Wrist Extension Loss | Thumb Extension Deficit | Finger MCP Extension Failure
- Radial nerve palsy = loss of wrist extension, thumb extension, finger MCP extension
- Posterior interosseous nerve (PIN) palsy spares ECRL (wrist extension intact)
- PT to ECRB restores wrist extension (most important transfer)
- PL to EPL restores thumb IP extension (enables key pinch)
- Tendon transfers require M4 donor strength, full passive ROM, healed soft tissues
- “Radial nerve high injuries spare ECRL (innervated proximal to spiral groove)
- “Standard transfer set: PT→ECRB, PL→EPL, FCR→EDC (Brand transfers)
- “Never harvest ECRL as donor - it is vascularized by radial artery perforators
- “Postoperative splinting: wrist 45° extension, MCP 0° extension, IP flexion
Radial nerve innervates all wrist/finger extensors. Injury at spiral groove (mid-humerus) causes complete palsy. Injury distal to supinator (PIN palsy) spares ECRL - wrist extension maintained but weak thumb/finger extension.
Wait 3-6 months for nerve recovery before tendon transfer. If no recovery by 6 months, proceed with surgery. EMG at 3 months guides decision. Never delay beyond 12 months - muscle fibrosis occurs.
One donor = one function. Donor must have M4 strength, expendable function, similar excursion. Synergistic transfers (flexor→extensor) require retraining but work well. PT to ECRB is most critical transfer.
6 weeks immobilization in wrist 45° extension, MCP 0° extension. Then gentle active ROM with blocking splint for 6 more weeks. Full strengthening at 12 weeks. Expect 6-12 months for functional maturity.
- Nerve Level
- High radial (spiral groove)
- Treatment
- Wait 3-6 months then PT→ECRB, PL→EPL, FCR→EDC
- Key Pearl
- Always exclude fracture - Holsten fracture association
- Nerve Level
- PIN (below supinator)
- Treatment
- Wait 3-6 months then PL→EPL, FCR→EDC only
- Key Pearl
- ECRL spared - can skip PT→ECRB transfer
- Nerve Level
- Incomplete injury
- Treatment
- Conservative with dynamic splinting
- Key Pearl
- Continue observation up to 6 months
PPFStandard Tendon Transfer Set (Brand)
Hook:PPF - Primary Priority Functions restored by these three transfers!
MEDSDonor Tendon Requirements (MEDS)
Hook:MEDS - the donor tendon prescription for successful transfer!
Overview and Epidemiology
Radial nerve palsy causes devastating functional loss - inability to extend wrist, thumb, and fingers eliminates precision grip, power grip, and all hand positioning. Tendon transfers can restore 85-95% of function when nerve recovery fails. Early recognition and timely surgery (before 12 months) prevents permanent disability.
- Humerus fracture (Holstein-Lewis distal spiral groove injury)
- Saturday night palsy (compression against humerus during sleep)
- Iatrogenic (lateral approach to humerus, radial head excision)
- Penetrating trauma (stab, gunshot wounds)
- Compression neuropathy (tumor, lipoma, crutch palsy)
- Loss of wrist extension - hand drops, grip strength falls 70%
- Loss of thumb extension - cannot perform key pinch or tripod pinch
- Loss of finger MCP extension - intrinsics cannot extend digits
- Preserved intrinsic function - PIP/DIP extension via interossei/lumbricals maintained
Pathophysiology and Mechanisms
High radial nerve injury (above spiral groove): All extensors paralyzed including ECRL. Complete wrist drop. Low radial nerve injury (PIN below supinator): ECRL spared, weak wrist extension maintained but thumb/finger extension lost. Level of injury determines which transfers are needed.
