Wear Debris → Osteolysis → Implant Migration | Rule Out Infection | Paprosky Classification
GRUEN ZONES (FEMORAL)
Critical Must-Knows
- Aseptic loosening = implant failure due to particle-induced osteolysis, NOT infection
- Wear debris (polyethylene, metal, cement) triggers macrophage activation
- Gruen zones (1-7) for femur, DeLee/Charnley (I-III) for acetabulum
- Rule out infection with ESR, CRP, aspiration before labeling as aseptic
- Paprosky classification guides bone loss management in revision surgery
Clinical Pearls
- "Aseptic loosening is a biologic process - particle disease
- "Progressive radiolucent lines, migration, subsidence on serial X-rays
- "Must exclude infection - aspirate if any doubt
- "Revision complexity depends on bone loss (Paprosky)
Critical Aseptic Loosening Exam Points
Particle Disease Pathway
Wear debris from bearing surfaces (PE most common) or cement triggers macrophage activation → cytokine release (TNF-α, IL-1, IL-6) → osteoclast recruitment → bone resorption → osteolysis → loosening. This is a biologic, not mechanical, process.
Infection Exclusion Critical
Never assume aseptic without workup. Check ESR, CRP (elevated in infection), hip aspiration (cell count, culture), and consider alpha-defensin or synoviasure. Infection has different management (2-stage vs 1-stage revision).
Radiographic Zones
Gruen zones 1-7 (femoral stem): Zone 1 (calcar resorption/subsidence), Zone 7 (stress shielding). DeLee/Charnley I-III (acetabular): Zone I superior, Zone II medial, Zone III inferior. Progressive lucent lines indicate loosening.
Migration vs. Subsidence
Migration = lateral shift, rotation, or tilt. Subsidence = distal vertical settling. More than 5mm migration in 2 years indicates loosening. Early settling under 2mm may be stable in uncemented stems.
Quick Decision Guide - Aseptic vs Septic Loosening
| Feature | Aseptic Loosening | Septic Loosening |
|---|---|---|
| Onset | Gradual (years), progressive pain | Acute or subacute, persistent pain |
| ESR/CRP | Normal or mildly elevated | Elevated (CRP more than 10, ESR more than 30) |
| Aspiration WCC | Less than 3000 cells/μL | More than 3000 cells/μL (PMN more than 80%) |
| Radiology | Progressive lucent lines, focal osteolysis | Rapid bone loss, periosteal reaction |
| Treatment | Single-stage revision | Two-stage revision (usually) |
PARTICLE - MPARTICLE - Mechanism of Aseptic Loosening
| P | Polyethylene wear debris Most common source of particles |
| A | Activation of macrophages Phagocytosis of particles |
| R | Release of cytokines TNF-α, IL-1, IL-6, RANKL |
| T | T-cell involvement Adaptive immune response |
| I | Inflammation (chronic) Periprosthetic membrane formation |
| C | Cytokine-driven osteoclasts RANKL activates osteoclasts |
| L | Lysis of bone (osteolysis) Bone resorption around implant |
| E | Eventually loosens implant Loss of fixation, migration |
| P | Polyethylene wear debris Most common source of particles | T | T-cell involvement Adaptive immune response | L | Lysis of bone (osteolysis) Bone resorption around implant |
| A | Activation of macrophages Phagocytosis of particles | I | Inflammation (chronic) Periprosthetic membrane formation | E | Eventually loosens implant Loss of fixation, migration |
| R | Release of cytokines TNF-α, IL-1, IL-6, RANKL | C | Cytokine-driven osteoclasts RANKL activates osteoclasts |
Hook:PARTICLE describes the cascade from wear debris to implant loosening - it's a biologic process
1-7GRUEN - Femoral Stem Zones (1-7)
| G | Greater trochanter region (Zone 1) Proximal medial, calcar region |
| R | Region just below (Zone 2) Medial mid-stem |
| U | Under the stem tip (Zone 4) Distal tip region |
| E | East side proximal (Zone 7) Proximal lateral |
| N | Next zones lateral (5, 6) Lateral mid and distal |
| G | Greater trochanter region (Zone 1) Proximal medial, calcar region | E | East side proximal (Zone 7) Proximal lateral |
| R | Region just below (Zone 2) Medial mid-stem | N | Next zones lateral (5, 6) Lateral mid and distal |
| U | Under the stem tip (Zone 4) Distal tip region |
Hook:GRUEN zones: 1 and 7 are proximal (medial and lateral), 2-6 spiral down medial then lateral
I-IIIDeLee - Acetabular Zones (I-III)
| D | Dome (Zone I) Superior weight-bearing region |
| e | medial (Zone II) Central medial region |
| L | Lower (Zone III) Inferior/ischial region |
| e | each zone important Lucency location matters |
| e | evaluate all three Check all zones systematically |
| D | Dome (Zone I) Superior weight-bearing region | e | each zone important Lucency location matters |
| e | medial (Zone II) Central medial region | e | evaluate all three Check all zones systematically |
| L | Lower (Zone III) Inferior/ischial region |
Hook:DeLee zones: I (superior dome), II (medial), III (inferior) - think clockwise from top
ASPIRATION - WASPIRATION - When to Aspirate Hip
| A | Any elevated inflammatory markers ESR more than 30, CRP more than 10 |
| S | Systemic symptoms present Fever, malaise, weight loss |
| P | Pain out of proportion Worse than expected for aseptic |
| I | Implant failing rapidly Rapid bone loss on X-ray |
| R | Revision being planned Always rule out before revision |
| A | Acute onset symptoms Not gradual deterioration |
| T | Temperature elevation Persistent low-grade fever |
| I | Infection history Previous wound issues |
| O | Obvious clinical suspicion Sinus, drainage, warmth |
| N | Never assume aseptic When in doubt, aspirate |
| A | Any elevated inflammatory markers ESR more than 30, CRP more than 10 | I | Implant failing rapidly Rapid bone loss on X-ray | T | Temperature elevation Persistent low-grade fever | N | Never assume aseptic When in doubt, aspirate |
| S | Systemic symptoms present Fever, malaise, weight loss | R | Revision being planned Always rule out before revision | I | Infection history Previous wound issues | ||
| P | Pain out of proportion Worse than expected for aseptic | A | Acute onset symptoms Not gradual deterioration | O | Obvious clinical suspicion Sinus, drainage, warmth |
Hook:ASPIRATION - When to aspirate: essentially, when ANY suspicion of infection exists
Overview and Epidemiology
Aseptic loosening is the most common indication for revision total hip arthroplasty in the late postoperative period (beyond 5 years). It represents failure of implant fixation due to particle-induced osteolysis rather than infection.
