Synovium Structure | Type A and B Synoviocytes | Hyaluronic Acid | Boundary and Fluid Film Lubrication
- Synovium lacks basement membrane - unique feature allowing bidirectional diffusion for joint nutrition
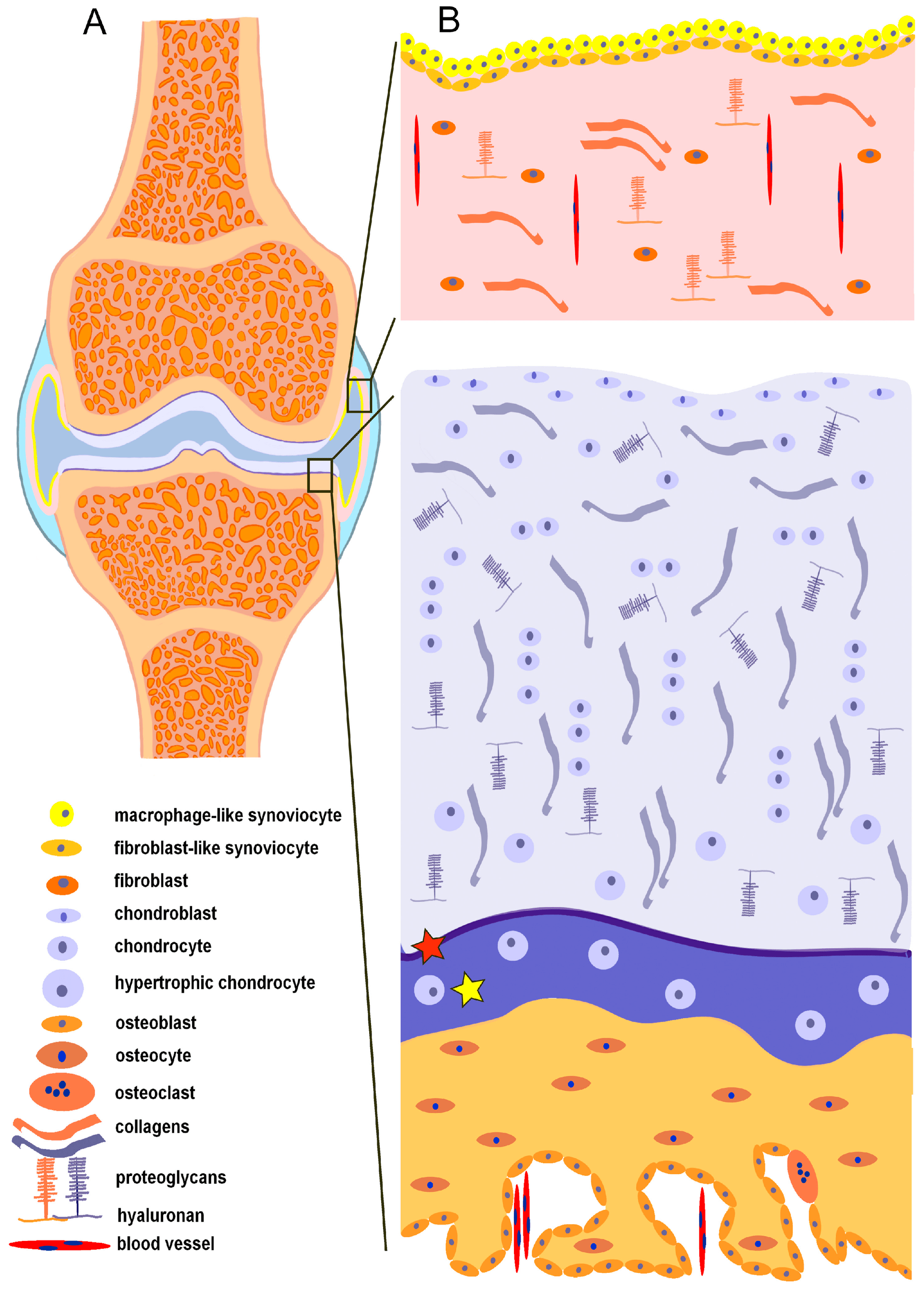
- Type A synoviocytes are macrophage-like (CD68+) and remove debris via phagocytosis
- Type B synoviocytes are fibroblast-like and synthesize hyaluronic acid for synovial fluid viscosity
- Hyaluronic acid (MW 3-4 MDa) provides non-Newtonian viscosity for lubrication
- Boundary lubrication (lubricin/PRG4) prevents solid-solid contact at low speeds; fluid film lubrication at high speeds
- “Normal synovial fluid is acellular (under 200 WBC/μL) with no organisms on Gram stain
- “Septic arthritis: over 50,000 WBC/μL with over 75% neutrophils, positive culture
- “Inflammatory arthritis: 2,000-50,000 WBC/μL, rheumatoid factor may be present
- “Lubrication mechanisms differ by speed: boundary (static/low speed) vs fluid film (high speed)
Synovium lacks basement membrane - unique feature among body membranes. The intima (lining layer) is 1-3 cells thick with Type A (macrophage-like) and Type B (fibroblast-like) synoviocytes. Subintima is vascular connective tissue.
