Shoulder Pain | Infraspinatus Wasting | Notch-Specific Compression
- Suprascapular nerve arises from upper trunk (C5-C6), travels through suprascapular notch under transverse scapular ligament
- Spinoglenoid notch entrapment spares supraspinatus, isolates infraspinatus atrophy and weakness
- Paralabral ganglion cysts from superior labral tears are the leading compressive etiology at spinoglenoid notch
- Infraspinatus wasting is the hallmark clinical sign; external rotation weakness at 0 and 90 degrees
- EMG shows denervation; MRI identifies ganglion and labral tear; decompression indicated for progressive deficit or failed conservative care
- “Suprascapular notch lesion = supraspinatus + infraspinatus wasting
- “Spinoglenoid notch lesion = infraspinatus only wasting (supraspinatus spared)
- “Always image the labrum when isolated infraspinatus atrophy present
- “Positive lag sign and hornblower sign indicate advanced infraspinatus dysfunction
Suprascapular notch lies at superior border of scapula; nerve passes beneath transverse scapular ligament. Compression here denervates both supra- and infraspinatus.
Spinoglenoid notch is more distal at base of scapular spine; compression spares supraspinatus. Classic infraspinatus fossa wasting with preserved supraspinatus.
Paralabral ganglion from posterosuperior labral tear is the most common mass lesion. Cyst compresses nerve at spinoglenoid notch; always evaluate labrum on MRI.
EMG confirms diagnosis. Fibrillations and positive sharp waves appear 3-4 weeks after onset. Normal EMG early does not exclude entrapment; repeat if high suspicion.
- Diagnosis
- Suprascapular notch compression, no ganglion
- Treatment
- Transverse scapular ligament release +/- notchplasty
- Key Pearl
- Address ligament first; check for space-occupying lesion
- Diagnosis
- Spinoglenoid notch + paralabral ganglion on MRI
- Treatment
- Arthroscopic labral repair + cyst decompression
- Key Pearl
- Treat the labral tear to prevent recurrence
- Diagnosis
- Confirmed entrapment on EMG/MRI
- Treatment
- Surgical decompression at affected notch
- Key Pearl
- Delay increases irreversible atrophy risk
SISINotch Differentiation
Hook:SISI: Suprascapular notch hits both; Spinoglenoid hits Infraspinatus alone!
LABRALGanglion Cyst Mechanism
Hook:LABRAL explains why cyst decompression must include labral repair!
EMGMRIEMG and Imaging Sequence
Hook:EMGMRI sequence prevents missing treatable compressive pathology!
Overview and Epidemiology
Suprascapular nerve entrapment is an under-recognised cause of shoulder pain and weakness. It is frequently misdiagnosed as rotator cuff pathology or cervical radiculopathy. Early recognition prevents irreversible muscle atrophy. The two anatomic sites produce distinct clinical pictures, and paralabral ganglion cysts represent the most common compressive lesion at the spinoglenoid notch. Surgical decompression yields good outcomes when performed before advanced fatty infiltration.
- Repetitive traction: Overhead athletes, weightlifters, swimmers
- Ganglion cyst: Paralabral cyst from superior labral tear
- Transverse scapular ligament: Thickened or ossified ligament at suprascapular notch
- Space-occupying lesions: Tumours, varices, or fracture callus
- Iatrogenic: After distal clavicle excision or shoulder surgery
- Pain: Deep, aching posterior shoulder pain, worse at night
- Weakness: Loss of external rotation power and overhead function
- Atrophy: Visible infraspinatus fossa wasting (chronic cases)
- Secondary impingement: Loss of infraspinatus leads to altered scapular mechanics
- Quality of life: Significant disability in athletes and manual workers

Suprascapular neuropathy in a shoulder referral practice
- Of 92 patients undergoing electrodiagnostic testing for suspected SSN, 40 (43%) were confirmed; SSN was diagnosed in 4.3% of all new patients
- Patients with a massive rotator cuff tear were significantly more likely to have an abnormal study (p=0.006)
- Abnormal motor unit action potentials were the commonest finding (88%); frank denervation was seen in only 33%
Arthroscopic suprascapular nerve release: indications and technique
- Described indications and surgical technique for arthroscopic suprascapular nerve release at both notches
- Emphasized addressing compressive pathology such as ganglion cysts and ligament release
- Good outcomes with arthroscopic approach in selected patients
A distinct, examinable mechanism beyond the two compressive notches: a massive, medially retracted supraspinatus/infraspinatus tear tethers and tractions the suprascapular nerve. As the musculotendinous junction retracts medially, the nerve is drawn medially and its angle at the suprascapular notch increases, producing a traction neuropathy that compounds the wasting of the torn cuff. This is the likely reason EMG abnormalities are commoner with massive cuff tears (as in the Boykin series), and it is the rationale for nerve assessment in that setting: restoring the musculotendinous unit by repairing the retracted tear can relieve the traction, generally preferred to an isolated nerve release. Distinguish this traction mechanism from true notch entrapment by a discrete compressive lesion.
