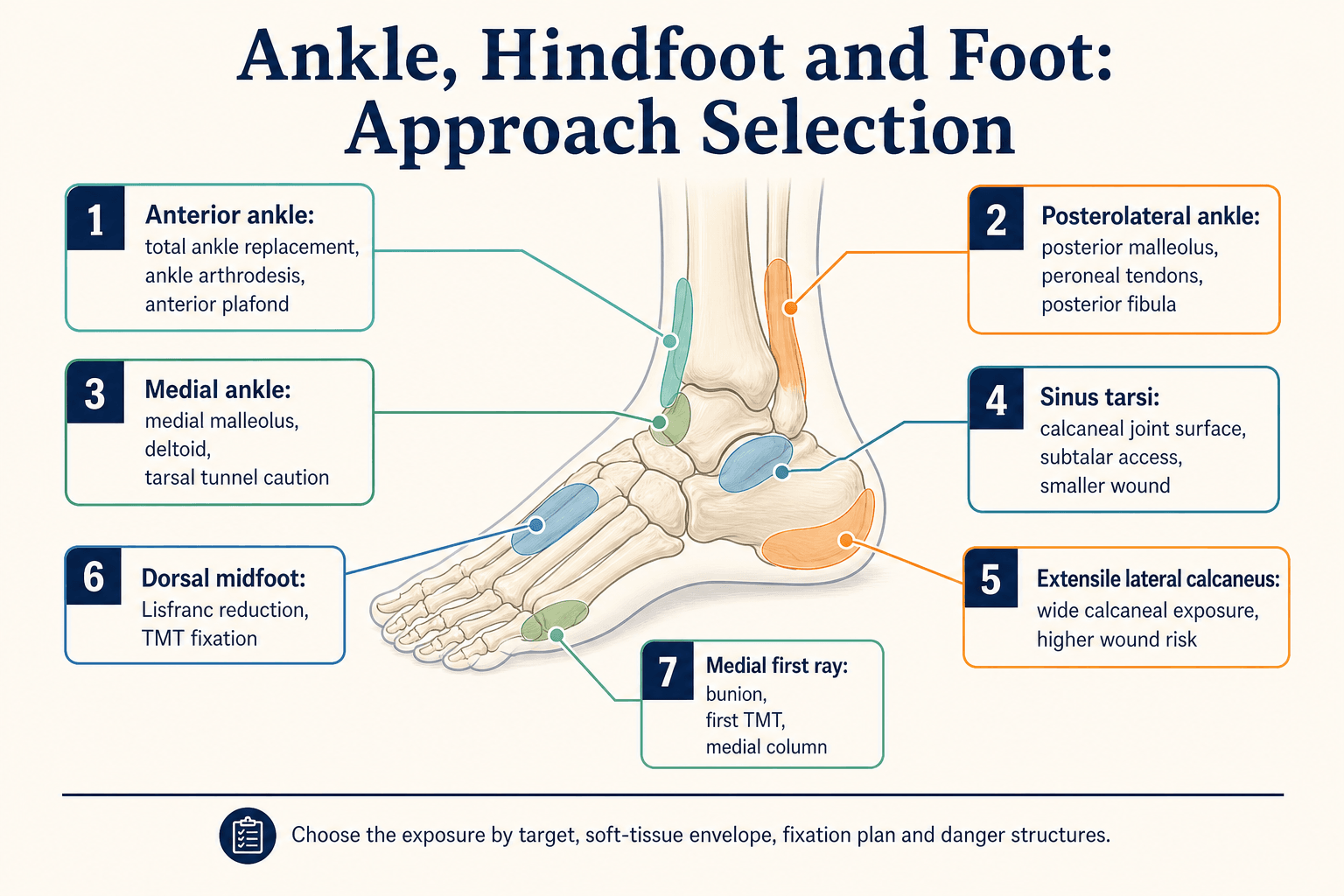
Choose the exposure by target, soft tissue and danger structures
- The approach is chosen by the structure that needs reduction, fixation, release, fusion or reconstruction.
- Swelling, scars, diabetes, smoking, vascular disease and previous incisions can make the technically familiar approach unsafe.