Hyaluronic acid (hyaluronan) is a high molecular weight (3-4 MDa) glycosaminoglycan synthesized by Type B synoviocytes. Provides non-Newtonian viscosity: high viscosity at low shear (shock absorption), low viscosity at high shear (ease of movement).
Two lubrication modes: (1) Boundary lubrication by lubricin (PRG4) adsorbed to cartilage surface prevents solid-solid contact at low speeds. (2) Fluid film lubrication by pressurized synovial fluid separates surfaces at high speeds.
Normal synovial fluid: Clear, yellow, viscous, acellular (under 200 WBC/μL). Septic arthritis: Purulent, over 50,000 WBC/μL, over 75% PMNs, positive culture. Crystal arthropathy: Monosodium urate (gout, negative birefringence), calcium pyrophosphate (pseudogout, positive birefringence).
TYPE ABTYPE AB - Synoviocyte Functions
Hook:TYPE AB blood types remind you: Type A cleans (macrophage), Type B builds (fibroblast)
Overview and Introduction
The synovium is a specialized mesenchymal tissue that lines the non-cartilaginous surfaces of synovial joints. It produces synovial fluid, which provides nutrition to avascular articular cartilage and enables nearly frictionless joint motion through sophisticated lubrication mechanisms.
Synovial fluid is a dialysate of plasma enriched with hyaluronic acid (hyaluronan), a high molecular weight glycosaminoglycan that provides unique viscoelastic properties essential for joint function.
Core Concepts
Five concepts unify this topic and recur throughout the basic-science viva:
- The intima has no basement membrane. This unique feature permits bidirectional diffusion that nourishes avascular articular cartilage and allows rapid fluid exchange.
- Two synoviocytes, two jobs. Type A (macrophage-like, CD68+) clear debris and present antigen; Type B (fibroblast-like, vimentin+) synthesise hyaluronan and lubricin.
- Hyaluronan is a glycosaminoglycan, not a proteoglycan (no protein core); its high molecular weight (3-4 MDa) gives synovial fluid non-Newtonian, shear-thinning viscosity.
- Two lubrication regimes. Boundary lubrication (lubricin/PRG4) dominates at low speed/high load; fluid-film lubrication (hyaluronan-rich fluid) dominates at high speed.
- Synovial fluid analysis is diagnostic. Cell count, differential, crystals and culture separate normal, non-inflammatory, inflammatory and septic categories.
Synovium Anatomy and Histology
Macroscopic Anatomy
Location and distribution:
- Lines joint capsule, intra-articular ligaments, and bone surfaces not covered by cartilage
- Does NOT cover articular cartilage or menisci
- Extends to bone-cartilage junction (tidemark region)
- Forms synovial folds (plicae) and villi that increase surface area