Definition:
- Loss of mechanical fixation between implant and bone
- Due to biologic reaction to wear debris (particle disease)
- Progressive bone resorption (osteolysis) around implant
- Results in pain, migration, and eventual mechanical failure
Epidemiology:
- Most common late cause of revision THA: aseptic loosening (with associated osteolysis) is the single most frequent indication for revision in joint registry data. [1]
- Conventional polyethylene carried a high long-term failure burden — in a 10-year RCT the conventional UHMWPE arm had 38% osteolysis and a 14.6% revision rate. [2]
- Highly cross-linked polyethylene (HXLPE) reduced that to 8% osteolysis and 1.9% revision at 10 years. [2]
- Typical presentation: progressive over years, most often becoming symptomatic beyond 5-10 years from the primary procedure.
Modern Improvements
Highly cross-linked polyethylene (HXLPE) dramatically reduces particle generation. In a 10-year double-blinded RCT the 3D wear rate fell from a mean of 0.27 mm/year (conventional UHMWPE) to 0.03 mm/year (HXLPE), with osteolysis falling from 38% to 8% and revision from 14.6% to 1.9%. [2] This lower particle load is the principal modern defence against aseptic loosening.
Risk factors for aseptic loosening:
- Young, active patients - higher wear rates
- Obesity - increased joint forces
- Poor implant positioning - edge loading, impingement
- Conventional polyethylene - higher wear
- Thin cement mantles - cement fracture
- Undersized components - inadequate fixation
- Osteolysis-prone patients - genetic factors (cytokine polymorphisms)
Pathophysiology - Particle Disease
The particle disease cascade:
Aseptic loosening is fundamentally a biologic process driven by wear particles, not a purely mechanical phenomenon.
Step 1: Particle Generation
- Polyethylene wear (most common source)
- Metal-on-metal wear (cobalt/chromium particles)
- Ceramic particles (if liner fracture)
- Cement particles (PMMA debris)
- Corrosion products (at modular junctions)
Step 2: Particle Distribution
- Particles migrate along effective joint space
- Enter periprosthetic tissues via joint fluid pumping
- Size matters: 0.1-10 micron particles most biologically active
- Smaller particles more phagocytosable, larger particles accumulate
Step 3: Macrophage Activation
- Macrophages phagocytose wear particles
- Frustrated phagocytosis - cannot digest polyethylene
- Macrophage activation and cytokine release
- Key cytokines: TNF-α, IL-1β, IL-6, RANKL
Step 4: Osteoclast Recruitment
- RANKL binds to RANK on osteoclast precursors
- OPG (osteoprotegerin) normally inhibits RANKL
- Imbalance: RANKL/OPG ratio increased
- Osteoclast activation and bone resorption
Step 5: Osteolysis and Membrane Formation
- Periprosthetic membrane forms (granulation tissue)
- Contains macrophages, giant cells, particles
- Progressive bone resorption creates cystic lesions
- Membrane extends along implant-bone interface
Step 6: Mechanical Loosening
- Loss of bone support
- Micromotion increases
- Further particle generation (vicious cycle)
- Implant migration or subsidence
Vicious Cycle
Loosening creates more micromotion → generates more particles → drives more osteolysis → creates more loosening. This is why early detection and intervention are important - the process accelerates once established.
Genetic factors:
- Polymorphisms in cytokine genes (TNF-α, IL-1)
- Some patients are high responders to particles
- Explains variability in osteolysis rates with similar wear
Classification Systems and Radiographic Assessment
Gruen Zones (Femoral Component)
The femur is divided into 7 zones around the stem on AP radiograph.