- Anterior ankle work risks superficial peroneal branches superficially and deep peroneal nerve with dorsalis pedis artery in the deep interval.
- Calcaneal approach choice is a soft-tissue decision as much as a fracture decision: sinus tarsi reduces wound burden but gives less extensile exposure.
- Dorsal midfoot incisions need deliberate skin bridge planning because wound breakdown over Lisfranc fixation is difficult to rescue.
- “For posterior malleolus fixation, CT pattern and reduction target matter more than fragment-size rules alone.
- “For calcaneus fractures, sinus tarsi is attractive when the joint can be reduced through a limited window; extensile lateral remains useful when wide reduction is required.
- “For total ankle replacement, the approach is linked to implant design and the planned correction strategy.
- “For any foot approach, closure and postoperative swelling control are part of the operation, not an administrative detail.
Surgical Approaches to the Ankle, Hindfoot and Foot
Do not force an approach through swollen skin, tight scars or a poor flap. In this region, the wound can fail even when the reduction or implant position is good.
- Useful Exposure
- Anterior ankle approach
- Main Risk
- Superficial peroneal branches, deep peroneal nerve, dorsalis pedis
- Practical Rule
- Mark nerves, preserve full-thickness flaps and keep interval controlled.
- Useful Exposure
- Posterolateral ankle approach
- Main Risk
- Sural nerve, lesser saphenous vein, FHL interval
- Practical Rule
- Use CT to decide whether direct posterior buttress is needed.
- Useful Exposure
- Sinus tarsi or extensile lateral
- Main Risk
- Lateral wound flap, sural nerve, peroneal tendons
- Practical Rule
- Pick the smallest exposure that still permits accurate reduction.
- Useful Exposure
- Dorsal midfoot windows
- Main Risk
- Dorsalis pedis, deep peroneal nerve, skin bridge
- Practical Rule
- Plan incisions around columns and fixation, not just the visible diastasis.
- Useful Exposure
- Medial first-ray or medial column approach
- Main Risk
- Dorsomedial cutaneous nerve, capsule, wound irritation
- Practical Rule
- Protect skin and plan correction, fixation and shoe-wear implications.
SAFEApproach Description
Hook:SAFE keeps the approach practical.
DRAPEFoot and Ankle Setup
Hook:DRAPE before the incision.
Overview and Indications
Foot and ankle approaches are high-risk because the operative targets are small, the skin envelope is thin, and the incisions often lie directly over implants. A safe approach begins by defining the target: ankle joint, posterior malleolus, distal fibula, medial malleolus, talus, calcaneus, subtalar joint, Lisfranc complex, medial column, first ray or lesser rays.
The second decision is the soft-tissue route. A perfect bony plan is not useful if the incision crosses compromised skin or creates a flap that cannot survive. Open fractures, diabetes, peripheral vascular disease, neuropathy, smoking, oedema, previous scars and swelling after high-energy trauma all shift the balance toward staged surgery, limited exposure or a different incision.
CT pattern, swelling, reduction target and fixation surface decide whether exposure is direct, limited, extensile or staged.
Deformity correction needs an approach that permits release, correction, fixation and safe closure.
Implant design, bone preparation, alignment correction and wound risk influence anterior, lateral, transfibular or arthroscopic choices.
For calcaneus, posterior malleolus, Lisfranc and total ankle surgery, the approach is not just anatomy recall. It determines whether reduction, fixation, wound healing and later reconstruction are realistic.
Relevant Anatomy
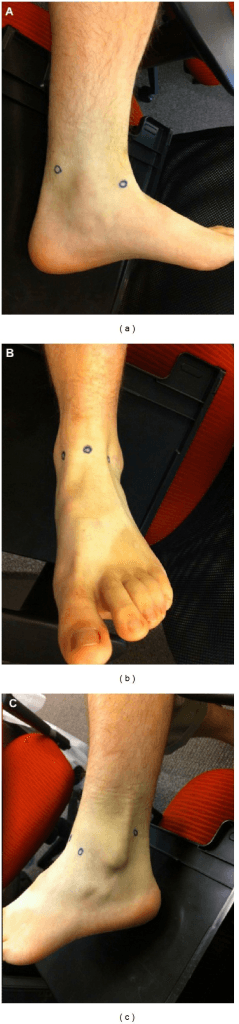
The foot and ankle contain many named structures in shallow tissue planes. The main safety rule is simple: identify the structure at risk before retraction, not after bleeding, numbness or tendon injury occurs.
