Posterior Tibial Nerve Compression | Flexor Retinaculum | Medial Ankle
Severity Classification
Critical Must-Knows
- Posterior Tibial Nerve Branches: Medial plantar (abductor hallucis), lateral plantar (intrinsics), medial calcaneal (heel sensation)
- Tinel Sign: Most reliable clinical test - tap posterior to medial malleolus
- Space-Occupying Lesions: 20-30% have identifiable cause (ganglion, lipoma, varicosities)
- Double Crush: Exclude proximal nerve compression (L4-S2 radiculopathy)
- Surgical Release: Must decompress entire tunnel including abductor hallucis fascia
Clinical Pearls
- "Burning plantar pain worse at night = classic presentation
- "Always examine for intrinsic muscle weakness (toe spread)
- "MRI before surgery to identify space-occupying lesions
- "Incomplete release = recurrence - extend distally through abductor tunnel
Clinical Imaging
Imaging Gallery

Critical TTS Exam Points
Anatomical Course
Posterior tibial nerve posterior to medial malleolus. Passes beneath flexor retinaculum with posterior tibial artery and tendons (Tom, Dick, And Very Nervous Harry).
Branch Sequence
Medial calcaneal first, then bifurcation. Medial plantar (larger, sensory dominant), lateral plantar (motor dominant). All may be affected.
Examination
Tinel most reliable. Dorsiflexion-eversion stress test positive in 80%. Check intrinsic muscle power and sensation.
Surgical Pearls
Complete release essential. Must decompress flexor retinaculum AND abductor hallucis origin. Identify and protect all branches.
Quick Decision Guide
| Presentation | Investigations | Treatment | Key Pearl |
|---|---|---|---|
| Intermittent burning, positive Tinel | NCS baseline | Orthotics, activity modification | Trial 3 months conservative treatment |
| Constant symptoms, sensory loss | MRI to exclude lesion | Corticosteroid injection trial | Injection confirms diagnosis if relief |
| Motor weakness, intrinsic wasting | Urgent MRI and NCS | Surgical decompression | Complete release including distally |
TOM, DICK And Very Nervous HARRYTarsal Tunnel Contents
| T | Tibialis Posterior Most anterior |
| D | Flexor Digitorum Longus FDL tendon |
| A | Artery (PT) Posterior tibial artery |
| V | Vein Posterior tibial vein |
| N | Nerve Posterior tibial nerve |
| H | Flexor Hallucis Longus Most posterior |
| T | Tibialis Posterior Most anterior | A | Artery (PT) Posterior tibial artery | N | Nerve Posterior tibial nerve |
| D | Flexor Digitorum Longus FDL tendon | V | Vein Posterior tibial vein | H | Flexor Hallucis Longus Most posterior |
Hook:Anterior to posterior order - Tom, Dick And Very Nervous Harry. The NERVE is vulnerable between the vessels and FHL!
MLCPTN Terminal Branches
| M | Medial Plantar Larger branch, sensory to medial 3.5 toes, motor to abductor hallucis |
| L | Lateral Plantar Motor dominant, supplies intrinsics, sensory to lateral 1.5 toes |
| C | Calcaneal (Medial) Sensory to medial heel, first to branch proximally |
| M | Medial Plantar Larger branch, sensory to medial 3.5 toes, motor to abductor hallucis |
| L | Lateral Plantar Motor dominant, supplies intrinsics, sensory to lateral 1.5 toes |
| C | Calcaneal (Medial) Sensory to medial heel, first to branch proximally |
Hook:MLC = Medial, Lateral, Calcaneal - the three branches you must identify and decompress!
SPACECauses of Tarsal Tunnel Syndrome
| S | Space-occupying lesion Ganglion, lipoma, neurilemoma |
| P | Post-traumatic Fractures, dislocations, scarring |
| A | Anatomical variants Accessory muscles, bony prominences |
| C | Compression Varicosities, tenosynovitis |
| E | External factors Tight footwear, prolonged standing |
| S | Space-occupying lesion Ganglion, lipoma, neurilemoma | C | Compression Varicosities, tenosynovitis |
| P | Post-traumatic Fractures, dislocations, scarring | E | External factors Tight footwear, prolonged standing |
| A | Anatomical variants Accessory muscles, bony prominences |
Hook:SPACE = Something is taking up SPACE in the tunnel! Look for mass lesions.