Macroscopic appearance:
- Thin membrane (0.1-0.3 mm thickness)
- Smooth, glistening surface
- Pink to pale red color (vascular)
- Highly vascular and innervated
Microscopic Structure
The synovium has two distinct layers:
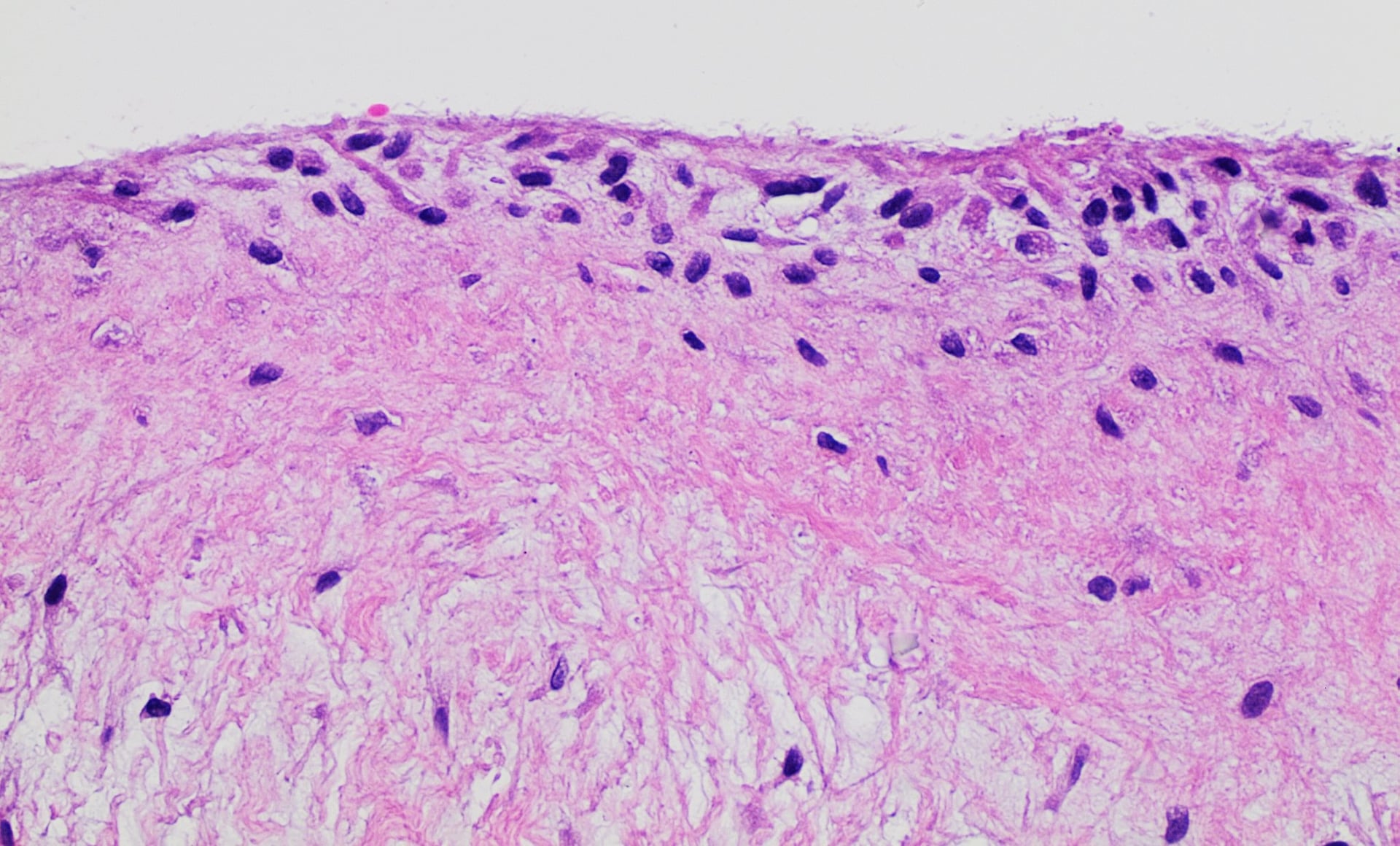
1. Intima (Lining Layer):
- Thickness: 1-3 cell layers (20-40 micrometers)
- Cell types: Type A and Type B synoviocytes
- NO basement membrane - unique feature allowing bidirectional diffusion
- Intercellular gaps: Allow molecules up to 10-20 nm to pass freely
- Function: Synovial fluid production, nutrition of cartilage, debris removal
2. Subintima (Sublining Layer):
- Structure: Loose connective tissue rich in blood vessels, lymphatics, and nerves
- Three subtypes based on predominant tissue:
- Fibrous (collagenous) - most common, near capsule
- Areolar (loose connective tissue) - most common, near bone
- Adipose (fat tissue) - near fat pads
- Function: Vascular supply, immune surveillance, structural support
Understanding the lack of basement membrane is critical - this allows efficient nutrient exchange for avascular cartilage.
Synovial Fluid Composition and Properties
Synovial Fluid Components
Normal synovial fluid characteristics:
- Volume: 0.3-3.5 mL in knee (varies by joint size)
- Color: Clear to pale yellow (straw-colored)
- Viscosity: High (due to hyaluronic acid)
- Clarity: Transparent (can read newsprint through it)
- Cell count: Under 200 WBC/μL (under 25% neutrophils)
Composition:
1. Plasma dialysate (base fluid):
- Water: 85%
- Electrolytes: Similar to plasma (Na+, K+, Cl-, Ca2+, Mg2+)
- Glucose: 90-100% of plasma glucose (50-100 mg/dL)
- Small molecules diffuse freely from blood
2. Hyaluronic acid (key component):
- Concentration: 3-4 mg/mL (0.3-0.4%)
- Molecular weight: 3-4 million Daltons (3-4 MDa)
- Source: Synthesized by Type B synoviocytes
- Function: Provides viscosity and elasticity
3. Lubricin (PRG4):
- Glycoprotein: 227 kDa molecular weight
- Source: Synthesized by Type B synoviocytes and chondrocytes
- Function: Boundary lubrication, prevents cartilage adhesion
- Concentration: 50-400 micrograms/mL
4. Proteins:
- Total protein: 1-2 g/dL (one-third of plasma protein concentration)
- Albumin: Predominant protein (passes through synovial membrane easily)
- Immunoglobulins: IgG, IgM, IgA present in lower concentrations than plasma
- Enzymes: Collagenase, hyaluronidase (at low levels normally)
5. Cells:
- Total WBC: Under 200/μL (mostly mononuclear)
- Cell types: Monocytes, lymphocytes, synoviocytes (shed from intima)
- No RBCs in normal fluid
Normal synovial fluid is essentially a plasma ultrafiltrate enriched with hyaluronic acid and lubricin.
