Cardiac Conditions & Pre-Participation Screening
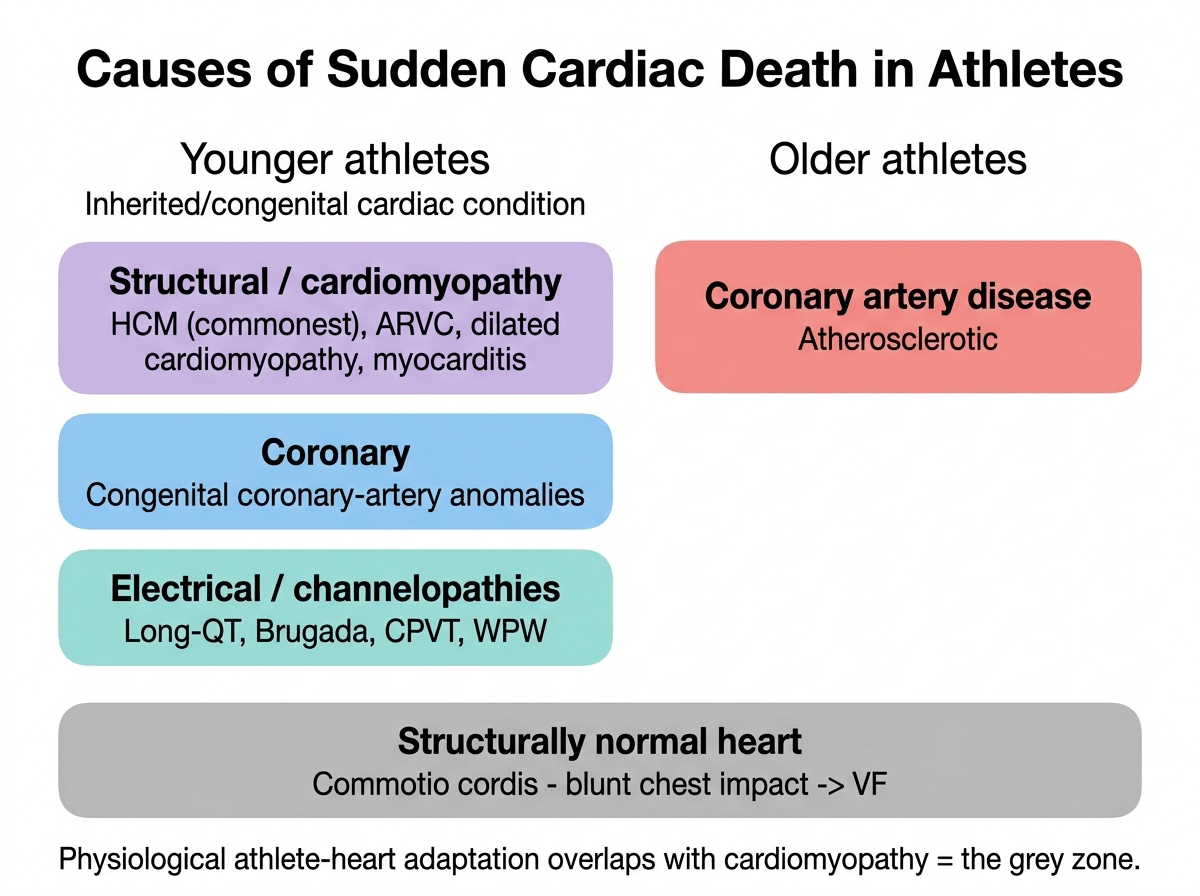
- SUDDEN CARDIAC DEATH (SCD) is the leading MEDICAL cause of death in sport, and in YOUNG athletes it is usually due to an underlying STRUCTURAL or ELECTRICAL CARDIAC CONDITION - most importantly HYPERTROPHIC CARDIOMYOPATHY (HCM), ARRHYTHMOGENIC (right-ventricular) CARDIOMYOPATHY (ARVC), dilated cardiomyopathy, congenital CORONARY ARTERY ANOMALIES, CHANNELOPATHIES (long-QT syndrome, Brugada, catecholaminergic polymorphic VT), myocarditis, and COMMOTIO CORDIS (ventricular fibrillation from blunt chest impact at a vulnerable point in the cardiac cycle).
- In OLDER ('master') athletes, atherosclerotic CORONARY ARTERY DISEASE is the leading cause of exercise-related SCD - so the differential is age-dependent.