Proximal regions:
- Zone 1: Proximal medial (calcar region)
- Zone 7: Proximal lateral (greater trochanter region)
Mid-stem regions:
- Zone 2: Medial mid-stem (above Zone 3)
- Zone 6: Lateral mid-stem (above Zone 5)
Distal regions:
- Zone 3: Medial distal
- Zone 5: Lateral distal
- Zone 4: Tip of stem (below stem tip)
Clinical significance:
- Zone 1 lucency: Calcar resorption, subsidence risk
- Zone 7 lucency: Stress shielding (common, may be stable)
- Circumferential lucency (all zones): Definitely loose
- Progressive lucency (increasing on serial films): Loosening
- Lucency more than 2mm: Concerning for loosening
Zone 7 Stress Shielding
Stress shielding in Zone 7 (proximal lateral) is common with stiff stems and may be stable if non-progressive and stem otherwise well-fixed distally. This differs from true loosening which is progressive and often circumferential.
Clinical Presentation and Assessment
History:
- Onset: Gradual, progressive (years not weeks)
- Pain: Groin pain (acetabular) or thigh pain (femoral)
- Start-up pain: Worse after rest, improves with walking
- Activity limitation: Progressive difficulty with activities
- Previous function: Often initially well-functioning THA
- Time since surgery: Typically more than 5-10 years
Symptoms suggesting aseptic (not septic):
- Gradual onset over months to years
- No systemic symptoms (no fever, malaise)
- Pain improving with activity (mechanical)
- No night sweats or constitutional symptoms
Symptoms raising suspicion for infection:
- Acute or subacute onset
- Persistent pain despite rest
- Systemic symptoms (fever, malaise)
- Night pain, rest pain
- History of wound problems
Physical examination:
Physical Examination Findings
| Finding | Significance | Interpretation |
|---|---|---|
| Antalgic gait | Pain with weight-bearing | Mechanical pain from loosening |
| Groin pain on axial load | Acetabular component loosening | Positive impingement test |
| Thigh pain on axial load | Femoral component loosening | Start-up pain typical |
| Leg length discrepancy | Component migration | Measure and compare to prior |
| Normal wound, no warmth | Suggests aseptic | Infection would show inflammation |
| Erythema, warmth, sinus | Suggests septic | Requires infection workup |
Range of motion:
- Usually preserved unless severe migration
- Pain at end range if impingement
- Stiffness suggests other pathology (infection, heterotopic ossification)
Neurovascular examination:
- Document distal pulses, sensation
- Sciatic nerve (prior posterior approach)
- Femoral nerve (prior anterior approach)
Investigations and Differential Diagnosis
Differential diagnosis of the painful THA
Aseptic loosening is a diagnosis of exclusion. Systematically consider intrinsic and extrinsic causes before attributing pain to loosening.
Differential Diagnosis of the Painful Total Hip Replacement
| Cause | Discriminating features | Key investigation |
|---|---|---|
| Aseptic loosening | Gradual start-up/thigh or groin pain, progressive lucent lines, normal-to-mildly raised markers | Serial radiographs; aspiration to exclude PJI |
| Periprosthetic joint infection | Rest/night pain, sometimes acute, raised ESR/CRP, possible sinus | Serum ESR/CRP then aspiration; 2018 ICM score |
| Periprosthetic fracture | Acute pain after a fall, deformity, inability to weight-bear | Radiographs (Vancouver classification) |
| Instability / recurrent dislocation | Pain with specific positions, episodes of giving way | Examination, radiographs, component-position CT |
| Adverse reaction to metal debris (ARMD/pseudotumour) | MoM or modular-junction implant, groin mass, effusion | Serum cobalt/chromium, MARS MRI / ultrasound |
| Iliopsoas impingement / tendinitis | Groin pain on active hip flexion/stairs, oversized or prominent cup | Examination, CT for cup overhang, diagnostic injection |
| Referred lumbar spine pathology | Back-dominant pain, radicular features, normal hip on exam | Spine examination, lumbar imaging |
| Trochanteric bursitis / abductor pathology | Lateral tenderness, pain lying on side, Trendelenburg | Examination, ultrasound/MRI of abductors |
| Stress shielding / thigh pain (well-fixed stem) | Activity-related thigh pain with stiff stem, no progression | Serial radiographs showing stable fixation |
Radiographic workup:
Standard X-rays (AP pelvis, AP hip, lateral hip):
- Compare to prior films (serial assessment)
- Evaluate Gruen zones (femur) and DeLee/Charnley zones (acetabulum)
- Measure lucent lines (width and extent)
- Assess for migration (quantify displacement)
- Look for osteolysis (focal bone loss)
- Evaluate cement mantle (if cemented)
CT scan (if planning revision):
- Better assessment of bone loss (Paprosky classification)
- Identify osteolysis not visible on X-ray
- Evaluate pelvic discontinuity
- Plan reconstruction strategy
- 3D reconstruction for templating
Laboratory investigations:
Laboratory Investigations - Infection Screening
| Test | Aseptic Loosening | Infection | Action |
|---|---|---|---|
| ESR | Normal or mildly elevated (under 30) | Elevated (more than 30) | First-line screening |
| CRP | Normal (under 10 mg/L) | Elevated (more than 10 mg/L) | More specific than ESR |
| WBC | Normal | May be elevated | Less specific for PJI |
| IL-6 | Normal or mildly elevated | Elevated | Research tool mostly |
Hip aspiration (when to perform):