Overview and Epidemiology
Why TTS Matters
TTS is the lower limb analogue of carpal tunnel syndrome but is much less common. Understanding the anatomy and terminal branches is essential for exam and surgical planning.
Tarsal Tunnel Syndrome is compression of the posterior tibial nerve or its terminal branches beneath the flexor retinaculum on the medial aspect of the ankle.
Demographics
- Female predominance: 2:1 ratio
- Peak age: 40-60 years
- Bilateral: 25% of cases
- Associated conditions: Pes planus, diabetes, RA
Less common than carpal tunnel syndrome but important to recognise.
Risk Factors
- Trauma: Ankle fractures, sprains (most common)
- Pes planus: Increased nerve tension
- Space-occupying lesions: Ganglion, lipoma
- Systemic: Diabetes, hypothyroidism, RA
20-30% have identifiable mass lesion causing compression.
Anatomy and Pathophysiology
Tarsal Tunnel Anatomy
The tarsal tunnel is a fibro-osseous tunnel on the medial ankle. The ROOF is the flexor retinaculum (laciniate ligament) extending from medial malleolus to calcaneus. The FLOOR is the medial talus, sustentaculum tali, and medial calcaneus.
Tarsal Tunnel Boundaries:
- Roof: Flexor retinaculum (laciniate ligament)
- Floor: Medial surface of talus, sustentaculum tali, medial calcaneus
- Anterior: Medial malleolus
- Posterior: Medial calcaneal tuberosity
Contents (Anterior to Posterior - Tom, Dick And Very Nervous Harry):
- Tibialis posterior tendon
- Flexor digitorum longus tendon
- Posterior tibial artery and veins
- Posterior tibial nerve
- Flexor hallucis longus tendon
Posterior Tibial Nerve Branches:
- Medial calcaneal nerve: First branch, sensory to medial heel
- Medial plantar nerve: Larger terminal branch, sensory to medial 3.5 toes, motor to abductor hallucis, FHB, FDB, first lumbrical
- Lateral plantar nerve: Smaller terminal branch, motor to intrinsics, sensory to lateral 1.5 toes
Pathophysiology:
- Increased pressure within the tarsal tunnel (greater than 30 mmHg)
- Venous congestion and nerve ischaemia
- Demyelination (reversible in early stages)
- Axonal damage (irreversible - motor weakness, atrophy)
- Fibrosis and adhesions (chronic cases)
Aetiology and Classification
Aetiological Classification
| Category | Examples | Frequency |
|---|---|---|
| Post-traumatic | Ankle fractures, sprains, dislocation | Most common |
| Space-occupying lesions | Ganglion, lipoma, neurilemoma, varicosities | 20-30% |
| Biomechanical | Pes planus, hindfoot valgus, tarsal coalition | Common |
| Systemic | Diabetes, hypothyroidism, RA, amyloidosis | Variable |
| Idiopathic | No identifiable cause | 30-40% |
Always investigate for underlying cause - MRI before surgery.
Clinical Assessment
History
- Burning pain: Plantar foot and toes
- Nocturnal symptoms: Worse at night, wake from sleep
- Aggravating factors: Prolonged standing, walking
- Radiation: Along medial arch to toes
- Associated: Weakness of toe flexion
Burning plantar pain worse at night is virtually diagnostic.
Examination
- Tinel sign: Tap posterior to medial malleolus
- Dorsiflexion-eversion test: Positive in 80%
- Two-point discrimination: Greater than 6mm abnormal
- Intrinsic muscle testing: Toe spread, FHB power
- Hindfoot alignment: Check for pes planus
Always compare to contralateral side.
Provocative Tests:
Clinical Tests for TTS
| Test | Technique | Sensitivity | Specificity |
|---|---|---|---|
| Tinel sign | Tap posterior to medial malleolus | 58% | 92% |
| Dorsiflexion-eversion | Hold 30 seconds, reproduces symptoms | 81% | 85% |
| Direct compression | 30 seconds over tunnel | 50% | 90% |
| Triple compression | DF + eversion + compression | 85% | 88% |
Differential Diagnosis
Consider: Plantar fasciitis (different location), Morton neuroma (forefoot), L5-S1 radiculopathy (check back), peripheral neuropathy (bilateral, diabetics), Baxter neuropathy (first branch LPN).