- A central diagnostic challenge is the 'GREY ZONE' between PHYSIOLOGICAL cardiac ADAPTATION to intense exercise ('athlete's heart') and CARDIAC DISEASE that can cause SCD: features influenced by age, sex and ethnicity overlap, and careful interpretation of clinical findings with a broad diagnostic armamentarium (and sometimes ONGOING SURVEILLANCE, especially in the young) is needed to differentiate them.
- PRE-PARTICIPATION SCREENING aims to detect at-risk athletes BEFORE competition: it includes a focused personal/family HISTORY (syncope/near-syncope with exertion, family history of SCD/cardiomyopathy/channelopathy) and EXAMINATION, with the addition of a 12-lead ECG in some protocols (e.g. European/Italian models) - the value and optimal form of screening (history/exam alone vs ECG-inclusive) are DEBATED, balancing detection against false positives/cost.
- The 'grey zone' means screening and evaluation must avoid TWO errors: MISSING a disease that could cause SCD, and FALSELY DISQUALIFYING a healthy athlete with a physiological adaptation - so equivocal findings often require expert cardiology evaluation and surveillance rather than immediate disqualification.
- GIVE THE DENOMINATOR, because it is what the screening argument is actually about: sudden cardiac arrest occurs in roughly 1 in 50,000 ATHLETE-YEARS overall, rising to about 1 in 35,000 person-years in YOUNG MALE athletes and about 1 in 18,000 in BLACK MALE athletes. At that event rate even a specific test produces far more false positives than true ones, so the debate turns on cost and on the harm of wrongly restricting a healthy athlete rather than on whether the conditions are dangerous. ETHNICITY cuts both ways here - black male athletes carry the highest reported risk while also being the group in whom anterior T-wave inversion with preceding J-point elevation is a NORMAL variant.
- THE SURVIVAL BENEFIT OF THE EMERGENCY RESPONSE IS MEASURABLE AND STEPWISE. Pooling 28 non-randomised studies of sports-related arrest, the odds of survival were 2.55 (95% CI 1.48-4.37) with a BYSTANDER PRESENT, 3.84 (2.36-6.25) with BYSTANDER CPR and 5.25 (3.58-7.70) with BYSTANDER AED USE, at GRADE moderate certainty. On-site AED use also outperformed defibrillation by arriving emergency services - but many venues omit AEDs from the medical plan entirely, or leave them unsignposted or obstructed, which is the practical failure mode to look for.
- Regardless of screening, the EMERGENCY ACTION PLAN is critical to SURVIVING an on-field cardiac arrest: prompt recognition, immediate CPR, and EARLY DEFIBRILLATION with an on-site AUTOMATED EXTERNAL DEFIBRILLATOR (AED) are the key determinants of survival - so venues and teams must have a rehearsed emergency plan and accessible AEDs.
- “SCD = leading medical cause of death in sport. Young athletes: HCM, ARVC, dilated cardiomyopathy, congenital CORONARY ANOMALIES, CHANNELOPATHIES (long-QT/Brugada/CPVT), myocarditis, COMMOTIO CORDIS. Older athletes: coronary artery disease.
- “'Athlete's heart' (physiological adaptation) overlaps with cardiomyopathy = the diagnostic GREY ZONE - careful interpretation +/- surveillance; avoid missing disease AND avoid falsely disqualifying a healthy athlete.
- “Pre-participation screening = history + examination +/- ECG (DEBATED; ECG-inclusive in some protocols). Survival of an arrest depends on the EMERGENCY ACTION PLAN: early CPR + on-site AED (early defibrillation).
- “Rates: ~1:50,000 athlete-years overall; ~1:35,000 young male; ~1:18,000 black male athletes - the low event rate is why screening is contested.
- “Survival gradient (28 studies): witnessed OR 2.55, bystander CPR OR 3.84, bystander AED OR 5.25. On-site AED beats waiting for EMS.
- “Practical failure mode: AEDs absent from the medical plan, unsignposted or obstructed.
Young: HCM, ARVC, dilated cardiomyopathy, coronary anomalies, channelopathies (long-QT/Brugada/ CPVT), myocarditis, commotio cordis. Older: coronary artery disease.
'Athlete's heart' vs disease - careful interpretation +/- surveillance (don't miss disease or falsely disqualify). Emergency action plan + AED (early defibrillation) saves lives.