Indications for aspiration:
- Any elevated inflammatory markers (ESR more than 30, CRP more than 10)
- Clinical suspicion of infection
- All revisions (rule out infection before any revision)
- Atypical presentation
- Rapid bone loss
Aspiration technique:
- Fluoroscopic or ultrasound guidance
- Lateral approach (avoid contamination)
- Send for: cell count with differential, culture (hold 14 days), alpha-defensin
- Stop antibiotics 2 weeks before aspiration
Aspiration interpretation:
Synovial Fluid Analysis
| Parameter | Aseptic | Infected | Threshold |
|---|---|---|---|
| WBC count | Less than 3000 cells/μL | More than 3000 cells/μL | 3000 cells/μL |
| PMN percentage | Less than 80% | More than 80% | 80% PMNs |
| Alpha-defensin | Negative | Positive | High specificity |
| Culture | Negative | Positive | Gold standard but 7% false negative |
MSIS Criteria
Major criteria for PJI (any one = infected):
- Sinus tract communicating with prosthesis
- Two positive cultures of same organism
Minor criteria (need threshold score):
- Elevated ESR (more than 30) or CRP (more than 10)
- Elevated synovial WBC (more than 3000) or PMN (more than 80%)
- Positive alpha-defensin
- Positive histology (more than 5 PMNs per high-power field)
If major criteria absent, use scoring system with minor criteria. Always rule out infection before labeling as aseptic.
Additional investigations:
Nuclear medicine (if diagnosis uncertain):
- Bone scan (Tc-99m): Sensitive but not specific
- Labeled WBC scan (In-111 or Tc-99m): More specific for infection
- FDG-PET: High sensitivity for infection but expensive
Other tests:
- D-dimer: Elevated in infection (but not specific)
- Synoviasure: Newer biomarker panel
- PCR for organisms: If culture-negative but high suspicion
Management Algorithm
Step 1: Confirm diagnosis of loosening
- Serial radiographs showing progression
- Definite radiographic criteria (migration, lucency)
- Exclude other causes of pain (referred, spine)
Step 2: Rule out infection
- ESR, CRP (if elevated → aspirate)
- Hip aspiration if any suspicion
- MSIS criteria to classify as aseptic vs septic
Step 3: Assess symptoms and function
- Pain severity and functional limitation
- Impact on activities of daily living
- Patient expectations and goals
Step 4: Determine treatment approach
- Symptomatic + radiographic progression → Surgery
- Asymptomatic + early changes → Observation with serial X-rays
- Minimal symptoms + stable → Conservative management
This systematic assessment guides appropriate management decisions for each patient.
Surgical Technique - Revision for Aseptic Loosening
Surgical Approach Selection
Posterior approach (most common):
- Good exposure to acetabulum and femur
- Extensile if needed (trochanteric slide/osteotomy)
- Familiar to most surgeons
- Risk: Dislocation (especially if prior posterior approach)
Direct anterior approach:
- If prior anterior primary
- Good acetabular exposure
- Difficult femoral exposure for revision
- Limited extensile options
Lateral approach:
- Less common for revisions
- Risk to abductors
- Transtrochanteric extension possible
Extended trochanteric osteotomy (ETO):
- For difficult femoral extraction
- Well-fixed uncemented stems
- Cement column removal
- Allows distal access to femur
- Must repair and protect postoperatively
Key principles:
- Adequate exposure is critical
- Protect neurovascular structures
- Plan extensile approach if needed
- Don't fight through small exposure
Extended approaches allow safer component removal and better access for reconstruction.
Complications of Revision THA
Complications of Revision for Aseptic Loosening
| Complication | Incidence | Prevention/Management |
|---|---|---|
| Dislocation | 5-15% (higher than primary) | Restore offset, tension; constrained liner if needed |
| Intraoperative fracture | 5-10% | Careful extraction; ETO for well-fixed stems |
| Periprosthetic fracture (postop) | 2-5% | Protected weight-bearing; adequate fixation |
| Nerve injury | 1-3% | Careful retraction; document preop exam |
| Infection | 2-5% | Antibiotic prophylaxis; minimize operative time |
| Leg length discrepancy | Common | Templating; intraoperative measurement |
| Re-revision | 10-15% at 10 years | Address bone loss adequately; stable fixation |
| Thromboembolic disease | 1-2% | Chemical and mechanical prophylaxis |
Dislocation:
- Higher risk than primary THA (abductor damage, soft tissue laxity)
- Restore offset and leg length
- Consider constrained liner or dual-mobility
- Posterior repair if posterior approach
Intraoperative fracture:
- Femoral fractures during stem removal (most common)
- Treat with cerclage cables and/or revision to longer stem
- Acetabular fractures (medial wall blow-out)
- May need cage or column plating
Nerve injury:
- Sciatic nerve most at risk (posterior approach, retraction)
- Femoral nerve (anterior approach)
- Document preoperative exam
- Avoid excessive retraction and leg lengthening
Infection:
- Higher risk in revision than primary
- Meticulous debridement
- Antibiotic prophylaxis
- Consider vancomycin powder locally (controversial)
Dislocation Risk
Dislocation rates are higher after revision (5-15%) than primary (1-3%). Contributing factors: soft tissue damage, abductor insufficiency, poor bone stock affecting component position. Consider dual-mobility bearings or constrained liners in high-risk patients.