Investigations
Nerve Conduction Studies
Gold standard for confirmation but false negative rate 30-50%.
| Parameter | Normal | Abnormal |
|---|---|---|
| Medial plantar DML | Less than 4.4 ms | Greater than 4.4 ms |
| Lateral plantar DML | Less than 4.6 ms | Greater than 4.6 ms |
| SNAP amplitude | Greater than 5 mcV | Reduced or absent |
EMG findings in motor involvement:
- Fibrillation potentials in intrinsics
- Positive sharp waves
- Reduced recruitment
NCS may be normal in 30-50% of clinical TTS.
Management
Non-Operative Management
First-line treatment for 3-6 months.
Activity Modification:
- Avoid prolonged standing
- Limit high-impact activities
- Comfortable, supportive footwear
Orthotics:
- Medial arch support for pes planus
- Heel cushioning
- Custom orthotics if required
Medications:
- NSAIDs for pain relief
- Gabapentin for neuropathic pain
- Topical capsaicin
Physical Therapy:
- Nerve gliding exercises
- Stretching programme
- Strengthening
Success rate 40-50% with conservative treatment.
Surgical Technique
Complete Tarsal Tunnel Release
Indications:
- Failed conservative treatment (3-6 months)
- Space-occupying lesion
- Progressive motor deficit
- Intractable symptoms
Patient Positioning:
- Supine with leg externally rotated
- Thigh tourniquet
- Foot at end of table
Incision:
- Curvilinear incision posterior to medial malleolus
- Extend distally along abductor hallucis
- Length 6-8 cm for adequate exposure
Superficial Dissection:
- Identify and protect posterior tibial vessels
- Incise flexor retinaculum completely
- Identify main PTN trunk
Deep Dissection:
- Trace nerve proximally and distally
- Identify and release all three branches
- Release medial calcaneal nerve
- Continue release through abductor hallucis tunnel
- Excise any mass lesions
Closure:
- Leave retinaculum open
- Close subcutaneous tissue and skin
- Bulky dressing
Critical Points:
- Must release distally through abductor tunnel
- Identify and protect all branches
- Excise mass lesions completely
- Neurolysis if fibrosis present
These principles ensure complete decompression and optimal outcomes.
Complications
Surgical Complications
- Recurrence: 10-20% (incomplete release)
- Wound complications: Delayed healing, infection
- Nerve injury: Damage to branches
- Scar tethering: Nerve adhesions
- Persistent symptoms: Incomplete decompression
Most complications from inadequate release.
Prevention
- Complete release: Include abductor tunnel
- Meticulous technique: Identify all branches
- MRI preoperatively: Plan for mass lesions
- Gentle handling: Minimise nerve trauma
- Early mobilisation: Reduce adhesions
Attention to detail prevents recurrence.