Causes, the Grey Zone, Screening & Response
SCD is the leading medical cause of death in sport. In young athletes it reflects an underlying cardiac condition - HCM, ARVC, dilated cardiomyopathy, congenital coronary anomalies, channelopathies (long-QT, Brugada, CPVT), myocarditis, and commotio cordis; in older athletes, coronary artery disease. Intense exercise produces physiological 'athlete's heart' that overlaps with cardiomyopathy - the grey zone - requiring careful interpretation and sometimes surveillance to avoid both missing disease and falsely disqualifying a healthy athlete. Pre-participation screening uses history + examination, with ECG added in some (debated) protocols. Crucially, surviving an on-field arrest depends on the emergency action plan: prompt recognition, immediate CPR and early defibrillation with an on-site AED.
- Athlete's heart (physiological)
- Mild, symmetrical; regresses with detraining
- Disease (e.g. cardiomyopathy)
- Marked/asymmetrical (HCM); does not regress
- Athlete's heart (physiological)
- Balanced dilatation, normal function
- Disease (e.g. cardiomyopathy)
- Disproportionate; abnormal function/strain
- Athlete's heart (physiological)
- Common training-related changes
- Disease (e.g. cardiomyopathy)
- Pathological patterns (e.g. deep T-wave inversion)
- Athlete's heart (physiological)
- Absent
- Disease (e.g. cardiomyopathy)
- Exertional syncope; family history of SCD
- Athlete's heart (physiological)
- Reassure (+/- surveillance)
- Disease (e.g. cardiomyopathy)
- Expert evaluation; risk stratify; restrict as indicated
Screening & Emergency Response
- Pre-participation screening: personal/family history (exertional syncope/near-syncope, family history of SCD/cardiomyopathy/channelopathy) + examination; ECG added in some protocols (debated - detection vs false positives/cost). Equivocal/'grey zone' findings -> expert cardiology evaluation +/- surveillance.
- Avoid both errors: don't MISS disease; don't FALSELY DISQUALIFY a healthy athlete (physiological adaptation).
- Emergency action plan (critical): rehearsed plan, prompt recognition of arrest, immediate CPR, and early defibrillation with an accessible on-site AED - the key determinants of survival.
- Commotio cordis: consider chest protection in at-risk sports; immediate defibrillation is life-saving.
Two principles dominate the care of athletes at risk of sudden cardiac death. First, distinguishing the physiological 'athlete's heart' from disease is genuinely difficult: intense training produces cardiac adaptations
- influenced by age, sex and ethnicity - that overlap with cardiomyopathies that cause SCD, so evaluation must avoid both errors. Missing a hypertrophic or arrhythmogenic cardiomyopathy, a coronary anomaly or a channelopathy can be fatal, while over-calling a normal adaptation as disease can wrongly end an athlete's career; equivocal 'grey zone' findings therefore warrant expert cardiology assessment, a broad diagnostic work-up and, especially in the young, ongoing surveillance rather than a snap judgement. Second, whatever the screening strategy - and the value and form of pre-participation screening (history/examination alone versus ECG-inclusive) remain debated - no screening eliminates risk, so the decisive factor in surviving an on-field cardiac arrest is the emergency response: a rehearsed emergency action plan, prompt recognition, immediate CPR and, above all, early defibrillation with an accessible automated external defibrillator. Venues, teams and events must therefore have AEDs and trained responders, because early defibrillation is what turns an arrest into a survivor.
Interpreting the Athlete's ECG (the International Criteria)
Separating a training-related ECG change from a pathological one is the practical skill the grey zone demands. Modern athlete ECG interpretation (the International / Seattle-derived criteria) sorts findings into normal, borderline and abnormal, which sharply cuts false positives compared with older standards. The key principle: electrical changes that simply reflect high vagal tone and chamber enlargement are normal; changes that suggest a cardiomyopathy or channelopathy are abnormal and trigger work-up.