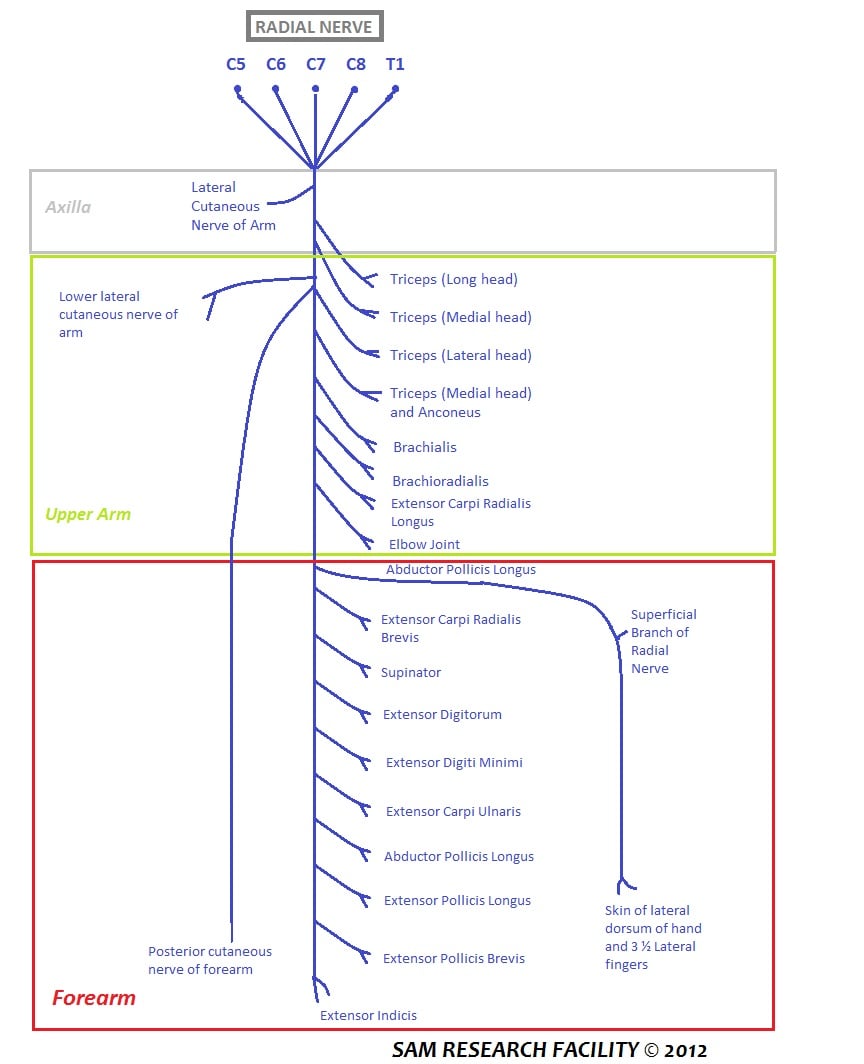
Radial Nerve Anatomy
- Branches
- To triceps, anconeus, ECRL
- Muscles Innervated
- Elbow extension, wrist extension
- Clinical Deficit
- High injury: elbow weakness + complete wrist drop
- Branches
- To brachioradialis, ECRB, ECRL
- Muscles Innervated
- Wrist extensors
- Clinical Deficit
- Classic radial nerve palsy with complete wrist drop
- Branches
- PIN to EDC, EPL, EPB, EIP, ECU
- Muscles Innervated
- Finger/thumb extensors
- Clinical Deficit
- Weak wrist extension maintained, no finger/thumb extension
Tendon Transfer Biomechanics
- Strength: Minimum M4 (good against gravity + resistance)
- Excursion: Similar amplitude to recipient (6-7cm for wrist)
- Expendable: Function can be sacrificed without deficit
- Direction: Straight line of pull or via pulley
- Full passive ROM: No joint contractures
- Healed soft tissues: No ongoing infection or edema
- Timing: 3-6 months post-injury to allow nerve recovery
- Motivation: Patient must comply with rehabilitation
Classification of Radial Nerve Palsies
Classification by Injury Level
- Injury Location
- Above spiral groove (proximal humerus)
- Deficits
- Triceps + all wrist/finger/thumb extensors
- Transfers Needed
- PT→ECRB, PL→EPL, FCR→EDC (full set)
- Injury Location
- Spiral groove (mid-humerus)
- Deficits
- Wrist + finger + thumb extensors (triceps spared)
- Transfers Needed
- PT→ECRB, PL→EPL, FCR→EDC (full set)
- Injury Location
- Below supinator (proximal forearm)
- Deficits
- Finger + thumb extensors (ECRL spared)
- Transfers Needed
- PL→EPL, FCR→EDC (skip PT→ECRB)
Test ECRL function: Patient extends wrist in radial deviation. If present, ECRL is intact (PIN palsy). If absent, complete radial nerve palsy. This distinction changes surgical plan - PIN palsy does not need PT→ECRB transfer.
The timing section above frames transfers as a late salvage after recovery fails - but a high-yield concept is that the wrist-extension transfer can be done EARLY, at the time of (or soon after) nerve repair, as an "internal splint" rather than waiting the full reinnervation period:
- The idea (Burkhalter): perform the pronator teres to ECRB transfer early, while awaiting radial nerve recovery. It provides immediate active wrist extension - so the patient regains a functional, grip-stabilising hand straight away and can often discard the external cock-up splint during the long wait.