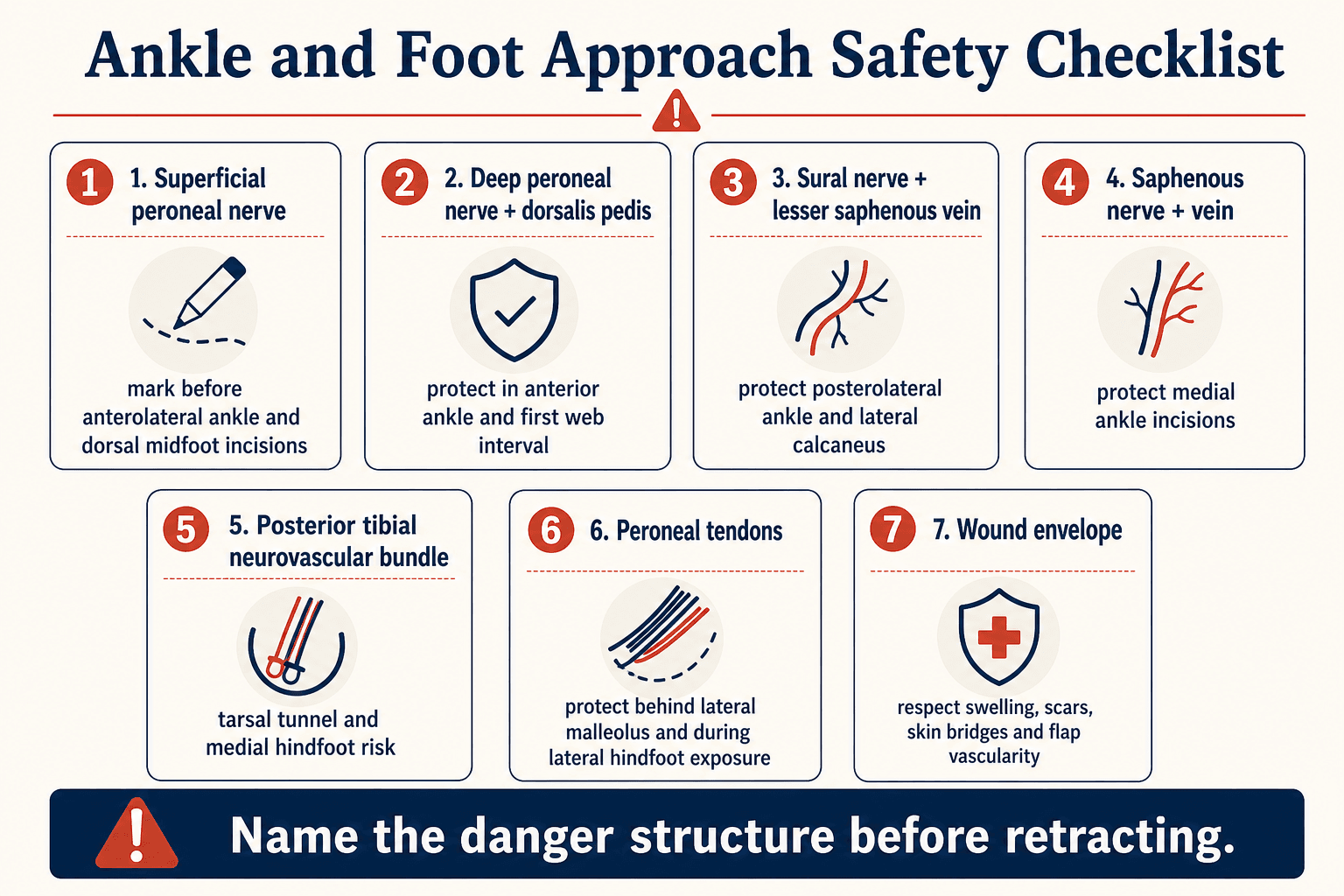
- Where It Matters
- Anterolateral ankle, dorsal midfoot
- Practical Protection
- Mark branches if visible or palpable; avoid blind subcutaneous spreading.