Pathophysiology
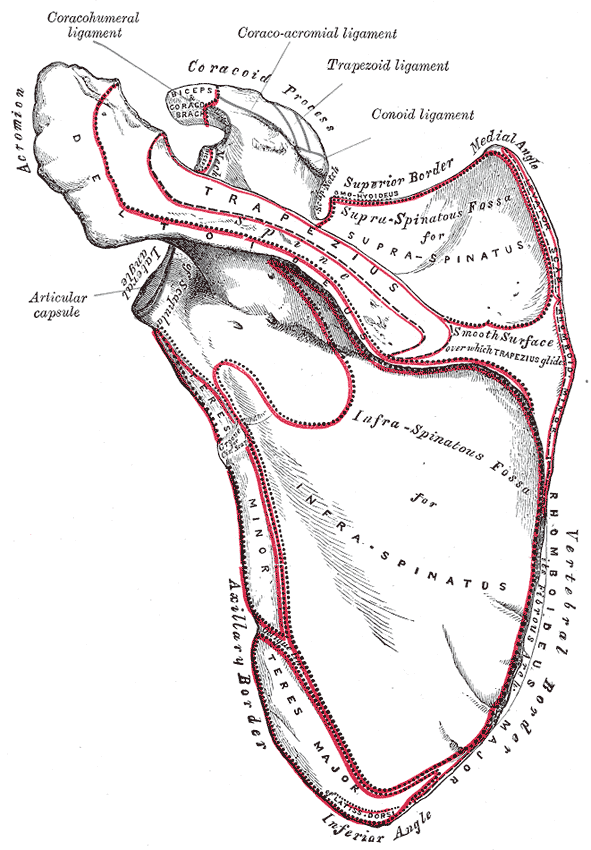
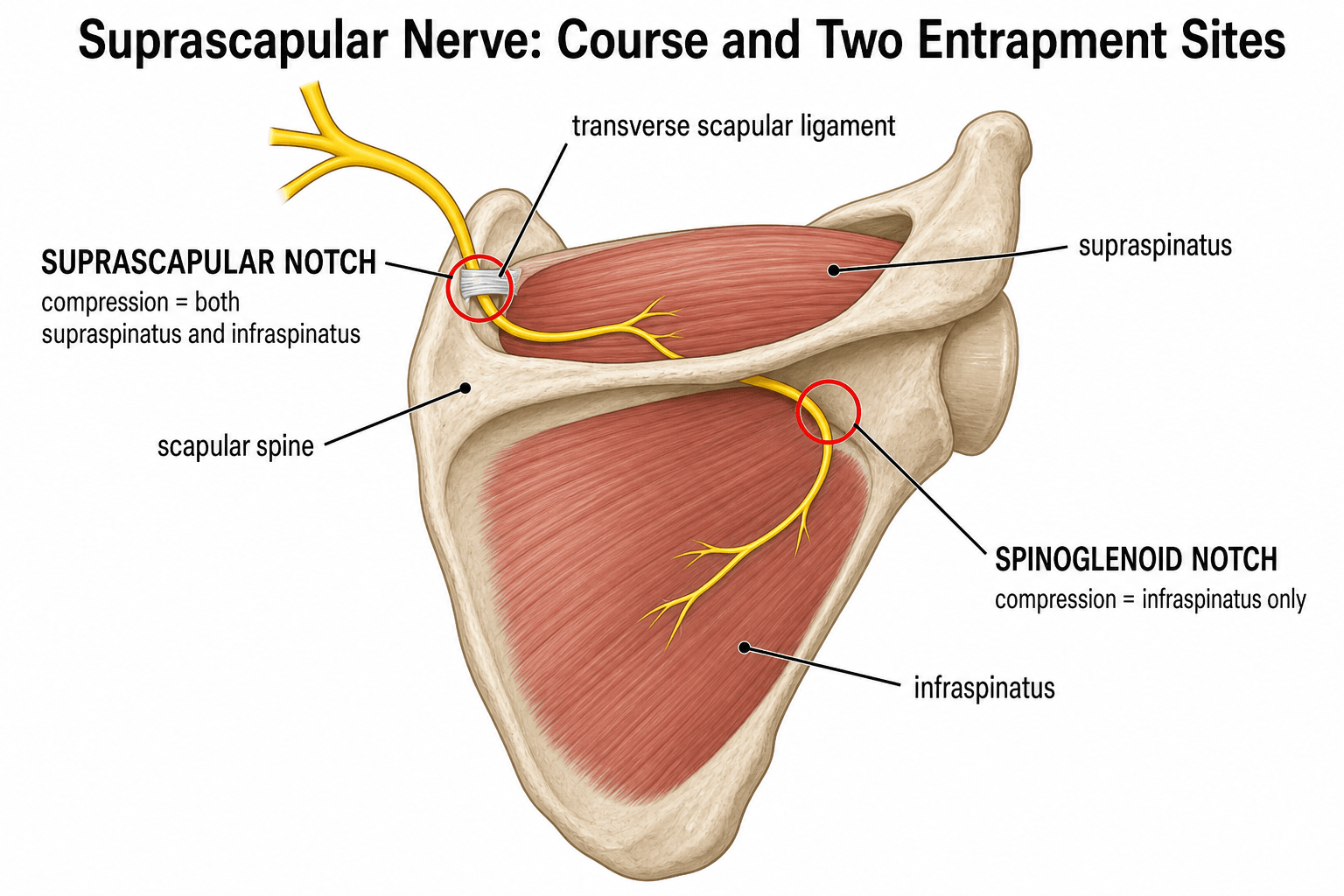
The suprascapular nerve (C5-C6, occasional C4) arises from the upper trunk of the brachial plexus. It travels posteriorly through the suprascapular notch beneath the transverse scapular ligament, giving motor branches to supraspinatus, then continues around the scapular spine through the spinoglenoid notch (under the spinoglenoid ligament) to innervate infraspinatus. Compression at the suprascapular notch affects both muscles; compression at the spinoglenoid notch isolates infraspinatus. The nerve is relatively fixed at both notches, making it vulnerable to traction and mass effect.
The suprascapular nerve is predominantly motor (supra- and infraspinatus), but it is not purely motor: beyond a small posterolateral cutaneous territory it carries articular (sensory) branches to the acromioclavicular joint, the subacromial bursa and the posterosuperior glenohumeral joint capsule - together supplying roughly 70 percent of the sensory innervation of the shoulder joint. This is the anatomical basis of the suprascapular nerve block, infiltrated at the suprascapular notch (or the floor of the supraspinatus fossa), used for analgesia in adhesive capsulitis, rheumatoid and osteoarthritic shoulder pain, post-operative pain and the palliation of malignant shoulder pain. So a "suprascapular nerve" answer that calls it purely motor is incomplete.
- Suprascapular Notch
- Supra- and infraspinatus
- Spinoglenoid Notch
- Infraspinatus only
- Suprascapular Notch
- Ligament entrapment, traction
- Spinoglenoid Notch
- Paralabral ganglion cyst
- Suprascapular Notch
- Both fossae wasting
- Spinoglenoid Notch
- Infraspinatus fossa only
- Suprascapular Notch
- Posterolateral shoulder
- Spinoglenoid Notch
- Minimal or none
Mechanism: Superior or posterosuperior labral tear allows synovial fluid to track into the spinoglenoid region, forming an expanding cyst that compresses the nerve against the notch. Recurrence is high if the labral tear is not addressed.
Timeline: Acute denervation shows fibrillations on EMG at 3-4 weeks. Chronic compression leads to muscle atrophy followed by fatty infiltration (Goutallier stages). Irreversible changes begin after 6-12 months of untreated compression.