- It acts as a "helper", not a burned bridge: because PT is synergistic and the transfer is to the wrist (not the fingers), it does not preclude nerve recovery - if the radial nerve reinnervates the wrist extensors, the PT transfer simply augments them; if recovery fails, it is already in place as the definitive wrist transfer.
- Why the wrist first: wrist extension is the most important single function (it powers grip via tenodesis and positions the hand), so restoring it early gives the biggest functional return during the recovery window; the finger and thumb transfers are usually still staged/decided later.
- Caveat: this is an adjunct to, not a replacement for, the recovery-monitoring pathway; the finger/thumb transfers and any nerve surgery are still timed on reinnervation.
Exam point: the PT-to-ECRB transfer can be performed early as an "internal splint" to give immediate wrist extension during the wait for nerve recovery - it is synergistic, does not block reinnervation, and becomes the definitive wrist transfer if recovery fails.
WTFFunctions Lost in Radial Nerve Palsy
Hook:WTF - the patient's reaction when they realize they can't extend their wrist, thumb, or fingers!
Clinical Assessment
- Mechanism: Fracture, compression, penetrating trauma?
- Timing: Immediate (injury) vs delayed (callus compression)
- Recovery: Any return of function? Proximal to distal progression?
- Functional impact: Grip strength, pinch strength, activities of daily living
- Previous surgery: Nerve exploration, nerve repair, grafting?
- Wrist extension: Active extension against gravity (test ECRL vs ECRB)
- Thumb extension: EPL (IP extension), EPB (MCP extension), APL (abduction)
- Finger extension: EDC (MCP extension), EIP (independent index extension)
- Passive ROM: Full at wrist, MCP, PIP, DIP (rule out contractures)
- Sensation: Dorsal first web space (superficial radial nerve)
Physical Examination Sequence
Systematic Examination
Patient extends wrist with forearm pronated. Normal = 70° extension. ECRL produces extension with radial deviation. ECRB produces straight extension. Loss of both = complete palsy. Weak extension in radial deviation only = PIN palsy (ECRL spared).
EPL test: Thumb on table, lift thumb off surface (IP extension). EPB test: Extend thumb MCP against resistance. APL test: Abduct thumb perpendicular to palm. Loss of all three = PIN involvement.
EDC test: Extend MCP joints with wrist in neutral. EIP test: Extend index finger independently with other fingers flexed. Inability to extend MCPs even with wrist flexed (tenodesis) = EDC paralysis.
PT strength: Resist foot inversion (M4 minimum required). PL presence: 15% absent - palpate tendon with wrist flexion. FCR strength: Resist wrist flexion in radial deviation. All donors must be M4 or stronger.
Differential Diagnosis of Wrist/Finger Drop
- Key clinical feature
- Complete wrist + finger + thumb extension loss, dorsal first web sensory loss
- Wrist extension
- Absent (complete wrist drop)
- Distinguishing test
- Triceps spared if below spiral groove; sensory deficit present
- Key clinical feature
- Finger/thumb extension loss, no sensory deficit
- Wrist extension
- Present but radially deviated (ECRL spared)
- Distinguishing test
- Radial-deviated wrist extension preserved; sensation intact
- Key clinical feature
- Loss of finger extension, often progressive/sequential
- Wrist extension
- Normal
- Distinguishing test
- No tenodesis effect; passive wrist flexion does not extend fingers
- Key clinical feature
- Finger can be held extended but not actively initiate extension
- Wrist extension
- Normal
- Distinguishing test
- Passive extension maintained; tendon subluxates into intermetacarpal groove
- Key clinical feature
- Multi-nerve pattern, often with proximal weakness
- Wrist extension
- Variable
- Distinguishing test
- Weakness crosses nerve territories; neck/shoulder signs, dermatomal sensory loss
- Key clinical feature
- Extensor weakness with upper motor neuron signs or inconsistency
- Wrist extension
- Variable
- Distinguishing test
- Hyperreflexia/tone, or normal tenodesis with inconsistent effort
Concurrent injuries with radial nerve palsy:
- Brachial artery injury (check pulses, capillary refill)
- Median/ulnar nerve injury (high-energy trauma)
- Compartment syndrome (forearm compartments)
- Elbow instability (terrible triad injuries) Document neurovascular status thoroughly before and after any intervention.
Investigations
Diagnostic Workup
Clinical examination is diagnostic. Loss of wrist extension, thumb extension, finger MCP extension with preserved sensation (superficial radial nerve may be intact). Check for proximal injuries (triceps weakness suggests high lesion).