- Where It Matters
- Anterior ankle and first web interval
- Practical Protection
- Stay in the correct interval and protect the deep bundle during anterior ankle work.
- Where It Matters
- Posterolateral ankle, lateral calcaneus
- Practical Protection
- Plan incision and retraction with the nerve course in mind.
- Where It Matters
- Medial ankle and medial column
- Practical Protection
- Protect superficial structures during medial incisions.
- Where It Matters
- Tarsal tunnel and medial hindfoot
- Practical Protection
- Avoid uncontrolled deep medial dissection; know the bundle position before release.
- Where It Matters
- Lateral malleolus and lateral calcaneus
- Practical Protection
- Protect tendon sheath and avoid iatrogenic subluxation or irritation.
- Where It Matters
- Calcaneus, Lisfranc, arthroplasty and revision surgery
- Practical Protection
- Create full-thickness flaps and avoid narrow threatened bridges.
Foot and ankle implants often sit under thin skin. If closure requires tension, rethink fixation prominence, flap handling, drains, negative-pressure dressing and postoperative swelling control.
Internervous Plane and Intervals
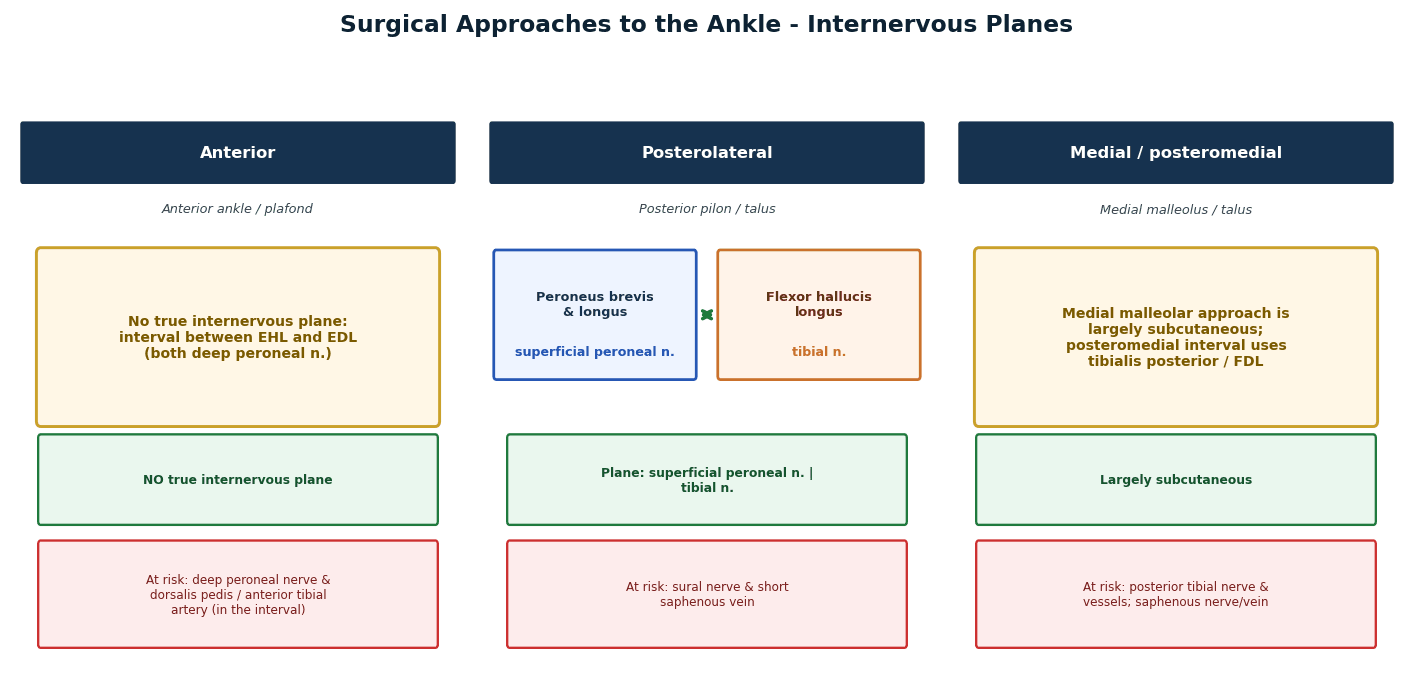
Some exposures use named internervous planes. Many foot and ankle approaches are better described as tendon windows, safe corridors or direct subperiosteal exposures. In practice, the important step is to state the interval and the structures at risk.