Classification and Types
Classification by Notch Location
- Muscles Affected
- Supraspinatus + infraspinatus
- Typical Etiology
- Ligament entrapment, traction, tumour
- Treatment Focus
- Ligament release +/- notchplasty
- Muscles Affected
- Infraspinatus only
- Typical Etiology
- Paralabral ganglion cyst, labral tear
- Treatment Focus
- Cyst decompression + labral repair
Distinguishing the notch level is the single most important step in planning surgery.
Clinical Assessment
- Pain: Deep posterior shoulder pain, activity-related, night pain common
- Weakness: Difficulty with external rotation, overhead lifting, throwing
- Onset: Insidious in ganglion cases; acute after trauma or repetitive stress
- Sport / occupation: Overhead athletes, weightlifters, manual labourers
- Prior treatment: Failed physiotherapy, injections, or rotator cuff repairs
- Inspection: Infraspinatus fossa wasting (compare sides); supraspinatus wasting if proximal lesion
- Palpation: Tenderness at suprascapular or spinoglenoid notch
- Strength: External rotation weakness at side and in 90 degrees abduction
- Special tests: Hornblower sign, external rotation lag sign, positive Jobe test (if supraspinatus involved)
- Sensory: Posterolateral shoulder numbness (suprascapular notch lesions)
Infraspinatus strength testing: Patient seated, arm at side, elbow flexed 90 degrees. Resist external rotation. Weakness compared with contralateral side indicates infraspinatus dysfunction.
Hornblower sign: Patient attempts to bring hand to mouth with elbow elevated; positive if arm drops into internal rotation (infraspinatus failure).
External rotation lag sign: Passive external rotation to maximum, release; lag greater than 10 degrees indicates significant infraspinatus weakness.
Notch palpation: Tenderness 2 cm medial to posterolateral acromion (suprascapular notch) or at base of scapular spine (spinoglenoid notch).
- Wasting Pattern
- Infraspinatus +/- supraspinatus
- Discriminating Finding
- Notch tenderness, positive lag sign
- Key Test / Imaging
- EMG denervation; MRI ganglion or ligament
- Wasting Pattern
- Supraspinatus +/- infraspinatus
- Discriminating Finding
- Positive impingement, weakness on Jobe
- Key Test / Imaging
- Ultrasound or MRI shows tendon tear
- Wasting Pattern
- Deltoid, biceps, brachioradialis
- Discriminating Finding
- Neck pain, dermatomal sensory loss
- Key Test / Imaging
- Cervical MRI, EMG myotomal pattern
- Wasting Pattern
- Patchy, often multiple nerves
- Discriminating Finding
- Acute severe pain followed by weakness
- Key Test / Imaging
- EMG shows axonal neuropathy, no mass
Isolated infraspinatus atrophy with a normal supraspinatus is almost pathognomonic for spinoglenoid notch compression by a paralabral ganglion. Always obtain an MRI with intra-articular contrast or high-resolution sequences to visualise the labral tear and cyst. Missing the labral pathology leads to cyst recurrence after isolated decompression.
Investigations
Diagnostic Algorithm
Views: AP, axillary, scapular Y of shoulder Look for: Scapular notch ossification, fracture callus, bony tumours Clinical correlation: Usually normal; rules out other bony pathology
Indication: Every suspected case before surgery Findings: Fibrillations, positive sharp waves, reduced recruitment in infraspinatus (and supraspinatus if proximal) Timing: Perform at least 3-4 weeks after symptom onset; normal early EMG does not exclude diagnosis
Indication: All cases with positive EMG or high clinical suspicion Sequences: Axial and coronal oblique T2 fat-sat, MR arthrogram if labral tear suspected Findings: Ganglion cyst size and location, labral tear, muscle atrophy and fatty infiltration (Goutallier grade), ligament thickening
Indication: Bony notch narrowing, fracture callus, or tumour Benefit: Better bone detail for notchplasty planning
MRI is the key investigation once EMG confirms denervation. The combination of isolated infraspinatus atrophy plus a spinoglenoid notch ganglion on MRI is diagnostic. Always comment on labral integrity and Goutallier fatty infiltration grade, as advanced fatty change (greater than grade 2) predicts poorer functional recovery after decompression.