HYALURONICHYALURONIC - Hyaluronic Acid Properties
Hook:HYALURONIC = HY molecular weight gives LUBRICation
Joint Lubrication Mechanisms
Two Primary Lubrication Mechanisms
Joints achieve remarkably low friction (coefficient 0.001-0.01) through two complementary mechanisms that operate under different conditions:
1. Boundary Lubrication:
- Active when: Static loading, low sliding speeds, high loads
- Mechanism: Lubricin adsorbed to cartilage surface prevents solid-solid contact
- Lubricant: Lubricin (PRG4) - glycoprotein
- Coefficient of friction: 0.01-0.02
2. Fluid Film Lubrication:
- Active when: High sliding speeds, low to moderate loads
- Mechanism: Pressurized synovial fluid separates opposing cartilage surfaces
- Lubricant: Synovial fluid (water + hyaluronic acid)
- Coefficient of friction: 0.001-0.005
3. Additional mechanisms (contribute but less dominant):
- Weeping lubrication: Fluid exudes from cartilage matrix under load
- Boosted lubrication: HA macromolecules concentrate in gap, increasing viscosity locally
- Hydration lubrication: Hydrated phospholipid layers on cartilage surface
- Boundary Lubrication
- Low speed, high load
- Fluid Film Lubrication
- High speed, low-moderate load
- Boundary Lubrication
- Lubricin (PRG4)
- Fluid Film Lubrication
- Synovial fluid (HA + water)
- Boundary Lubrication
- Adsorbed molecular layer
- Fluid Film Lubrication
- Pressurized fluid film
- Boundary Lubrication
- 0.01-0.02
- Fluid Film Lubrication
- 0.001-0.005
- Boundary Lubrication
- Standing, static loading
- Fluid Film Lubrication
- Walking, running
The two mechanisms work together to provide lubrication across the full range of joint activities.
BOUNDARYBOUNDARY - Lubrication Mechanisms
Hook:BOUNDARY keeps cartilage surfaces apart at the boundary between static and moving
Synovial Fluid Analysis - Clinical Pathology
Classification of Synovial Fluid
- Normal
- Clear/pale yellow
- Non-inflammatory
- Yellow
- Inflammatory
- Yellow/cloudy
- Septic
- Purulent/opaque
- Normal
- Transparent
- Non-inflammatory
- Transparent
- Inflammatory
- Translucent/opaque
- Septic
- Opaque
- Normal
- High
- Non-inflammatory
- High
- Inflammatory
- Low
- Septic
- Very low
- Normal
- under 200/μL
- Non-inflammatory
- 200-2,000/μL
- Inflammatory
- 2,000-50,000/μL
- Septic
- over 50,000/μL
- Normal
- under 25%
- Non-inflammatory
- under 25%
- Inflammatory
- over 50%
- Septic
- over 75%
- Normal
- Negative
- Non-inflammatory
- Negative
- Inflammatory
- Negative
- Septic
- Positive (50-70%)
Key diagnostic thresholds:
- Normal: Under 200 WBC/μL
- Non-inflammatory (OA, trauma): 200-2,000 WBC/μL
- Inflammatory (RA, gout, pseudogout): 2,000-50,000 WBC/μL
- Septic: Over 50,000 WBC/μL (classic), but can overlap with inflammatory
Septic arthritis is a surgical emergency. Classic findings: WBC over 50,000/μL, over 75% PMNs, positive Gram stain or culture. However, WBC counts can overlap with inflammatory arthritis. Always correlate with clinical presentation (fever, acute monoarthritis). If suspicion is high, treat as septic until proven otherwise (washout and antibiotics).
Understanding synovial fluid classification guides diagnosis and management.