- Plane or Window
- Between tibialis anterior and EHL or between EHL and EDL depending target
- Target
- TAA, arthrodesis, anterior plafond
- Main Risk
- Deep peroneal nerve and dorsalis pedis; superficial peroneal branches.
- Plane or Window
- Between peroneal tendons and FHL region
- Target
- Posterior malleolus, posterior fibula, peroneal tendons
- Main Risk
- Sural nerve, lesser saphenous vein, FHL handling.
- Plane or Window
- Direct medial malleolar or deltoid exposure; deeper tarsal tunnel region when indicated
- Target
- Medial malleolus, deltoid, talus
- Main Risk
- Saphenous structures superficially; posterior tibial bundle posteriorly.
- Plane or Window
- Lateral interval through sinus tarsi toward posterior facet
- Target
- Calcaneal posterior facet and subtalar joint
- Main Risk
- Sural nerve branches, peroneal tendons, limited visualisation.
- Plane or Window
- Full-thickness lateral flap based on lateral calcaneal wall
- Target
- Wide calcaneal reduction and plating
- Main Risk
- Wound edge necrosis, sural nerve, peroneal tendons.
- Plane or Window
- Dorsal windows between extensor tendons and neurovascular structures
- Target
- Lisfranc and TMT fixation
- Main Risk
- Deep peroneal nerve, dorsalis pedis and skin bridge.
Fragment size alone is an unreliable approach rule. The CT pattern, syndesmotic stability, articular impaction, posterior incisura involvement and ability to reduce the fragment decide whether direct posterior exposure is useful.
Closure and Wound Management
Closure is part of the approach. Foot and ankle incisions sit close to tendons, implants and bony prominences. A wound that closes under tension should be treated as a warning sign, not as a cosmetic issue.
Reassess hardware prominence, tendon position, haemostasis, drain need and whether the skin can close without tension.
Splint or boot position should reduce tension on the incision and protect the repair or fixation.
Check wound edge viability, swelling, sensation, pin sites and signs of infection before weight-bearing progression.
If the patient has diabetes, neuropathy, vascular disease, smoking, revision surgery, severe swelling or multiple incisions, state the wound-risk plan explicitly.
Patient Positioning
Positioning must allow exposure, reduction and imaging. Before draping, check the image intensifier can obtain the views needed for the operation: ankle AP, mortise, lateral, Broden, Harris axial, oblique foot or weight-bearing comparison images when relevant.
- Best Use
- Anterior ankle, medial malleolus, medial column, many forefoot procedures
- Practical Checks
- Bump under hip if needed; foot at table end; confirm mortise and lateral imaging.
- Best Use
- Extensile lateral calcaneus, sinus tarsi, lateral hindfoot, peroneal tendons
- Practical Checks
- Pad bony prominences; protect peroneal nerve at fibular head; check lateral and axial views.
- Best Use
- Posterior ankle, FHL, posterior malleolus in selected workflows
- Practical Checks
- Airway, pressure areas, image access and conversion plan matter.
- Best Use
- Posterolateral ankle in selected fracture fixation
- Practical Checks
- Allows combined medial/lateral access when posterior exposure is limited but needed.
- Best Use
- Ankle arthroscopy, subtalar arthroscopy, selected fusions
- Practical Checks
- Portal safety, nerve marking and distraction force must be controlled.