Postoperative Care and Rehabilitation
Immediate postoperative care:
- ICU/HDU if complex or prolonged case
- DVT prophylaxis (chemical and mechanical)
- Pain management (multimodal, avoid excessive opioids)
- Monitor hemoglobin (transfuse if needed)
- Foley catheter typically removed day 1
- Early mobilization to chair
- Physiotherapy with walking frame
- Partial weight-bearing (if uncemented femur)
- Toe-touch weight-bearing (if ETO)
- Hip precautions (if posterior approach)
- Wound inspection
- Progress to crutches or walker
- Progressive weight-bearing (if stable fixation)
- Continue hip precautions for 6-12 weeks
- Outpatient physiotherapy
- Wound check at 2 weeks (remove sutures/staples)
- First follow-up X-rays at 6 weeks
- Advance to full weight-bearing (if healing well)
- Wean from walking aids
- ETO protected until union (usually 12 weeks)
- Progressive strengthening exercises
- Monitor for complications
- Return to normal activities gradually
- Avoid high-impact sports indefinitely
- Serial X-rays to monitor fixation (6 weeks, 3 months, 1 year)
- Long-term follow-up annually
Weight-bearing restrictions:
- Uncemented acetabulum: Partial weight-bearing for 6 weeks
- Extensively coated femoral stem: May allow immediate weight-bearing
- Extended trochanteric osteotomy: Toe-touch for 6 weeks, partial for 6-12 weeks
- Bone grafting: Protected weight-bearing until graft incorporation
Hip precautions (if posterior approach):
- No hip flexion more than 90 degrees
- No adduction past midline
- No internal rotation
- Duration: 6-12 weeks (surgeon preference)
Monitoring for complications:
- Wound infection signs (erythema, drainage)
- DVT/PE symptoms (leg swelling, chest pain)
- Neurovascular status
- Pain out of proportion (compartment syndrome rare)
Long-term follow-up:
- Radiographs: 6 weeks, 3 months, 1 year, then annually
- Monitor for loosening, wear, osteolysis
- Document stable fixation (osseointegration)
- Check for heterotopic ossification
Outcomes and Prognosis
Revision THA outcomes:
Modern techniques and implants have improved revision THA outcomes substantially.
Survivorship (freedom from re-revision):
- 10-year survivorship: 80-90% (modern series)
- 15-year survivorship: 70-80%
- Worse outcomes with severe bone loss (Paprosky IIIB/IV)
Factors affecting outcomes:
Patient factors:
- Age (younger patients higher revision risk)
- Activity level
- BMI (obesity increases failure risk)
- Bone quality
Surgical factors:
- Severity of bone loss (Paprosky grade)
- Surgeon experience with revisions
- Achieving stable fixation
- Managing soft tissue/abductor integrity
Implant factors:
- Extensively coated stems (better outcomes than cemented in Paprosky III)
- Tantalum augments/cups (good outcomes in deficient acetabulum)
- Constrained liners (higher dislocation rate but necessary in some)
Functional outcomes:
- Most patients achieve pain relief
- Functional scores improve (Harris Hip Score, WOMAC)
- Return to low-impact activities
- Avoid high-impact sports
Implant-specific revision survivorship (representative series):
- Extensively porous-coated diaphyseal femoral stems: re-revision for aseptic femoral loosening 3% at 20 years, any-cause femoral re-revision 6.4% at 20 years. [4]
- Trabecular-metal/titanium revision cups for severe acetabular bone loss: 100% at 5 years and 88% at 10 years. [5]
- Dual-mobility and constrained bearings are used to manage the elevated dislocation risk of the revision setting (see Complications).
Registry Data
Across the major registries, aseptic loosening revision rates have fallen with modern bearings (HXLPE) and porous fixation. [1][2] However, once loosening occurs revision is complex and outcomes remain inferior to primary THA — prevention through optimal bearing choice and primary technique is the key message.