Pathophysiology of Synovial Diseases
Inflammatory Arthritis (Rheumatoid Arthritis)
Synovial pathology:
- Synovial hypertrophy: Intimal lining proliferates (10-20 cell layers thick vs normal 1-3)
- Pannus formation: Invasive synovial tissue (granulation tissue) erodes cartilage and bone
- Inflammatory infiltrate: Lymphocytes (T and B cells), plasma cells, macrophages in subintima
- Neovascularization: VEGF-driven angiogenesis brings more inflammatory cells
- Cytokine production: TNF-alpha, IL-1, IL-6 drive inflammation and joint destruction
Synovial fluid changes:
- High WBC count: 5,000-50,000/μL (inflammatory range)
- Neutrophil predominance: 50-75% PMNs
- Low viscosity: Hyaluronic acid degraded by hyaluronidase and free radicals
- Low complement: C3 and C4 consumed by immune complexes
- Rheumatoid factor: May be present
Osteoarthritis
Synovial pathology:
- Mild synovitis: Low-grade inflammation (not as severe as RA)
- Fibrosis: Subintimal fibrosis and thickening
- Cartilage fragments: Released into joint, phagocytosed by Type A synoviocytes
Synovial fluid changes:
- Low WBC count: 200-2,000/μL (non-inflammatory)
- Normal to decreased viscosity: HA molecular weight decreases over time
- Cartilage debris: May contain fragments
Septic Arthritis
Synovial pathology:
- Acute inflammation: Massive neutrophil infiltration
- Purulent exudate: Pus formation
- Cartilage destruction: Bacterial enzymes and neutrophil proteases degrade cartilage rapidly
- Vascular thrombosis: Can lead to bone infarction
Synovial fluid changes:
- Very high WBC count: Over 50,000/μL (often over 100,000)
- Neutrophil predominance: Over 75% (often over 90%)
- Positive culture: Staphylococcus aureus most common
- Low glucose: Bacteria consume glucose
- Very low viscosity: Complete HA degradation
Pigmented Villonodular Synovitis (Tenosynovial Giant Cell Tumour)
The classic PRIMARY proliferative disorder of synovium that a synovium topic must cover - and it is now understood to be a true clonal neoplasm, not merely inflammation. Pigmented villonodular synovitis (PVNS) is grouped with giant cell tumour of tendon sheath as tenosynovial giant cell tumour (TGCT). It is driven by overexpression of CSF1 (colony-stimulating factor 1), frequently through a chromosomal translocation involving the CSF1 gene; the few neoplastic cells then recruit a bulky reactive population of CSF1R-bearing macrophages.
- Two forms: localised (a discrete nodule - the intra-articular nodular form, or its digit equivalent giant cell tumour of the tendon sheath) and diffuse (the classic intra-articular diffuse-type lesion, most often the knee, then hip).
- Presentation: insidious monoarticular swelling and pain with recurrent atraumatic, serosanguinous or dark-brown effusion/haemarthrosis and mechanical symptoms, in a young-to-middle-aged adult.
- Imaging: MRI is diagnostic - nodular synovial proliferation that is low signal on both T1 and T2 with characteristic "blooming" artefact on gradient-echo sequences from haemosiderin deposition; aspirate is classically brown.
- Treatment: synovectomy (arthroscopic for localised; open or combined for diffuse), with high recurrence in diffuse disease; radiosynovectomy is an adjunct, and a systemic CSF1R inhibitor (pexidartinib) is used for diffuse, recurrent or unresectable disease. Untreated diffuse disease causes secondary cartilage and bone destruction.
Synovial Chondromatosis
The other primary synovial proliferative disorder, also absent from most candidates' answers. Primary synovial (osteo)chondromatosis is a benign metaplasia of the synovial intima producing multiple cartilaginous nodules that ossify and detach as loose bodies; it is a clonal process associated with FN1-ACVR2A gene fusions. It is distinct from secondary chondromatosis, in which loose bodies arise from a degenerate/osteoarthritic joint or osteochondral fragments.
- Presentation: monoarticular (knee most common, then hip, elbow, shoulder) pain, swelling, crepitus and locking/catching from loose bodies, with reduced range of motion.
- Imaging: multiple intra-articular calcified/ossified bodies with "ring-and-arc" chondroid mineralisation on radiographs - characteristically uniform in size in the primary form; non-mineralised cartilage bodies are shown on MRI/CT.
- Milgram staging: phase I (active intrasynovial disease, no loose bodies), phase II (transitional - intrasynovial disease plus loose bodies), phase III (free loose bodies, synovial disease quiescent).
- Treatment: removal of loose bodies plus synovectomy to reduce recurrence. Be alert to the rare malignant transformation to secondary chondrosarcoma, suggested by aggressive recurrence and bone destruction.
Differential Diagnosis of the Acutely Swollen Joint
The single most important decision after arthrocentesis is distinguishing septic arthritis from its mimics, because untreated infection destroys cartilage within days. Crystals and infection can coexist, so a positive crystal result does NOT exclude sepsis.