Surgical Technique
total ankle replacement, open ankle arthrodesis, anterior plafond work, anterior osteophytes and anterior ankle exposure.
- Supine position, foot at end of table, tourniquet if used, fluoroscopy checked.
- Mark tibialis anterior, EHL, EDL, superficial peroneal branches if visible, and the planned incision.
- Use a longitudinal anterior incision centred over the ankle joint and planned implant or fusion surface.
- Develop full-thickness flaps; avoid thin undermined skin.
- Identify the interval. Commonly work between tibialis anterior and EHL or between EHL and EDL according to target.
- Protect the deep peroneal nerve and dorsalis pedis artery in the deep anterior interval.
- Expose the capsule, open the joint and perform the planned preparation, reduction, fusion or arthroplasty steps.
- Close capsule and retinacular layers carefully; avoid prominent implants under the incision.
superficial peroneal neuritis, deep peroneal injury, wound breakdown, extensor tendon irritation and poor access to posterior deformity.
Structures at Risk and Pitfalls
The most common error is treating a foot and ankle approach as a named incision rather than a wound-risk decision. The second error is not matching the exposure to the reduction or fixation target.
- Why It Matters
- Thin skin and oedema increase breakdown risk.
- Prevention
- Delay definitive surgery or use staged/limited exposure when needed.
- Why It Matters
- An indirect screw may not control a posterior shear fragment.
- Prevention
- Read CT and choose direct buttress when the pattern requires it.
- Why It Matters
- Flap necrosis can be limb-threatening in high-risk patients.
- Prevention
- Wait for soft-tissue readiness or use limited/percutaneous strategies.
- Why It Matters
- Wound failure occurs directly over implants.
- Prevention
- Plan incisions around columns and expected fixation.
- Why It Matters
- Neuroma, numbness and pain can dominate the outcome.
- Prevention
- Mark, identify and protect superficial peroneal, sural and saphenous structures.
- Why It Matters
- Irritation, tendon wear and wound compromise.
- Prevention
- Contour and bury hardware appropriately; check closure before finalising.
A limited approach still needs full reduction strategy, fluoroscopic control, percutaneous tools, safe fixation and a plan if the reduction cannot be achieved.
Guidelines, Registries & Global Practice
Foot and ankle approach decisions are made worldwide against a backdrop of common biomechanical principles but very different resource settings. The unifying message across societies is soft-tissue-first surgery.
Global epidemiology
- Ankle fractures are among the most common lower-limb fractures, with rising incidence in older adults driven by fragility and rotational injuries.
- Calcaneal fractures are the most common tarsal fracture, typically high-energy axial-loading injuries in working-age adults, and frequently bilateral or associated with spinal injury.
- Lisfranc injuries are commonly missed on initial plain films; delayed diagnosis worsens outcome, so weight-bearing or CT imaging is emphasised internationally.
- Emphasis
- Approach atlas, internervous planes and staged management.
- Practical Point
- Definitive fixation timed to soft-tissue recovery; full-thickness flaps; named nerve protection.
- Emphasis
- Open fracture and ankle fracture standards; ortho-plastic pathways.
- Practical Point
- Severe open foot and ankle injuries managed jointly in major-trauma networks with early debridement and definitive cover.
- Emphasis
- Evidence-based appropriate-use guidance for ankle and foot trauma.
- Practical Point
- Selective operative indications; emphasis on patient factors and soft-tissue status.
- Emphasis
- Consensus on calcaneus and Lisfranc management.
- Practical Point
- Growing support for sinus tarsi and minimally invasive calcaneal fixation; CT-based Lisfranc decisions.
Registry and trial signals
- National joint registries (NJR UK, AOANJRR Australia, the Swedish and New Zealand registries) increasingly track total ankle replacement survivorship, informing the anterior versus lateral approach debate by linking implant and exposure to revision rates.
- The UK Heel Fracture Trial remains the strongest randomised signal shaping how aggressively the calcaneus is exposed.
High- versus limited-resource practice variation
Staged protocols, CT planning, negative-pressure dressings, ortho-plastic teams, total ankle replacement and arthroscopic fusion are widely available, favouring soft-tissue-sparing and minimally invasive approaches.