Postoperative Problems
| Complication | Incidence | Prevention | Management |
|---|---|---|---|
| Incomplete release | 10-20% | Full exposure distally | Revision surgery |
| Wound dehiscence | 5% | Careful closure, offload | Wound care, possible grafting |
| Persistent symptoms | 15-30% | Proper patient selection | NCS, consider revision |
| CRPS | 2-5% | Early mobilisation | Pain management, therapy |
Postoperative Care and Rehabilitation
Immediate Postoperative:
- Bulky dressing and posterior splint
- Elevation above heart level
- Non-weight bearing 2 weeks
Weeks 0-2:
- Rest, ice, elevation
- Ankle pumps
- Wound check at 2 weeks
Weeks 2-6:
- Transition to weight-bearing as tolerated
- Gentle range of motion
- Scar massage once healed
Weeks 6-12:
- Progressive strengthening
- Return to normal footwear
- Gradual return to activity
Expected Recovery:
- Burning pain relief: 2-4 weeks
- Sensory improvement: 3-6 months
- Motor recovery: 6-12 months (if present)
- Full recovery: 6-12 months
Outcomes and Prognosis
Prognostic Factors:
Predictors of Outcome
| Good Prognosis | Poor Prognosis |
|---|---|
| Identifiable cause (mass lesion) | Idiopathic TTS |
| Short duration of symptoms | Chronic symptoms over 12 months |
| Positive response to injection | Failed injection |
| Sensory symptoms only | Motor deficit present |
| Normal EMG | Denervation on EMG |
Evidence Base
Surgical Release Outcomes (Objective vs Subjective)
- 60 patients (68 feet) undergoing tarsal tunnel release; all had positive Tinel sign and abnormal motor nerve conduction
- 85% complete symptom relief by objective assessment, but only 51% by subjective patient-reported assessment
- Significant improvement in work quality, productivity and interpersonal relationships
- Highlights a dichotomy between objective and patient-perceived outcomes - counsel realistically
Anatomic Pain Scale & Predictors of Non-operative Failure
- Prospective evaluation of 46 patients (56 feet) treated non-operatively or surgically
- Surgery improved medial calcaneal and medial plantar - but not lateral plantar - nerve region pain
- Predictors of failed conservative treatment: longer motor nerve conduction latency and more foot comorbidities
- Anatomic pain mapping aids pre- and post-treatment assessment
Electrodiagnostic Testing in TTS (AANEM Evidence-Based Review)
- Systematic review of 317 articles; only 4 met methodological criteria, all Class III evidence
- Sensory NCS more often abnormal than motor NCS, but true sensitivity and specificity could not be determined
- NCS may help confirm tibial neuropathy at the ankle (Level C recommendation)
- Diagnosis remains primarily clinical; well-designed studies still needed
Dorsiflexion-Eversion Provocative Test
- Test described in 50 normal volunteers (100 feet) and 37 patients (44 feet) treated operatively
- Maximal ankle dorsiflexion + eversion + MTPJ dorsiflexion held 5-10 s stretches and compresses the nerve beneath the laciniate ligament
- Reproduced or intensified symptoms in the large majority of affected feet; induced no symptoms in any normal foot
- Symptoms abolished post-release (mean 2.9 months) except in calcaneal fracture-related cases
Variable Tibial Nerve Branching in the Tarsal Tunnel
- Gross anatomical study of 20 cadaveric lower limbs using the malleolar-calcaneal axis as reference
- Bifurcation proximal to the axis (within/above the tunnel) in 55%, at the axis in 30%, distal in 15%
- High and variable bifurcation means branches must be sought across the whole tunnel at surgery
- Knowledge of branching reduces risk of incomplete release and iatrogenic nerve injury
Narrative Review of Diagnosis and Management
- Narrative review identifying 88 relevant articles across multiple databases
- TTS is rare and frequently under-diagnosed; the optimal stage for conservative vs surgical care remains unclear
- Limited high-level evidence exists to guide management; no robust RCTs available
- Calls for a structured, step-wise, evidence-based treatment pathway
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
A 45-year-old woman presents with burning pain in the sole of her foot
"How would you assess this patient?"
NCS shows prolonged distal latency. MRI shows a ganglion in the tarsal tunnel
"What is your management plan?"
Patient presents 6 months post tarsal tunnel release with recurrent symptoms
"How would you approach this?"
MCQ Practice Points
Anatomy Question
Q: What is the order of structures in the tarsal tunnel from anterior to posterior? A: Tom, Dick And Very Nervous Harry - Tibialis posterior, Flexor Digitorum longus, Artery (posterior tibial), Vein, Nerve (posterior tibial), Flexor Hallucis longus. The posterior tibial nerve lies between the vessels anteriorly and FHL posteriorly.
Clinical Test
Q: A patient has burning pain in the plantar foot. Which test is most sensitive for tarsal tunnel syndrome? A: Dorsiflexion-eversion stress test has highest sensitivity (81%) and specificity (85%). Hold position for 30 seconds to reproduce symptoms. Tinel sign is more specific (92%) but less sensitive (58%).
Surgical Technique
Q: What is the most common cause of recurrence after tarsal tunnel release? A: Incomplete release, particularly failure to decompress distally through the abductor hallucis tunnel. Complete release must include the flexor retinaculum proximally and extend through the abductor hallucis fascia distally to fully decompress the medial and lateral plantar nerves.
