common congenital anomaly of the shoulder, caused by abnormal scapular descent during embryonic development.
- It is commonly linked with Klippel-Feil syndrome, scoliosis and rib anomalies; diagnostic confusion with scoliosis can delay treatment of other abnormalities.
- Non-surgical management suits mild cases; surgery for severe cases centres on resection of the protruding scapula and inferior scapular translation, with long-term studies showing maintained gains.
Surgical treatment systematic review and meta-analysis
- The review included 41 articles, 674 patients and 711 shoulders.
- Green and Woodward procedures, both aiming to relocate the scapula to a more anatomical position, were the most commonly used techniques.
- 168 adverse events were recorded, including 18 major complications, an overall low major-complication rate.
- The best clinical and cosmetic results were achieved when surgery was performed in children younger than 8 years.
Modified Woodward approach case series and literature review
- Two boys (aged 7 and 10 years) with limited shoulder range of motion were treated with the modified Woodward approach.
- Physiotherapy from a young age was emphasised for mild disease; severe cases required operative correction with omovertebral band resection.
- Klippel-Feil association was highlighted as clinically important, reinforcing wider screening.
Woodward procedure with neuromonitoring
- Eighteen patients (mean age 4.4 years) underwent Woodward surgery with intraoperative neuromonitoring.
- Mean shoulder abduction improved from 84.4 to 151.1 degrees at 1 year.
- Mean Cavendish score improved from 3.6 to 1.1.
- One patient had a fall in motor-evoked potential signals during scapular reduction; correction was limited to the level where signals recovered, and no permanent plexus injury occurred.
3D CT morphology of omovertebral bone and scapula
- Twelve children with an omovertebral bone underwent preoperative 3D CT with reconstruction.
- The omovertebral bone most frequently connected to the cervical spine at C6 and was predominantly irregular in shape; scapular attachment was usually infraspinous along the vertebral border.
- All affected scapulae showed rotational deformity and a significantly reduced height-to-width ratio compared with the normal side.
Woodward with clavicle osteotomy and neuromonitoring
- Thirty-six patients (mean age 4.1 years) underwent the Woodward procedure with clavicle osteotomy and intraoperative neuromonitoring, mean follow-up 5.6 years.
- Shoulder abduction improved by an average of 74 degrees and Cavendish grade improved from grade 3 to 4 down to grade 1 to 2.
- No intraoperative neuromonitoring alerts and no brachial plexus injuries occurred; complications were limited to one delayed wound healing and one hypertrophic scar.
Patient-reported outcomes after modified Green procedure
- Forty-two shoulders in 40 children were treated with the modified Green procedure, mean follow-up 5 years.
- Adjunctive clavicular osteotomy in 15 patients improved postoperative abduction by a mean of 25 degrees.
- At follow-up, 67.5 percent had a QuickDASH score under 7 and 70 percent reported high satisfaction; the complication rate was 7.1 percent.