- Typical synovial WBC
- over 50,000/μL (often over 100,000)
- PMN %
- over 90%
- Discriminating feature
- Positive Gram stain/culture; low glucose; raised synovial lactate
- Key action
- Urgent washout + IV antibiotics
- Typical synovial WBC
- 10,000-60,000/μL
- PMN %
- over 75%
- Discriminating feature
- Young, sexually active; migratory; tenosynovitis/pustular rash; culture often negative
- Key action
- IV ceftriaxone; screen for STI
- Typical synovial WBC
- 2,000-100,000/μL
- PMN %
- 70-95%
- Discriminating feature
- Needle crystals, negative birefringence (intracellular)
- Key action
- NSAID/colchicine/steroid; urate-lowering later
- Typical synovial WBC
- 2,000-100,000/μL
- PMN %
- 70-95%
- Discriminating feature
- Rhomboid crystals, positive birefringence; chondrocalcinosis on X-ray
- Key action
- Treat acute attack; seek metabolic cause
- Typical synovial WBC
- 2,000-50,000/μL
- PMN %
- over 50%
- Discriminating feature
- Symmetrical polyarthritis; RF/anti-CCP; low complement
- Key action
- DMARD/biologic; rheumatology referral
- Typical synovial WBC
- 200-2,000/μL
- PMN %
- under 25%
- Discriminating feature
- High viscosity; cartilage debris; no crystals/organisms
- Key action
- Analgesia, load management
- Typical synovial WBC
- Bloody/xanthochromic
- PMN %
- Variable
- Discriminating feature
- Trauma, anticoagulation, haemophilia, PVNS
- Key action
- Treat cause; exclude fracture
Up to 5% of septic joints contain crystals concurrently. If the clinical picture is septic (fever, rapid onset, raised CRP, immunosuppression), treat as infection regardless of crystal findings until cultures are back.
Management Algorithm
Clinical Relevance
Understanding synovial biology directly informs everyday orthopaedic decision-making:
- Septic arthritis is a surgical emergency: bacterial and neutrophil proteases degrade the collagen-proteoglycan matrix within hours, so prompt arthrocentesis, washout and antibiotics preserve cartilage. The synovial WBC count and PMN percentage are the most powerful early laboratory discriminators.
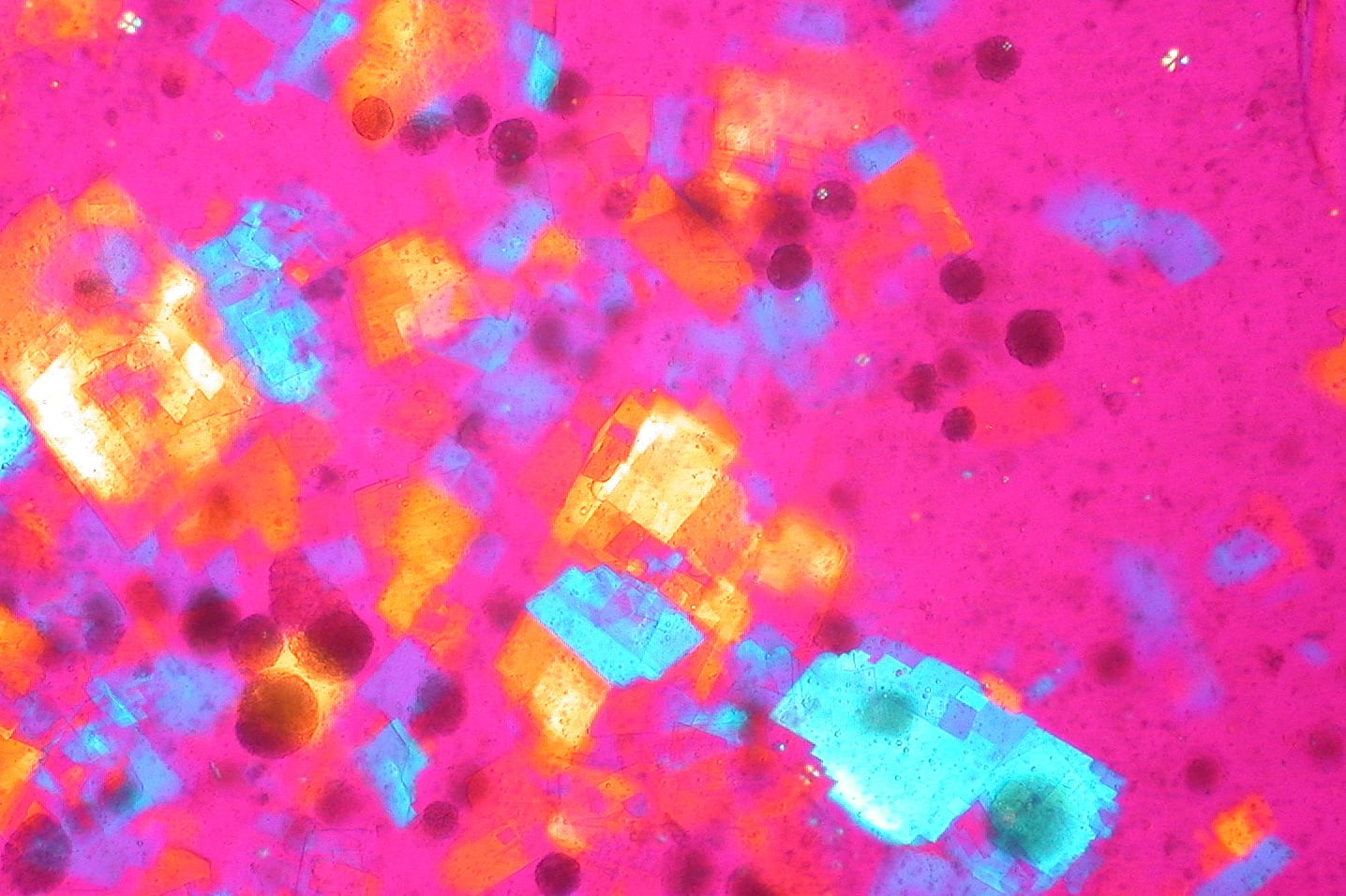
- Crystal arthropathy (gout, CPPD) is diagnosed definitively by polarised-light crystal identification in synovial fluid - and can coexist with infection.