Evidence Base
HXLPE Reduces Wear, Osteolysis and Revision at 10 Years - Double-Blinded RCT
- Double-blinded RCT of 122 hips randomised to highly cross-linked (XLPE) versus conventional UHMWPE liners, minimum 10-year follow-up
- 3D wear rate significantly lower with XLPE (mean 0.03 mm/yr) versus conventional UHMWPE (mean 0.27 mm/yr) (less than 0.001)
- Osteolysis prevalence 8% (XLPE) versus 38% (conventional) (less than 0.005)
- Revision rate 1.9% (XLPE) versus 14.6% (conventional) (p = 0.012); 10 of 12 revisions were in the conventional group
Cellular and Molecular Biology of Periprosthetic Osteolysis
- Implant wear debris is the major initiating event in periprosthetic osteolysis and aseptic loosening
- Wear particles primarily target macrophages and osteoclast precursors, activating MAP kinase pathways and NF-kappaB
- Net effect is up-regulation of pro-inflammatory signalling (including TNF) and RANKL-driven osteoclastogenesis
- Reducing particle size to lower bulk wear may paradoxically increase biological activity of the debris
2018 Evidence-Based and Validated Definition of Periprosthetic Hip and Knee Infection
- Major criteria (two positive cultures of the same organism, or a sinus tract) remain diagnostic of PJI
- Weighted minor criteria: serum CRP greater than 1 mg/dL (2), D-dimer greater than 860 ng/mL (2), ESR greater than 30 mm/hr (1); synovial WBC greater than 3000 cells/microL (3), alpha-defensin (3), leukocyte esterase ++ (3), PMN greater than 80% (2), synovial CRP greater than 6.9 mg/L (1)
- Aggregate preoperative score of 6 or more = infected; 2-5 is inconclusive and requires intra-operative findings
- New definition sensitivity 97.7% versus 79.3% (MSIS 2011), specificity 99.5%
Evaluation and Management of Acetabular Bone Loss in Revision THA: 10-Year Update
- The Paprosky classification remains the most widely used system for acetabular bone loss and is defined by integrity of the anterosuperior and posteroinferior columns
- Cemented reconstruction has declined; highly porous hemispherical shells with modular porous-metal augments now treat most acetabular revisions
- Cup-cage reconstruction, custom triflange and acetabular distraction are reserved for chronic pelvic discontinuity and severe (Type III) defects
- Careful radiographic assessment can identify pelvic discontinuity pre-operatively and direct construct choice
Extensively Porous-Coated Stems: Excellent Long-Term Survivorship in Revision THA
- 925 extensively porous-coated cylindrical stems in revision THA, mean 13-year follow-up
- Cumulative incidence of re-revision for aseptic femoral loosening 3% at 20 years; any-cause femoral re-revision 6.4% at 20 years
- 94% of un-revised stems were radiographically bone-ingrown
- Stem fracture clustered in 10.5-13.5 mm diameters; femoral bone loss and stem length were not predictors of re-revision
Trabecular Titanium Cups in Acetabular Revision: 10-Year Survivorship
- 85 acetabular revisions using trabecular titanium revision cups for severe bone loss, mean 6.1-year follow-up
- Harris Hip Score improved from 54.7 to 89.7 (less than 0.05)
- Only 2 cups (2.3%) re-revised (one aseptic loosening, one infection)
- 5-year and 10-year survivorship 100% and 88% respectively
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Presentation of Aseptic Loosening
"A 68-year-old man presents with progressive groin pain 12 years after cemented THA. He had good function until 18 months ago when pain gradually worsened. X-rays show progressive lucent lines in DeLee/Charnley zones I and II around the acetabular component, measuring 3mm. Gruen zone 1 and 7 show 2mm lucent lines on the femoral side. ESR is 18, CRP is 6. How do you assess and manage this patient?"
Scenario 2: Differentiating Aseptic from Septic Loosening
"A 72-year-old woman presents with 6 months of progressive hip pain, 8 years after uncemented THA. X-rays show lucent lines around the femoral stem in all Gruen zones. ESR is 45, CRP is 18. She has no fever or systemic symptoms. How do you proceed?"
Scenario 3: Severe Bone Loss - Paprosky IIIB
"You are planning revision THA for aseptic loosening. The CT scan shows Paprosky Type IIIB acetabular bone loss with superior migration more than 4cm and destruction of the ischium and teardrop. There is also complete loss of the anterior and posterior columns. How do you manage this acetabular defect?"
MCQ Practice Points
Mechanism Question
Q: What is the primary mechanism by which polyethylene wear debris causes osteolysis in aseptic loosening?
A: Macrophage activation leading to cytokine release (TNF-α, IL-1, IL-6, RANKL). These cytokines recruit and activate osteoclasts, causing bone resorption. This is a biologic process (particle disease), not purely mechanical loosening.
Zone Question
Q: A patient has a 3mm lucent line in Gruen zone 1. What does this indicate?
A: Gruen zone 1 is the proximal medial (calcar) region. A 3mm lucent line (threshold is 2mm) indicates calcar resorption and suggests femoral component loosening or impending subsidence. This is concerning and warrants close follow-up or consideration of revision.
Infection Differentiation
Q: What is the threshold synovial fluid white blood cell count that suggests periprosthetic joint infection rather than aseptic loosening?
A: More than 3000 cells/μL OR more than 80% polymorphonuclear cells (PMNs). Either of these thresholds is a minor criterion in the MSIS criteria for PJI. Aseptic loosening typically has synovial WBC less than 3000 with less than 80% PMNs.
Classification Question
Q: A revision THA CT shows acetabular superior migration of 4cm with destruction of the ischium and teardrop. What Paprosky classification is this?
A: Paprosky Type IIIB. Type III is defined by superior migration more than 3cm. Type IIIB specifically has ischial and teardrop destruction (loss of Köhler's line), indicating severe bone loss. This requires complex reconstruction (cup-cage or triflange).
Treatment Question
Q: What is the primary advantage of highly cross-linked polyethylene (HXLPE) over conventional polyethylene in THA?