Delayed presentation, limited CT, and infection risk push practice toward conservative management of many calcaneal fractures, percutaneous or limited approaches, and external fixation where soft tissues or implants are constrained.
State the shared principle first (soft-tissue-first, named-nerve protection, CT-guided decisions), then acknowledge that approach availability and threshold to operate vary with resources and the strength of randomised evidence.
Controversies and Areas of Uncertainty
Approach selection around the foot and ankle is one of the most actively debated areas in trauma surgery because the same fracture can be reached several ways with very different wound risks. The exam reward is not picking a "right" incision but explaining the trade-off.
- Argument For
- Restores Bohler angle, hindfoot width and subtalar congruity.
- Counter-argument
- UK Heel Fracture Trial showed no 2-year benefit and far higher complications.
- Pragmatic Position
- Selective surgery: tongue-type, gross varus, open or soft-tissue-threatening patterns, young high-demand patients.
- Argument For
- Extensile gives wide exposure for comminuted Sanders III/IV.
- Counter-argument
- Sinus tarsi halves wound complications with similar angle restoration.
- Pragmatic Position
- Default to sinus tarsi; reserve extensile for fractures it cannot reduce, once the envelope is ready.
- Argument For
- Old teaching fixed fragments over 25 to 33% of the plafond.
- Counter-argument
- Step-off and morphology, not size, drive arthritis and stability.
- Pragmatic Position
- Use a CT-based classification (Bartonicek/Mason) and posterolateral ORIF for joint-involving shear fragments.
- Argument For
- ORIF preserves native joints and motion.
- Counter-argument
- Primary arthrodesis lowers reoperation in ligamentous patterns (Henning RCT).
- Pragmatic Position
- Fix bony injuries anatomically; favour primary arthrodesis for purely ligamentous instability.
- Argument For
- Anterior is familiar and restores tibial slope.
- Counter-argument
- Lateral allows anatomic axial implant placement.
- Pragmatic Position
- Approach follows implant design and the planned deformity correction, not surgeon habit alone.
Examiners escalate by changing the soft tissues, the comorbidities or the fracture morphology. A candidate who insists on one approach regardless of these variables loses marks; a candidate who states the decision rule and adapts gains them.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has a trimalleolar ankle fracture. CT shows a posterolateral posterior malleolar fragment with posterior incisura involvement and syndesmotic instability.”
“A patient has a displaced intra-articular calcaneal fracture. The skin is swollen but improving. You are asked whether you would use a sinus tarsi or extensile lateral approach.”
“A patient has a Lisfranc fracture-dislocation requiring operative reduction and fixation. You are asked to describe your approach.”
Opening Line
- I choose the approach by operative target, CT morphology, fixation plan, soft-tissue envelope and danger structures.
- The incision is unsafe if the wound cannot close or if the danger structure has not been named.
Danger Structures
- Anterior ankle: superficial peroneal branches, deep peroneal nerve and dorsalis pedis.
- Posterolateral ankle and lateral calcaneus: sural nerve, lesser saphenous vein, peroneal tendons.
- Medial ankle: saphenous nerve and vein superficially; posterior tibial neurovascular bundle deeply.
Approach Decisions
- Posterior malleolus: use CT, not fragment size alone.
- Calcaneus: sinus tarsi for limited safe reduction; extensile lateral for wide reduction when the soft tissues allow.
- Lisfranc: dorsal windows must preserve skin bridges and permit anatomic second-ray reduction.
Technique Priorities
- Confirm imaging before draping.
- Raise full-thickness flaps where flaps are required.
- Avoid prominent hardware under thin skin.
- Closure, immobilisation and wound review are part of the approach.
Evidence Base
Posterior Malleolus: Posterolateral ORIF Beats A-to-P Screws
- Fragment size is NOT a reliable indication for fixation; articular step-off is the key driver of arthritis.
- Posterolateral ORIF outperformed percutaneous anterior-to-posterior screws.
- Posterior fragments involving the joint surface should be anatomically reduced and buttressed.