- Osteoarthritis and inflammatory arthritis both degrade hyaluronan (reducing molecular weight and concentration) and lubricin, impairing both fluid-film and boundary lubrication and accelerating wear.
- Pannus in rheumatoid arthritis arises from fibroblast-like (Type B) synoviocyte hyperplasia and macrophage-driven cytokine release, eroding cartilage and bone; this stromal biology is now a therapeutic target (e.g. cadherin-11).
- Lubricin (PRG4) is so central that its genetic loss alone (CACP syndrome) causes precocious, non-inflammatory joint failure - human proof of its protective role and a rationale for PRG4-based therapeutics.
Guidelines, Registries & Global Practice
Global Epidemiology
Septic arthritis has a global incidence of roughly 4-10 per 100,000 person-years, rising to 30-70 per 100,000 in patients with rheumatoid arthritis or a prosthetic joint. Staphylococcus aureus is the leading pathogen worldwide; in regions with high HIV/TB prevalence, tuberculous and atypical joint infection are proportionally more common. Crystal arthropathy is rising globally: gout now affects 1-4% of adults in high-income countries (driven by ageing, obesity and metabolic syndrome), with the highest prevalence reported in Oceania. Osteoarthritis with secondary synovitis is the commonest cause of chronic joint effusion across all regions.
Side-by-Side Guidance
- Scope
- Acute native-joint sepsis
- Key recommendation
- Aspirate BEFORE antibiotics; send urgent microscopy, Gram stain, culture and crystals; treat empirically if sepsis suspected
- Evidence basis
- National guideline, expert consensus + evidence review
- Scope
- Crystal arthropathy
- Key recommendation
- Synovial fluid crystal identification by polarised microscopy is the diagnostic gold standard; always exclude co-existing sepsis
- Evidence basis
- Systematic review + consensus (varied levels)
- Scope
- Prosthetic joint infection
- Key recommendation
- Synovial WBC, PMN%, leucocyte esterase and alpha-defensin form a multi-test diagnostic algorithm (MSIS/EBJIS criteria)
- Evidence basis
- Evidence-based, mixed strength
- Scope
- Osteoarthritis
- Key recommendation
- Conditional recommendation AGAINST intra-articular hyaluronan (viscosupplementation) for knee/hip OA owing to small, uncertain benefit
- Evidence basis
- Strong/conditional GRADE recommendations
- Scope
- Osteoarthritis
- Key recommendation
- Do NOT offer intra-articular hyaluronan; intra-articular corticosteroid only for short-term relief
- Evidence basis
- GRADE evidence review
Practice Variation and Registry Evidence
Viscosupplementation illustrates marked global practice variation: despite a clear biological rationale (Balazs & Denlinger, above), large meta-analyses found only small symptomatic benefit, leading AAOS, ACR and NICE to recommend against routine intra-articular hyaluronan for knee/hip osteoarthritis, while it remains widely used in parts of Europe and Asia. For prosthetic joint infection, synovial fluid criteria are codified differently by the Musculoskeletal Infection Society (MSIS), the European Bone and Joint Infection Society (EBJIS) and AAOS, producing variation in reported infection rates across national arthroplasty registries. National joint registries (e.g. the Australian AOANJRR, the UK National Joint Registry, and Scandinavian registries) track revision for infection as a key outcome, and consistently identify deep infection as a leading cause of early revision after hip and knee arthroplasty.