AP and lateral humerus to identify fracture (Holstein-Lewis). Forearm radiographs if PIN palsy suspected (evaluate for proximal radius fracture, Monteggia injury). Document any bony pathology requiring fixation first.
EMG/NCS at 3 months post-injury to assess for reinnervation. Fibrillation potentials indicate denervation. Motor unit potentials indicate recovery. Absent motor units at 6 months = indication for tendon transfer.
MRI of arm/forearm if nerve exploration planned (identify neuroma, nerve gap, tumor). Ultrasound to confirm tendon integrity of donors (PT, PL, FCR). Not routinely required for tendon transfers.
EMG at 3 months shows denervation (fibrillation potentials). Repeat EMG at 6 months - if no motor unit potentials in radial-innervated muscles, nerve recovery unlikely. Proceed with tendon transfer surgery at this point. Do not wait beyond 12 months - muscle fibrosis reduces transfer success.
Treatment and Surgical Intervention
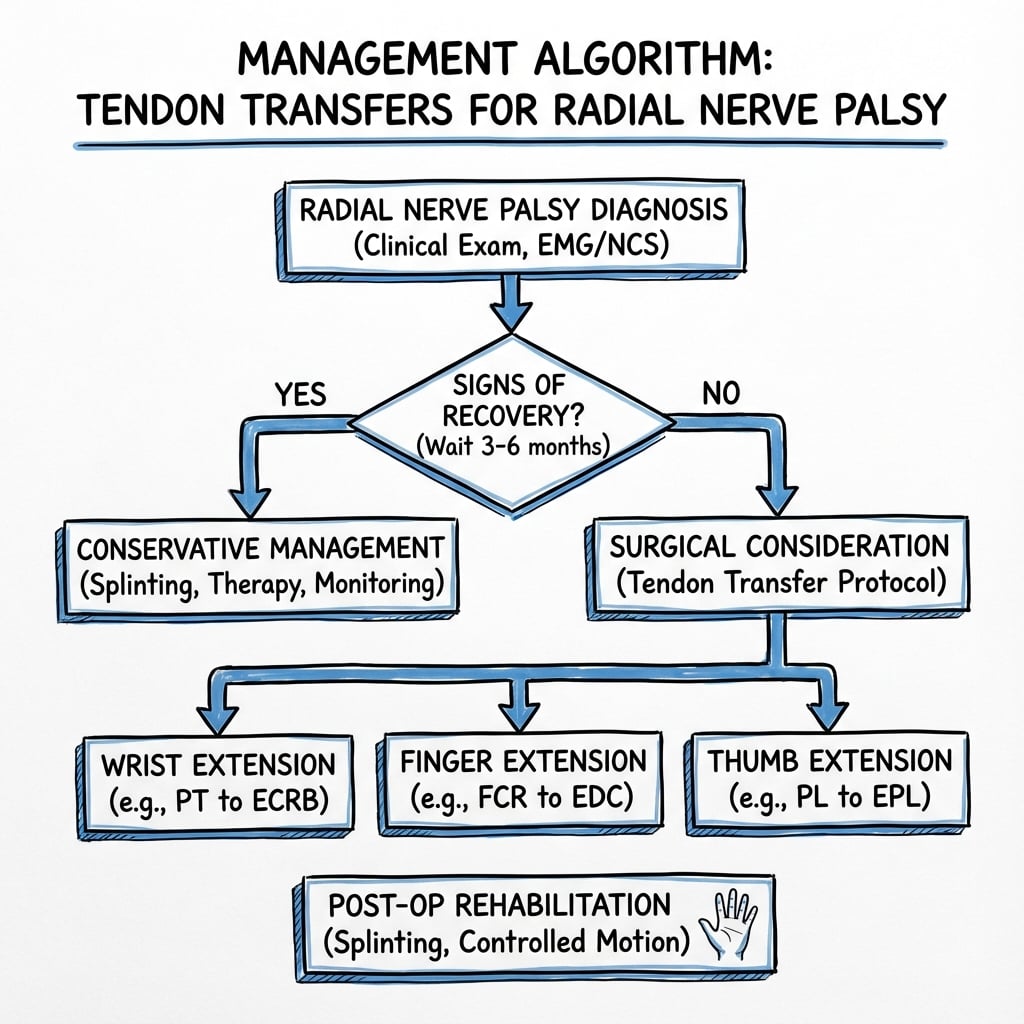
Conservative Management
Indications: All patients for first 3-6 months to allow nerve recovery.