A: Reduced wear rate by 80-90% (from 0.1-0.2mm/year to under 0.05mm/year). This reduces particle generation, decreasing osteolysis and aseptic loosening rates. Registry data shows HXLPE has significantly improved long-term implant survivorship.
Radiology Question
Q: What radiographic finding is definitive for component loosening?
A: Migration of the component (change in position more than 5mm in 2 years) or component/cement fracture. Progressive lucent lines suggest loosening but are not definitive until migration occurs or lucency becomes circumferential (more than 2mm).
Guidelines, Registries & Global Practice
This section frames aseptic loosening as a global problem, drawing on the major national joint registries as cited evidence rather than the practice of any single country.
Global epidemiology
- THA volume — and therefore the at-risk population for late loosening — is rising worldwide. Registry-based modelling in Australia projected a 208% increase in primary THA for osteoarthritis between 2013 and 2030. [3] Ageing populations and rising obesity drive similar trends across high-income registries.
- Aseptic loosening / osteolysis is the leading recorded indication for revision THA in registry data; in the National Joint Registry of England and Wales it ranks ahead of dislocation, pain and periprosthetic fracture as a cause of single-stage revision. [1]
- The dominant modifiable driver historically was conventional polyethylene wear; the shift to HXLPE has reduced osteolysis and revision substantially. [2]
Major guidelines and consensus, side by side
Guidance Relevant to the Loose THA (where bodies differ)
| Body / Region | Position | Evidence basis |
|---|---|---|
| ICM / MSIS (international consensus) | Exclude PJI in EVERY painful/loose THA using the 2018 weighted scoring system before calling it aseptic | Multicentre diagnostic validation, sensitivity 97.7% |
| AAOS (USA) | Routine serum ESR and CRP first-line in suspected PJI; aspirate if raised or clinical suspicion | Evidence-based CPG (moderate-strong) |
| NICE / BOA (UK) | Surveillance imaging of THA and prompt specialist referral for a painful prosthesis; revision in units with appropriate expertise | Guideline / consensus |
| EFORT / European | Bearing-surface optimisation (HXLPE, ceramic) to reduce wear-driven osteolysis; classify bone loss before revision | Consensus, registry-supported |
Registry evidence (implant survival and revision)
What the Joint Registries Show
| Registry | Region | Relevance to aseptic loosening |
|---|---|---|
| NJR | England, Wales, NI | Aseptic loosening/osteolysis the leading cause of revision; basis for ODEP implant benchmarking |
| AOANJRR | Australia | Mandatory registry; rising THA burden and reduced wear-driven failure with HXLPE |
| AJRR | USA | Largest by annual volume; tracks bearing-surface and fixation trends |
| SHAR / Swedish | Sweden | Longest follow-up; pioneered registry feedback driving lower long-term loosening |
| NZJR | New Zealand | Uses revision rate per 100 component-years; bearing comparisons |
Independent series corroborate registry signals: extensively porous-coated diaphyseal stems show only 3% re-revision for aseptic femoral loosening at 20 years [4], and trabecular-metal/titanium revision cups achieve ~88% survivorship at 10 years in deficient acetabula. [5]
Global practice variation