Across the UK (BSR/BOA), European and US guidance, the consistent principle for a hot swollen native joint is to aspirate and culture the joint BEFORE starting antibiotics wherever feasible, because a single dose of antibiotic can render the culture falsely negative and obscure the diagnosis.
Basic Science Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the structure of the synovium. What are the two types of synoviocytes and what are their functions?”
“Explain the mechanisms of joint lubrication. How do boundary lubrication and fluid film lubrication differ?”
“You aspirate synovial fluid from an acutely swollen knee. Describe how you would analyze the fluid and interpret the results.”
Synovium Structure
- Intima: 1-3 cell layers thick (20-40 μm), NO basement membrane (unique feature for diffusion)
- Subintima: vascular connective tissue (fibrous, areolar, or adipose types)
- Type A synoviocyte: macrophage-like (CD68+), phagocytosis, 20-30% of intimal cells
- Type B synoviocyte: fibroblast-like (vimentin+), synthesize HA and lubricin, 70-80% of intimal cells
Synovial Fluid Normal Composition
- Volume: 0.3-3.5 mL in knee joint
- Appearance: clear, pale yellow, transparent, highly viscous
- WBC count: under 200/μL (under 25% neutrophils)
- Hyaluronic acid: 3-4 mg/mL, 3-4 MDa molecular weight (provides viscosity)
- Lubricin (PRG4): 50-400 μg/mL (boundary lubrication)
- Protein: 1-2 g/dL (one-third of plasma)
Hyaluronic Acid
- Glycosaminoglycan (NOT proteoglycan - no protein core)
- Repeating disaccharides: D-glucuronic acid + N-acetyl-D-glucosamine
- MW: 3-4 million Daltons (3-4 MDa) in normal SF
- Non-Newtonian viscosity: high at low shear (shock absorption), low at high shear (ease of movement)
- Synthesized by Type B synoviocytes (HAS1/2/3 enzymes)
- Degraded in arthritis (lower MW and concentration) - impairs fluid film lubrication
Lubrication Mechanisms
- Boundary lubrication: lubricin (PRG4) adsorbed to cartilage, active at low speed/high load, coefficient 0.01-0.02
- Fluid film lubrication: pressurized SF separates surfaces, active at high speed, coefficient 0.001-0.005
- Lubricin: 227 kDa glycoprotein, central mucin domain (hydrated brush), prevents solid-solid contact
- PRG4 deficiency: CACP syndrome (camptodactyly-arthropathy-coxa vara-pericarditis)
- Hydrodynamic: wedge film from sliding motion; Squeeze film: viscous resistance to rapid loading
Synovial Fluid Analysis
- Normal: under 200 WBC/μL, clear, viscous
- Non-inflammatory (OA): 200-2,000 WBC/μL, under 25% PMNs
- Inflammatory (RA, gout): 2,000-50,000 WBC/μL, over 50% PMNs
- Septic: over 50,000 WBC/μL, over 75% PMNs, positive culture (50-90%)
- Gout: MSU crystals (needle, negative birefringence - yellow when parallel)
- Pseudogout: CPP crystals (rhomboid, positive birefringence - blue when parallel)
- Septic markers: glucose under 50% of serum, lactate over 10 mmol/L
Key Clinical Correlations
- Septic arthritis: surgical emergency, treat if high suspicion (WBC counts overlap with inflammatory)
- Rheumatoid arthritis: pannus formation (invasive synovium), low complement (C3, C4), ragocytes
- Osteoarthritis: mild synovitis, HA degradation over time, cartilage fragments in SF
- Viscosupplementation: exogenous HA injection to restore fluid film lubrication in OA
- TB arthritis: lymphocyte predominance (not PMNs), culture on Lowenstein-Jensen (6-8 weeks)
Evidence Base
Viscosupplementation: Hyaluronan and Synovial Fluid Rheology
- Defined viscosupplementation: restoring the rheological homeostasis of the osteoarthritic joint by replacing degraded endogenous hyaluronan
- Normal synovial fluid is an elastoviscous solution; its high-molecular-weight hyaluronan confers shear-dependent (non-Newtonian) viscosity
- In osteoarthritis the molecular weight and concentration of hyaluronan fall, reducing elastoviscosity and impairing normal joint function
- Intra-articular high-MW hyaluronan augments the depleted fluid compartment to restore lubrication and shock absorption
Lubricin Deficiency Couples Friction to Cartilage Wear In Vivo
- Synovial fluid from humans with genetic lubricin (PRG4) deficiency failed to reduce friction in the boundary mode
- Knee joints of lubricin-null (Prg4-/-) mice showed higher friction and early cartilage wear versus wild-type controls
- Atomic force microscopy showed lubricin self-organises at the surface and reduces the work of adhesion between asperities
- Demonstrated that boundary friction is directly coupled to cartilage surface wear in vivo