Management Algorithm
Non-Operative Management (First Line for Most Cases)
Goal: Reduce nerve irritation, maintain muscle function, allow spontaneous recovery in traction or idiopathic cases
Conservative Protocol
Avoid: Repetitive overhead loading, heavy lifting, contact sports Allow: Light daily activities, scapular stabilisation exercises Physiotherapy: Focus on periscapular strengthening, posture correction
Repeat clinical exam: Assess pain, strength, atrophy progression Repeat EMG: If no improvement at 3 months, consider surgery NSAIDs or analgesic: Short course for pain flare
Surgery indicated if: Progressive weakness, worsening atrophy, persistent pain affecting function, confirmed compressive lesion on MRI Continue conservative if: Stable mild symptoms, good compliance, no mass lesion
Conservative care is appropriate for idiopathic or traction-related entrapment without a space-occupying lesion. However, a documented ganglion cyst causing progressive infraspinatus atrophy is best managed surgically; delay risks irreversible fatty infiltration. Reassess every 6 weeks with objective strength testing.
Complications
Complications arise both from the untreated entrapment and from surgical decompression.
- Irreversible infraspinatus (+/- supraspinatus) atrophy with fatty infiltration (Goutallier) once compression exceeds ~6-12 months
- Permanent external-rotation weakness and loss of overhead/throwing power
- Secondary impingement and scapular dyskinesis from altered force couples
- Chronic posterior shoulder pain and reduced sporting/occupational capacity
- Cyst enlargement with intra-osseous extension or recurrent effusion if a labral tear is left untreated
- Recurrence of the ganglion cyst - the commonest failure, almost always from an unrepaired labral tear
- Iatrogenic nerve injury to the suprascapular nerve itself or the nearby axillary nerve (inferior) during spinoglenoid work
- Suprascapular artery injury (runs over the ligament at the notch) causing bleeding
- Incomplete decompression (ligament not fully divided / notch still stenotic) with persistent symptoms
- Persistent weakness despite technically successful release when advanced fatty infiltration (>Goutallier 2) was present pre-operatively
- Stiffness / failure of labral healing and standard arthroscopic risks (infection, chondral injury)
Recurrent infraspinatus symptoms after spinoglenoid cyst decompression are, until proven otherwise, due to an unaddressed labral tear allowing the cyst to reform via a one-way valve. This is why labral repair - not cyst drainage alone - is the operation. Counsel and image accordingly before any revision.
Guidelines, Registries & Global Practice
- Overhead athletes (tennis, volleyball, swimming) have the highest incidence worldwide
- Ganglion cysts are the leading cause of surgically treated spinoglenoid entrapment in all regions
- Idiopathic ligamentous compression predominates in manual labourers and older patients
- Missed diagnosis is common; many patients undergo unsuccessful rotator cuff surgery before correct identification
- High-resource centres: Routine pre-operative EMG plus high-resolution MRI; arthroscopic decompression standard
- Limited-resource settings: Clinical diagnosis and basic MRI; open ligament release remains effective
- Universal principle: Outcome depends on timely decompression before irreversible fatty infiltration
- Surgery: Concentrated in shoulder-specialist units; revision rates higher when labral pathology is missed
- Diagnosis emphasis
- EMG confirmation plus MRI for mass lesion
- Conservative care
- Activity modification and physiotherapy 3 months
- Surgical indications
- Progressive deficit or compressive mass
- Diagnosis emphasis
- Clinical + EMG; MRI for ganglion and labrum
- Conservative care
- Physiotherapy-led; early referral if no improvement
- Surgical indications
- Failed conservative or documented cyst
- Diagnosis emphasis
- High index of suspicion in overhead athletes
- Conservative care
- Individualised; shorter conservative trial in athletes
- Surgical indications
- Early surgery for ganglion cysts in young patients
- Diagnosis emphasis
- EMG and MR arthrogram for labral assessment
- Conservative care
- Sport-specific rehabilitation protocols
- Surgical indications
- Decompression before Goutallier grade 3
There is no dedicated international registry for suprascapular nerve entrapment. Evidence is derived from case series and small prospective cohorts. The consistent message across guidelines is that EMG confirms the diagnosis, MRI identifies treatable compressive pathology (especially ganglion cysts), and surgical decompression is effective when performed before advanced muscle degeneration. Always document pre-operative muscle quality and counsel patients on realistic strength recovery.