Prognostic Factor
Q: Which patient with tarsal tunnel syndrome is most likely to have a good surgical outcome? A: Patient with space-occupying lesion (ganglion, lipoma) has approximately 90% success rate. Idiopathic cases have only 50% success. Other good prognostic factors include short duration of symptoms, sensory only symptoms, and positive response to diagnostic injection.
Nerve Branches
Q: Which branch of the posterior tibial nerve branches first within the tarsal tunnel? A: Medial calcaneal nerve branches first (proximal in the tunnel), providing sensory innervation to the medial heel. The nerve then bifurcates into medial plantar (larger, sensory dominant) and lateral plantar (motor dominant) branches more distally.
Controversies and Areas of Uncertainty
Where the Evidence Is Weak
TTS is a high-yield viva topic precisely because much of its management rests on low-level evidence. Be ready to defend a position while acknowledging the uncertainty.
Is It Over- or Under-diagnosed?
No accepted diagnostic gold standard exists. Clinical criteria, provocative tests and electrodiagnostics each have limitations, and there is no validated case definition - so the same foot may be labelled TTS by one clinician and plantar heel pain or polyneuropathy by another.
Role of Electrodiagnostics
True sensitivity/specificity of NCS could not be determined in the AANEM review, and a normal study does not exclude TTS. Some surgeons require electrodiagnostic confirmation before release; others operate on a strong clinical picture plus imaging.
Endoscopic vs Open Release
Endoscopic release offers smaller incisions but cannot address mass lesions and risks incomplete decompression. There are no high-quality randomised comparisons; open complete release remains the reference standard, especially when a space-occupying lesion is present.
Idiopathic TTS
Outcomes are substantially worse without an identifiable cause. Whether truly idiopathic cases benefit from surgery at all is debated, and many advocate exhausting conservative options and confirming with diagnostic injection first.
Guidelines, Registries & Global Practice
There are no dedicated national-society clinical practice guidelines specific to tarsal tunnel syndrome from the major bodies, reflecting its rarity and the limited high-level evidence. Practice is instead shaped by foot-and-ankle society consensus, electrodiagnostic practice parameters and surgical experience, and is broadly consistent worldwide.
Evidence and Guidance, Side by Side
| Source | Region | Position |
|---|---|---|
| AANEM practice parameter (Patel 2005) | International / US | NCS may confirm tibial neuropathy at the ankle (Level C); diagnosis remains clinical |
| AAOS / AOFAS expert consensus | US | Stepwise care - conservative first, image to exclude mass lesion, release for refractory or compressive cases |
| BOA / BOFAS practice (UK) | UK | Similar stepwise pathway; MRI and electrodiagnostics used selectively before surgery |
| EFORT / European foot-ankle societies | Europe | Emphasise excluding differentials (polyneuropathy, radiculopathy) and identifying a structural cause |
| McSweeney & Cichero narrative review | International | No robust evidence base; calls for a structured, step-wise approach and RCTs |
Global epidemiology and practice variation:
- TTS is uncommon and consistently under-recognised; precise population incidence is unknown across all regions.
- No arthroplasty/implant-style registries track TTS, as treatment is soft-tissue decompression rather than implantation.
- High-resource settings: routine pre-operative MRI and electrodiagnostics, ultrasound-guided diagnostic injection, and access to microsurgical neurolysis.
- Limited-resource settings: diagnosis is predominantly clinical with provocative tests; MRI and nerve conduction studies may be unavailable, so identifiable causes (post-traumatic deformity, large masses) are prioritised for surgery.
- Across all settings the surgical principle is identical: complete release of the flexor retinaculum, decompression of all branches, distal release through the abductor hallucis fascia, and excision of any space-occupying lesion.