- Findings
- Sinus bradycardia/arrhythmia, ectopic atrial/junctional rhythm, first-degree AV block, Mobitz I (Wenckebach), incomplete RBBB, isolated QRS-voltage criteria for LVH, early repolarisation/ST elevation; in black athletes, J-point elevation with convex ST elevation and T-wave inversion in V1-V4
- Action
- No further work-up if asymptomatic and no family history
- Findings
- Left or right axis deviation, left atrial enlargement, right ventricular hypertrophy voltages
- Action
- One alone is benign; TWO OR MORE borderline findings = evaluate
- Findings
- T-wave inversion beyond V1-V3 (esp. lateral/inferolateral), ST depression, pathological Q waves, complete LBBB, epsilon wave, prolonged or short QT, Brugada type-1 pattern, profound bradycardia/AV block, frequent PVCs or atrial/ventricular arrhythmias
- Action
- Refer for expert cardiac evaluation
Normal-in-athletes = the vagal / chamber-enlargement group (sinus brady, first-degree block, Wenckebach, incomplete RBBB, isolated LVH voltage, early repolarisation). Abnormal = anything pointing at structural or electrical disease (lateral/inferolateral T-wave inversion, ST depression, pathological Q waves, epsilon wave, long/short QT, Brugada type-1). Ethnicity matters: anterior T-wave inversion in V1-V4 with preceding J-point elevation is a normal variant in black athletes but warrants work-up otherwise.
How Often, In Whom, and What Actually Changes Survival
The Rate - and Why It Governs the Screening Argument
A review of sudden cardiac arrest in stadium sport puts the risk across athletes in all sports at about 1 in 50,000 athlete-years, and the risk is not evenly spread:
- Reported risk
- About 1 in 50,000 athlete-years
- Reported risk
- About 1 in 35,000 person-years
- Reported risk
- About 1 in 18,000 person-years
That order of magnitude is the reason the screening debate exists at all rather than being an oversight. When the event being sought occurs in roughly one athlete in fifty thousand per year, even a specific test generates far more false positives than true ones, and the argument turns on cost, on the consequences of wrongly restricting a healthy athlete, and on the size of any mortality benefit - not on whether the conditions are serious. Quoting a screening position without the denominator misses what is actually being argued about.
The demographic gradient also joins up with the ECG section: ethnicity affects both the baseline risk and the interpretation of the trace. Black male athletes carry the highest reported risk while also being the group in whom anterior T-wave inversion preceded by J-point elevation is a normal variant - so ethnicity must be handled carefully in both directions rather than being treated as a single adjustment.
What Changes Survival, in Order
The claim that the emergency response matters more than the screening can be quantified. A systematic review and meta-analysis of 28 non-randomised studies of sports-related sudden cardiac arrest found a stepwise association with survival:
- Odds ratio for survival (95% CI)
- 2.55 (1.48 to 4.37)
- Studies / patients
- 9 studies, 988 patients
- Odds ratio for survival (95% CI)
- 3.84 (2.36 to 6.25)
- Studies / patients
- 23 studies, 2,523 patients
- Odds ratio for survival (95% CI)
- 5.25 (3.58 to 7.70)
- Studies / patients
- 19 studies, 1,227 patients
The gradient is the teaching point: simply being witnessed roughly doubles the odds of survival, CPR nearly quadruples them, and bystander defibrillation carries the largest association of the three. GRADE certainty was rated moderate, and every study was non-randomised - which is unavoidable here and means these are associations rather than proven causal effects, though the direction and consistency are persuasive.
The practical corollary from the stadium review is unglamorous and worth stating: on-site AED use improved survival more than defibrillation delivered by arriving emergency services, yet many venues had no AED written into their medical plan, and the devices were frequently unsignposted or physically obstructed. An AED that nobody can find in ninety seconds is not an AED.
Give the denominator: roughly 1 in 50,000 athlete-years overall, 1 in 35,000 in young men and 1 in 18,000 in black male athletes - which is precisely why screening is argued about. Then give the survival gradient: bystander presence OR 2.55, bystander CPR OR 3.84, bystander AED use OR 5.25 across 28 studies, GRADE moderate. And note the practical failure mode - AEDs that are absent from the medical plan, unsignposted or obstructed.
Mnemonics & Memory Aids
ARREST
Hook:ARREST: AED/Action plan, aRrhythmogenic+hypertrophic CM, coRonary causes, Electrical channelopathies/commotio, Screening, aThlete's-heart grey zone.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What causes sudden cardiac death in athletes, what is the 'grey zone', and what most determines survival of an on-field arrest?”