Controversies & Areas of Uncertainty
Arthroscopic techniques allow simultaneous labral repair and cyst decompression with less morbidity, but open release remains reliable for isolated suprascapular notch ligament division. No randomised trials exist; choice depends on surgeon experience and pathology.
Most authors recommend 3 months of non-operative treatment before surgery, yet athletes with documented ganglion cysts and progressive atrophy may benefit from earlier intervention. The precise threshold for "failed conservative care" is not standardised.
Some surgeons routinely perform bony notchplasty after ligament release; others reserve it for visibly stenotic notches. No comparative data define the added benefit or risk of routine bony enlargement.
Recurrent symptoms after cyst decompression are usually due to untreated labral tears. Revision rates and functional results after re-operation are poorly documented in the literature.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old right-hand-dominant tennis player presents with 4 months of posterior shoulder pain and progressive weakness in external rotation. Examination shows visible wasting of the infraspinatus fossa with preserved supraspinatus. External rotation strength is 4-/5 at the side and in 90 degrees abduction. MRI reveals a 2.5 cm spinoglenoid notch ganglion cyst with a superior labral tear. EMG confirms denervation limited to infraspinatus. What is your diagnosis and recommended treatment?”
“A 45-year-old manual labourer presents with 9 months of deep aching shoulder pain and progressive weakness. He has wasting of both supraspinatus and infraspinatus fossae. External rotation and abduction strength are reduced. No labral tear or ganglion is seen on MRI. EMG shows denervation of both supra- and infraspinatus with normal cervical paraspinals. The transverse scapular ligament appears thickened. What is your diagnosis and surgical plan?”
Key Anatomy
- Suprascapular nerve (C5-C6) passes under transverse scapular ligament at suprascapular notch
- Spinoglenoid notch lies at base of scapular spine; compression here spares supraspinatus
- Paralabral ganglion from labral tear is the most common compressive lesion at spinoglenoid notch
- Nerve is fixed at both notches, making it vulnerable to traction and mass effect
Clinical Diagnosis
- Infraspinatus wasting +/- supraspinatus wasting localises the notch level
- External rotation weakness at side and 90 degrees abduction; positive lag and hornblower signs
- Deep posterior shoulder pain, worse with overhead activity and at night
- Always examine for labral tear signs when isolated infraspinatus atrophy present
Investigations
- EMG confirms denervation pattern and level (perform greater than 3 weeks after onset)
- MRI identifies ganglion cyst, labral tear, and Goutallier fatty infiltration grade
- MR arthrogram improves labral tear detection when spinoglenoid ganglion suspected
- Normal early EMG does not exclude entrapment; repeat if high clinical suspicion
Treatment Algorithm
- Conservative first for idiopathic/traction cases: activity modification, physiotherapy 3 months
- Surgery indicated for progressive deficit, compressive mass, or failed conservative care
- Suprascapular notch: transverse scapular ligament release +/- notchplasty
- Spinoglenoid notch + ganglion: arthroscopic labral repair + cyst decompression + ligament release
Surgical Pearls
- Always address labral tear when decompressing a ganglion cyst to prevent recurrence
- Assess Goutallier grade pre-operatively; greater than grade 2 predicts poorer strength recovery
- Post-op sling 4-6 weeks, early passive ROM, scapular stabilisation, then strengthening
- Document pre-operative EMG and muscle quality; counsel on realistic functional gains
Complications & Failure
- Recurrent cyst if labral tear not repaired (most common failure mode)
- Persistent pain or weakness if advanced fatty infiltration present pre-operatively
- Nerve injury during arthroscopic decompression (rare with careful portal placement)
- Stiffness or scapular dyskinesis if rehabilitation is inadequate
Evidence Base and Key Trials
Suprascapular nerve entrapment at the spinoglenoid notch
- First clear description of isolated infraspinatus atrophy due to spinoglenoid notch compression
- Clinical and EMG correlation established the notch-specific pattern
- Surgical release improved pain and strength in reported cases
Suprascapular nerve entrapment: a meta-analysis
- Literature review (1959-2001) of 88 cases meeting inclusion criteria; entrapment is rare and occurs mainly in patients under 40 years
- A ganglion compressing the nerve was significantly commoner in males, and typically caused ISOLATED infraspinatus atrophy
- Combined supra- and infraspinatus atrophy was more typical of LIGAMENTOUS compression, and a history of trauma pointed to the ligament as the cause