- Wrist extension splint (cock-up splint) maintains wrist in 30-45° extension
- MCP extension outrigger prevents MCP flexion contractures
- Night splinting to maintain passive ROM
- Wear splint during day for function, remove for exercises
- Passive ROM exercises - maintain full wrist, MCP, IP motion
- Strengthening of intact muscles (finger flexors, intrinsics)
- Functional training with splint (grip, pinch activities)
- Nerve gliding exercises to prevent adhesions
Surgical Management: Tendon Transfers
Indications:
- No clinical or EMG recovery by 6 months
- Progressive nerve injury with no expectation of recovery
- Nerve gap greater than 3cm not amenable to repair
- Patient motivated for rehabilitation
Standard Three-Transfer Set
Most widely used tendon transfer combination for radial nerve palsy.
- Restores Function
- Wrist extension
- Technique
- Harvest PT insertion, weave through ECRB
- Attachment
- Wrist 45° extension, fingers relaxed
- Restores Function
- Thumb IP extension
- Technique
- Harvest PL, reroute around FCR, weave through EPL
- Attachment
- Thumb in extension and abduction
- Restores Function
- Finger MCP extension
- Technique
- Split FCR into 4 slips, attach to EDC of each finger
- Attachment
- MCP 0° extension, IP flexion
ECRL is vascularized by radial artery perforators and should never be harvested as a donor. ECRB is the recipient of choice for wrist extension. PT is the ideal donor - strong (M5), expendable (tibialis posterior maintains foot inversion), and has good excursion (7cm).
The single most-asked radial-palsy question is "what are the options?" - and the examinable framework is the three named transfer sets, which differ only in the finger-extension donor (all three use PT to ECRB for the wrist and PL/FDS to EPL for the thumb):
- Standard / "Jones" set - FCU to EDC: the historical set. The problem is that flexor carpi ulnaris is the only ulnar deviator and the key power-grip wrist stabiliser, so sacrificing it produces radial deviation and weakens the wrist for heavy grip.
- Brand set - FCR to EDC: the popular modern choice. By preserving FCU, it maintains wrist stability/ulnar deviation and avoids the radial-deviation deformity of the Jones set - the main reason FCR is preferred over FCU.
- Boyes (superficialis) set - FDS to EDC/EPL (FDS of middle to EPL+EIP, FDS of ring to EDC), routed through the interosseous membrane: gives independent finger extension at any wrist position and strong excursion, but requires an intact median nerve, more retraining, and a window in the interosseous membrane, and costs PIP flexion of the donor fingers.
Pair these with the thumb/wrist donors: PT to ECRB (wrist - never ECRL, which is radial-artery-vascularised), and PL (or FDS) to EPL (thumb).
Exam point: name the three sets by their finger donor - FCU (Jones, but causes radial deviation), FCR (Brand, preserves FCU - preferred), and FDS (Boyes, independent extension but needs median nerve) - all on a background of PT-to-ECRB and PL-to-EPL.
Surgical Technique
Surgical Approach
Multiple incisions required to access donor and recipient tendons.
Incision Planning
10cm longitudinal incision over volar forearm starting 4cm proximal to wrist crease. Identify and harvest PT tendon at insertion on navicular. Identify and harvest PL tendon (if present) at wrist. Identify and harvest FCR tendon proximal to wrist.
6cm longitudinal incision over radial aspect of distal forearm. Identify ECRB tendon insertion on base of 3rd metacarpal. Create subcutaneous tunnel from volar incision to pass PT tendon.
8cm longitudinal incision centered over 3rd metacarpal. Identify EDC tendons at musculotendinous junction. Identify EPL tendon in third dorsal compartment at Lister's tubercle.
Superficial radial nerve crosses operative field at radial forearm incision - protect branches. Radial artery lies deep to FCR - retract carefully when harvesting FCR. PIN lies deep in forearm - not usually encountered with tendon harvesting.
Complications
- Incidence
- 2-5%
- Prevention
- Adequate fixation, proper tensioning, 6-week immobilization
- Management
- Urgent re-exploration and repair if within 2 weeks, revision transfer if delayed
- Incidence
- 10-15%
- Prevention
- M4 donor strength, proper tensioning, compliant rehab
- Management
- Extended therapy, consider revision if M3 or worse at 12 months
- Incidence
- 15-20%
- Prevention
- Early IP flexion exercises, splinting between sessions
- Management
- Aggressive hand therapy, dynamic splinting, capsulotomy if persistent
- Incidence
- 5-10%
- Prevention
- Select expendable donors, preserve ECRL, counsel patient
- Management
- Usually mild - PT loss compensated by tibialis posterior, PL loss asymptomatic
- Incidence
- 3-8%
- Prevention
- Careful dissection at radial forearm, protect nerve branches
- Management
- Desensitization therapy, neuroma excision if symptomatic
- Incidence
- 5-10%
- Prevention
- Smooth tunnels, avoid sharp angles, early mobilization
- Management
- Tenolysis after 3-6 months if limiting function
Key factors for successful transfer:
- Proper donor selection - M4 strength minimum
- Correct tensioning - wrist 45° extension for PT→ECRB, MCPs 0° for FCR→EDC
- Adequate fixation - Pulvertaft weave with 3-4 passes
- Strict immobilization - 6 weeks to allow tendon healing
- Motivated patient - compliance with rehab is essential Failure to adhere to these principles results in poor outcomes.