Causes
- Young: HCM, ARVC, dilated cardiomyopathy, congenital coronary anomalies
- Young: channelopathies (long-QT, Brugada, CPVT), myocarditis, commotio cordis
- Older (masters): atherosclerotic coronary artery disease
The grey zone
- 'Athlete's heart' (physiological adaptation) overlaps with cardiomyopathy
- Influenced by age, sex, ethnicity; careful interpretation +/- surveillance
- Avoid missing disease AND falsely disqualifying a healthy athlete
Screening
- History (exertional syncope; family history of SCD/cardiomyopathy/channelopathy) + examination
- ECG added in some protocols (debated - detection vs false positives/cost)
- Equivocal findings -> expert cardiology evaluation +/- surveillance
Surviving an arrest
- Emergency action plan (rehearsed); prompt recognition
- Immediate CPR; early defibrillation with on-site AED (the key to survival)
- Survival odds (28 studies): witnessed 2.55, bystander CPR 3.84, bystander AED 5.25
- On-site AED beats defibrillation by arriving EMS
- Check the AED is IN the medical plan, signposted and unobstructed
- Commotio cordis: chest protection in at-risk sports; immediate defibrillation
How common
- ~1 in 50,000 athlete-years across all sports
- ~1 in 35,000 person-years in young male athletes
- ~1 in 18,000 in black male athletes
- The low event rate is what makes screening contested (false positives dominate)
- Ethnicity shifts BOTH baseline risk AND normal ECG variants
Evidence & Key Studies
The grey zone between physiological adaptation and cardiac disease in athletes
- Athletes exhibit physiological cardiac changes that can overlap with cardiac diseases that may cause sudden cardiac death; age, sex and ethnicity influence the cardiac adaptation to exercise.
- The differential between 'athlete's heart' and heart disease can be challenging, but careful interpretation of clinical findings and a broad diagnostic armamentarium usually allow an appropriate differential diagnosis.
- Equivocal 'grey zone' cases require ongoing surveillance, especially in very young individuals, where a cardiac disease may only fully manifest at an older age.
Association between basic life support and survival in sports-related sudden cardiac arrest: a meta-analysis
- Systematic review and meta-analysis of 28 non-randomised studies of sports-related sudden cardiac arrest, examining bystander presence, bystander CPR and bystander AED use against survival.
- All three were significantly associated with survival: bystander presence OR 2.55 (95% CI 1.48-4.37), bystander CPR OR 3.84 (2.36-6.25) and bystander AED use OR 5.25 (3.58-7.70), with low to moderate heterogeneity.
- GRADE certainty was judged moderate; the authors conclude that first-aid training policy and AED installation in sport settings should be developed.
Sudden cardiac arrest in basketball and soccer stadiums and the role of automated external defibrillators (BELTRAN study review)
- Athletes across all sports face a sudden cardiac arrest risk of about 1 in 50,000 athlete-years, rising to about 1 in 35,000 person-years in young male athletes and about 1 in 18,000 in black male athletes.
- On-site AED use improves survival more than defibrillation delivered by arriving emergency services, and soccer outcomes are poorest in Africa and South America at 3% and 4% survival.
- Many stadiums have not incorporated AEDs into their medical plans, and the devices are often unrecognisable or obstructed - so signposting, trained personnel and inclusion in the medical plan matter as much as ownership.
The overlap between physiological cardiac adaptation and cardiac disease, the influence of age, sex and ethnicity, and the need for careful interpretation and ongoing surveillance come from the cited Sivalokanathan review. The survival odds ratios for bystander presence, CPR and AED use are the cited Michelland meta-analysis of 28 studies - all non-randomised, so these are associations rather than demonstrated causal effects, with GRADE certainty rated moderate. The incidence figures and the observations about AED signposting and medical plans come from the cited Bassi review, which is a narrative review rather than a pooled analysis, so its rates should be read as reported ranges rather than precise pooled estimates.
The argument that the low event rate is what drives the screening debate is an inference drawn from putting those incidence figures beside the debate rather than a conclusion any of the cited papers states. No verified figure was identified for the mortality benefit of ECG-inclusive versus history-and-examination screening, so none is quoted and the debate is left described rather than settled.
The specific causes of SCD in young versus older athletes, the International athlete ECG criteria, and the shift from blanket disqualification to shared decision-making are standard, well-established teaching. No dedicated topic on hypertrophic cardiomyopathy, commotio cordis or pre-participation evaluation exists in the library, so those are covered here rather than deferred. (See also Return to Sport Criteria.)