- Fixation philosophy differs by region: Scandinavian registries retain a strong cemented-stem tradition with excellent long-term results, while North American and Australian practice favours uncemented fixation — both achieve low aseptic-loosening rates in modern data.
- Resource setting changes the toolkit: porous-metal augments, cup-cage constructs and custom triflanges [4][5] are standard in high-resource centres, whereas impaction grafting and structural allograft remain important where modular porous metal is less available.
- Diagnostic access to alpha-defensin, leukocyte esterase and extended cultures varies, but the principle — exclude infection before revising a loose THA — is universal. [6]
Registry Importance
Whatever board you sit, know the world standard: (1) aseptic loosening is the leading registry-recorded cause of THA revision [1]; (2) HXLPE markedly lowered wear-driven osteolysis and revision [2]; (3) both cemented (Scandinavian) and uncemented (North American/Australasian) fixation achieve low loosening in modern registries; (4) always apply the 2018 PJI scoring system before labelling loosening aseptic. [6]
ASEPTIC LOOSENING IN THA
Clinical summary
DEFINITION AND MECHANISM
- •Aseptic loosening = implant failure due to particle-induced osteolysis (NOT infection)
- •Particle disease: PE wear → macrophage activation → cytokines (TNF-α, IL-1, RANKL) → osteoclasts → bone resorption
- •Vicious cycle: loosening → micromotion → more particles → more osteolysis
- •Most common late cause of THA revision (10-15 years post-primary)
RADIOGRAPHIC ZONES
- •Gruen zones 1-7 (femur): Zone 1 (calcar), Zone 7 (lateral proximal)
- •DeLee/Charnley I-III (acetabulum): Zone I (superior dome), Zone II (medial), Zone III (inferior)
- •Lucent line more than 2mm = concerning for loosening
- •Migration more than 5mm in 2 years = definite loosening
- •Serial X-rays essential - progression is key finding
INFECTION EXCLUSION (CRITICAL)
- •NEVER assume aseptic without ruling out infection
- •Check ESR (threshold 30), CRP (threshold 10)
- •If elevated markers: MUST perform hip aspiration
- •Aspiration: WBC more than 3000 or PMN more than 80% suggests infection
- •MSIS criteria: major (sinus, 2+ cultures) or minor (scored)
- •Alpha-defensin: high sensitivity/specificity for PJI
PAPROSKY CLASSIFICATION
- •Acetabular Type I: minimal bone loss (under 25%)
- •Type IIA-IIB: 25-50% loss, migration under 3cm
- •Type IIIA: migration more than 3cm, intact Köhler's line
- •Type IIIB: migration more than 3cm + ischium/teardrop destruction
- •Femoral Type I-II: metaphyseal loss, intact diaphysis
- •Type IIIA-IIIB: diaphyseal involvement
- •Type IV: non-supportive diaphysis
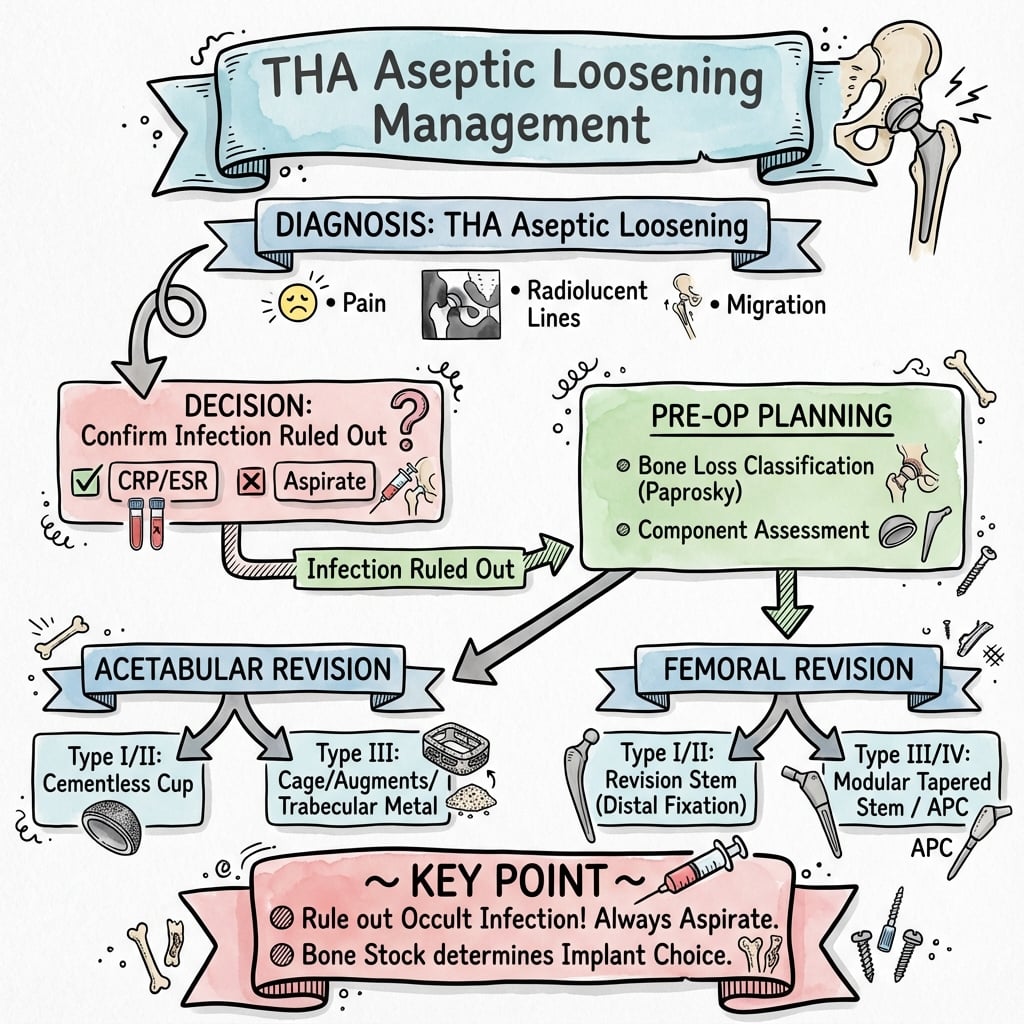
REVISION STRATEGY
- •Rule out infection first (aspiration if any doubt)
- •CT scan for bone loss assessment (Paprosky classification)
- •Type I-IIA acetabulum: standard hemispheric cup
- •Type IIB-IIIA: jumbo cup, augments, trabecular metal
- •Type IIIB: cup-cage construct or custom triflange
- •Femoral Type I-II: cemented or proximally coated
- •Type IIIA-IIIB: extensively coated diaphyseal fit
KEY EXAM POINTS
- •Aseptic loosening is biologic process (particle disease), not mechanical
- •HXLPE reduced wear by 80-90% (modern standard)
- •Always aspirate if ESR more than 30 or CRP more than 10 before revision
- •Serial X-rays show progression (single film cannot diagnose)
- •Outcomes: 80-90% survivorship at 10 years (worse than primary)
- •AOANJRR shows uncemented stems better in revision than cemented