Outcomes and Prognosis
Expected Functional Outcomes
- Preoperative
- 0° (wrist drop)
- Postoperative (12 months)
- 45-60° active extension
- Functional Gain
- Enables grip function, eliminates need for splint
- Preoperative
- 30% of normal (flexion only)
- Postoperative (12 months)
- 70-80% of normal
- Functional Gain
- Functional grip for ADLs and light work
- Preoperative
- Unable (no thumb extension)
- Postoperative (12 months)
- 80-90% of normal
- Functional Gain
- Key pinch and tripod pinch restored
- Preoperative
- 0° (drop hand)
- Postoperative (12 months)
- Full extension (0-10° hyperextension)
- Functional Gain
- Hand opening for grasp, release, fine motor
Factors predicting success:
- Surgery within 12 months of injury (before muscle fibrosis)
- Full passive ROM preoperatively
- M4 or M5 donor strength
- No concurrent nerve injuries
- Compliant with rehabilitation
- Young age and high motivation Patients meeting all criteria achieve M4-M5 transfer strength and return to previous occupation in 90% of cases.
Long-term Follow-up
- 6 weeks: Splint removed, begin active motion
- 3 months: Independent ADLs, light activities
- 6 months: Return to work (light duty)
- 12 months: Full strength maturation, final assessment
- Long-term: Function maintained indefinitely with rare deterioration
- 90% satisfied with functional outcome
- Grip strength most improved function (70-80% normal)
- Cosmesis improved (elimination of wrist drop)
- Independence in ADLs achieved
- Return to work in 85% of patients (may require job modification)
Guidelines, Registries & Global Practice
Global Epidemiology
Radial nerve palsy is the most common nerve palsy associated with long-bone fracture. In the systematic review by Shao and colleagues, the prevalence after humeral shaft fracture was 11.8% (532 palsies in 4517 fractures), with the highest association in middle and middle-distal third transverse and spiral fractures (PMID 16326879). The dominant non-traumatic cause worldwide remains compression neuropathy ("Saturday night palsy"). Because 70-88% of fracture-associated palsies recover spontaneously (PMID 16326879, 19669771), the population who ultimately require reconstruction is small, and tendon transfer is performed far more often than nerve transfer globally.
Side-by-Side Guidance Across Bodies
- Position on initial management
- Fracture-associated palsy: observe; most recover spontaneously
- Reconstruction guidance
- Tendon transfer if no recovery; nerve transfer in selected early cases
- Evidence level
- Consensus / narrative review
- Position on initial management
- Expectant management with structured nerve monitoring (clinical + NCS/EMG)
- Reconstruction guidance
- Refer to specialist hand unit if no recovery by 3 months for nerve or tendon reconstruction
- Evidence level
- Consensus / standards of care
- Position on initial management
- Closed humeral fracture with palsy: no routine acute exploration
- Reconstruction guidance
- Explore if open injury, secondary palsy after reduction, or no recovery by 3-4 months
- Evidence level
- Expert / educational
- Position on initial management
- Observation supported by Shao algorithm; baseline NCS at 6 weeks
- Reconstruction guidance
- Nerve transfer favoured if injury under ~12 months and nerve viable; tendon transfer for late palsy
- Evidence level
- Systematic review derived
There is no high-level (Level 1) guideline mandating a single pathway. All major bodies converge on: (1) expectant management of closed fracture-associated palsy because spontaneous recovery is the norm; (2) a decision checkpoint at roughly 3 months using clinical examination plus electrophysiology; and (3) tendon transfer as the durable reconstruction for established, non-recovering palsy, with nerve transfer as an emerging alternative when the injury is recent and the proximal nerve is viable (PMID 32093993, 38059217).