Tarsal Tunnel Syndrome Exam Cheat Sheet
Clinical summary
Anatomy
- •Tom, Dick And Very Nervous Harry = contents anterior to posterior
- •Three terminal branches: medial calcaneal (first), medial plantar, lateral plantar
- •Flexor retinaculum = roof; medial talus, sustentaculum tali and medial calcaneus = floor
Clinical Features
- •Burning plantar pain worse at night
- •Tinel positive posterior to medial malleolus
- •Dorsiflexion-eversion test most sensitive
- •Intrinsic weakness = advanced disease
Investigations
- •NCS: prolonged distal motor latency (less than 4.4ms MPN)
- •MRI: essential to identify mass lesions (20-30% have one)
- •NCS false negative rate 30-50%
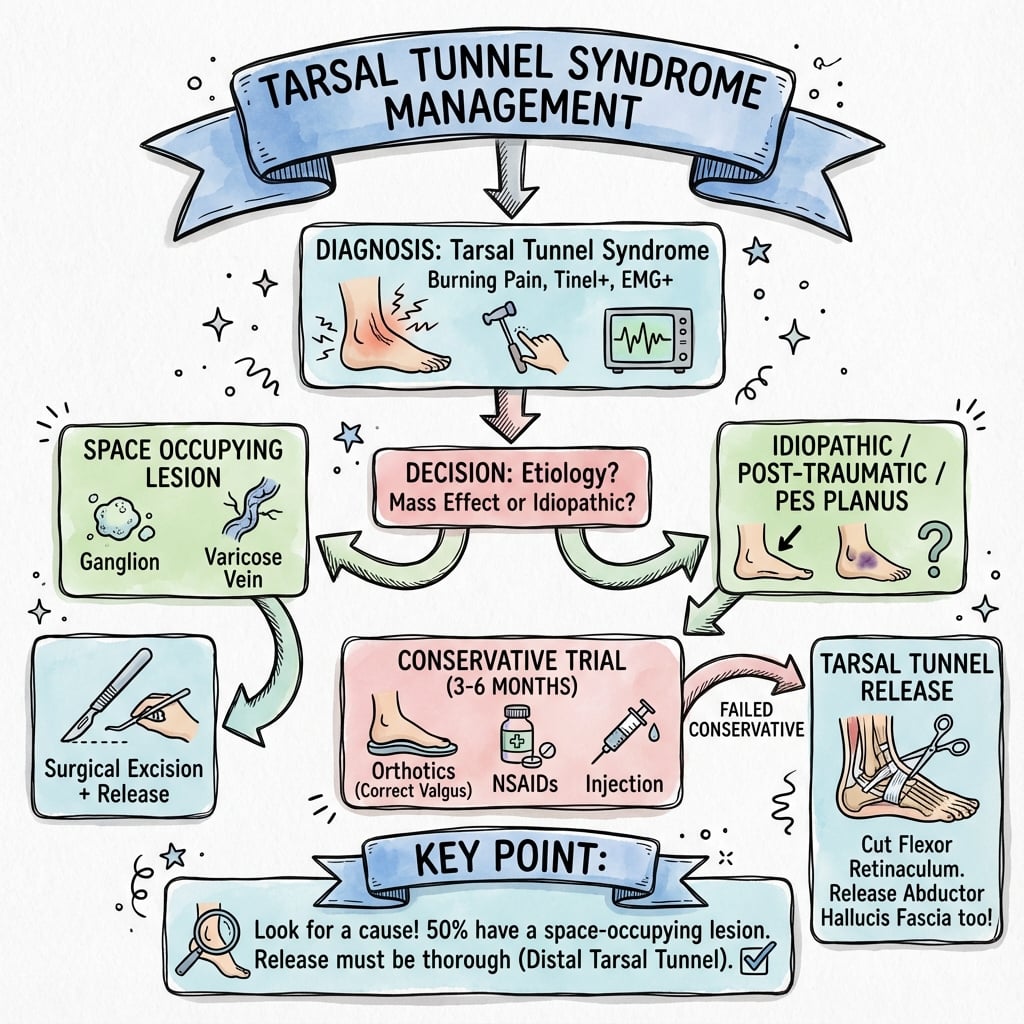
Treatment Algorithm
- •Conservative 3-6 months: orthotics, activity modification, medications
- •Injection: diagnostic and therapeutic, 50-60% temporary relief
- •Surgery if failed conservative or progressive motor deficit
Surgical Pearls
- •Curvilinear incision posterior to medial malleolus
- •Complete release of flexor retinaculum
- •MUST extend through abductor hallucis tunnel distally
- •Identify and protect all three branches
Outcomes
- •60-85% overall success
- •90% success with mass lesion
- •50% success idiopathic
- •Recurrence 10-20% (incomplete release)