Registry & Pooled Evidence
There is no dedicated international radial-nerve-palsy registry; the best population-level evidence comes from pooled systematic reviews. The Shao meta-analysis (1045 patients) anchors epidemiology and spontaneous-recovery data (PMID 16326879), and the Abboud meta-analysis (21 studies, 542 patients) provides the strongest comparative outcome data: tendon transfer gives higher rates of excellent recovery (29% vs 11%) and satisfaction (89%) but more radial deviation (18% vs 0%) and an 18% revision rate compared with nerve transfer (PMID 38059217).
Practice Variation
Practice differs by injury timing, resource setting and surgeon training. High-volume hand units increasingly offer nerve transfer (AIN-to-ECRB, FCR-branch-to-PIN) for sub-12-month injuries (PMID 32093993), whereas tendon transfer remains the universal default for late or irrecoverable palsy and in settings without microsurgical capacity. Donor-tendon preference also varies: some units use FCR for finger extension while preserving FCU to avoid radial deviation (PMID 16928411), while others use a single powerful FCU transfer for simplicity (PMID 16814906).
Key documentation requirements:
- Preoperative assessment of donor strength (M4 minimum) and passive ROM (full required)
- EMG/NCS results demonstrating no nerve recovery before electing reconstruction
- Informed consent discussing 6-12 month recovery, complication rate, revision risk (~18% in pooled data) and potential for inadequate strength or radial deviation
- Postoperative compliance with immobilisation - document patient education
- Timing: Document decision-making at the 3-month checkpoint, and that reconstruction was not unduly delayed
Common litigation issues:
- Failure to monitor for spontaneous recovery and to act at the 3-month checkpoint
- Inadequate initial fixation leading to rupture
- Premature mobilisation causing transfer failure
- Failure to recognise and manage complications (rupture, stiffness, radial deviation)
MCQ Practice Points
Q: A patient with radial nerve injury at the spiral groove has preservation of which function? A: Elbow extension (triceps innervated proximal to spiral groove). Loss of wrist extension, finger extension, and thumb extension. ECRL is variable - may be spared if injury is distal in spiral groove.
Q: Why is ECRL never used as a donor tendon for transfer? A: ECRL is vascularized by radial artery perforators and harvesting it risks vascular compromise. ECRB is the appropriate recipient for wrist extension restoration via PT transfer.
Q: When is the optimal time to perform tendon transfer surgery for radial nerve palsy? A: 3-6 months post-injury if EMG shows no motor unit potentials. Do not wait beyond 12 months as muscle fibrosis reduces outcomes. 70% of patients recover spontaneously within 3-6 months.
Q: What is the appropriate wrist position when tensioning PT to ECRB transfer? A: 45 degrees of wrist extension with fingers in neutral (not flexed). Too much extension creates finger tightness. Too little extension provides inadequate wrist extension power.
Q: What is the most common cause of inadequate strength after tendon transfer? A: Incorrect tensioning (transfer too loose) or inadequate donor strength (under M4 preoperatively). Prevention: confirm M4 donor strength preop and use proper tensioning technique intraoperatively.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old carpenter presents 4 months after a distal humerus fracture treated conservatively. He has complete wrist drop, no thumb extension, and no finger MCP extension. Sensation is intact in the first web space. EMG shows fibrillation potentials in radial-innervated muscles with no motor unit potentials. How would you manage this patient?”
“You are performing PT to ECRB transfer for radial nerve palsy. Walk me through your technique for harvesting PT, creating the tunnel, and tensioning the transfer. What are the key technical points?”
“A patient returns 3 weeks after tendon transfer surgery with sudden loss of wrist extension. They were progressing well in the splint but removed it yesterday to shower and heard a 'pop' when extending the wrist. On examination, there is no active wrist extension and you can palpate a gap in the subcutaneous tissue over the radial forearm. What is your diagnosis and management?”
Key Anatomy
- Radial nerve = all wrist/finger/thumb extensors innervation
- High injury (spiral groove) = complete wrist drop + finger/thumb extension loss
- PIN injury (below supinator) = ECRL spared, weak wrist extension maintained
- ECRL = vascularized by radial artery perforators, NEVER harvest as donor
Classification and Timing
- 0-3 months = observation with dynamic splinting, 70% spontaneous recovery
- 3-6 months = EMG at 3 months, proceed to surgery if no motor units by 6 months
- Beyond 12 months = outcomes decline due to muscle fibrosis, urgent surgery needed
- High vs PIN palsy = determines if PT→ECRB transfer needed (skip in PIN)
Standard Transfer Set (Brand)
- PT → ECRB = restores wrist extension (most important)
- PL → EPL = restores thumb IP extension (enables pinch)
- FCR → EDC = restores finger MCP extension (opens hand)
- Tensioning: wrist 45° extension, MCP 0°, fingers neutral
Surgical Pearls
- Donor requirements: M4 strength, expendable function, similar excursion
- Pulvertaft weave: 3-4 passes with 3-0 nonabsorbable suture
- PL absent in 15% - use FDS ring or middle as alternative donor
- Test tension intraop: flex/extend wrist and fingers to confirm appropriate pull
Complications
- Transfer rupture: 2-5% (urgent re-exploration within 48 hours)
- Inadequate strength: 10-15% (incorrect tensioning or weak donor)
- Finger stiffness: 15-20% (aggressive IP flexion exercises to prevent)
- Superficial radial nerve injury: 3-8% (protect at radial forearm incision)
Key Evidence and Outcomes
- Success rate: 85-95% achieve M4/M5 function at 12 months
- Grip strength: 70-80% of normal, pinch strength 80-90%
- Timing critical: under 12 months = 92% success, over 12 months = 71% success
- Long-term: 90% patient satisfaction, 85% return to work (may need modification)
Evidence Base and Key Trials
Radial Nerve Palsy Associated with Humeral Shaft Fractures: Systematic Review (defining epidemiology paper)
- Systematic review: 35 eligible papers, 1045 patients with radial nerve palsy
- Overall prevalence of radial nerve palsy after humeral shaft fracture 11.8% (532 of 4517 fractures)
- Middle and middle-distal third shaft fractures, transverse and spiral patterns, carry the highest association (p less than 0.001)
- Overall recovery 88.1%; spontaneous recovery 70.7% in conservatively managed patients
- No significant difference in final outcome between early exploration and expectant management - supports initial observation
Humeral Shaft Fractures with Radial Nerve Palsy: 117 Cases and a Management Algorithm
- 117 consecutive humeral shaft fractures with radial nerve palsy over 20 years; no primary nerve exploration
- Spontaneous recovery in 95% of closed and 94% of grade 1-2 open fractures
- Onset of recovery mean 6 weeks (range 3-24); full recovery mean 17 weeks (range 3-70)
- 14 patients had no clinical/EMG recovery by 12 weeks - threshold for exploration or reconstruction
- Delayed tendon transfers (2-3 years after injury) still achieved good/excellent function
Long-term Results of Tendon Transfers in Radial and Posterior Interosseous Nerve Palsy
- 18 tendon transfers for isolated radial or PIN palsy over 21 years; 15 reviewed at mean 9.5-year follow-up
- Outcomes: 11 excellent, 2 good, 1 fair, 1 poor
- Main problems were reduced grip power and radial deviation, the latter worst after flexor carpi ulnaris to EDC transfer
- Authors' final preference: modified Tsuge - PT to wrist extensors, FCR to fingers, PL to thumb, with APL tenodesis to brachioradialis
- Preserving FCU maintained wrist stability and flexion and avoided radial deviation
Single Flexor Carpi Ulnaris Transfer for Radial Nerve Palsy
- 108 patients with isolated persisting radial nerve palsy; single FCU transferred to EDC, EIP and EPL
- Only patients with M5 FCU power were selected for the single-transfer technique
- Mean follow-up 48 months (range 3-120); finger and MCP extension comparable to the normal hand
- Wrist extension range was less than the contralateral side but all patients regained functional, work-capable hands
- No clear difference in end result versus the conventional three-tendon transfer set
Nerve Transfer versus Tendon Transfer for Radial Nerve Paralysis (direct comparison)
- 14 patients had AIN-to-ECRB and FCR-branch-to-PIN nerve transfers (injury less than 12 months); 13 had PT/FCU/PL tendon transfers (paralysis at least 15 months)
- Nerve transfer gave better wrist flexion-extension arc and grip strength than tendon transfer
- Tendon transfer caused wrist flexion limitation in 9 of 13 and permanent radial deviation in 5 of 13
- Independent finger extension at any wrist position was achieved in all nerve-transfer but few tendon-transfer patients
- Both groups had a residual ~30° thumb MCP extension lag reflecting poor EPL recovery
Nerve Transfer versus Tendon Transfer for Radial Palsy: Systematic Review and Meta-analysis
- 21 studies, 542 patients pooled comparing tendon transfer (TT) and nerve transfer (NT)
- Excellent recovery (Bincaz scale) higher with TT (29% vs 11%)
- Failure to extend fingers higher with TT (49% vs 9%); 18% of TT patients required revision surgery
- Patient satisfaction 89% and inability to return to work only 7% after TT
- Radial deviation occurred in 18% after TT versus 0% after NT; no significant DASH difference between groups