The Great Imitator
Clinical Types
Critical Must-Knows
- Neurogenic TOS usually affects the Lower Trunk (C8/T1) - Ulnar border symptoms.
- The most common compression site is the Interscalene Triangle.
- Venous TOS is a DVT of the Subclavian Vein (Paget-Schroetter Syndrome).
- Arterial TOS is almost always associated with a bony anomaly (Cervical Rib).
- Roos Test (EAST) is the most sensitive screening test.
- Adson's Test obliterates the radial pulse (but is positive in many normal people).
Clinical Pearls
- "Gilliatt-Sumner Hand: severe wasting of Thenar AND Hypothenar muscles (Lower trunk).
- "In Ulnar nerve compression, Thenar is spared. In TOS, Thenar is wasted (C8/T1).
- "First Rib Resection is the definitive surgical treatment.
Clinical Imaging
Imaging Gallery

The Trap: Double Crush
The Diagnosis
Cervical Radiculopathy NTOS symptoms overlap with C8/T1 radiculopathy and Cubital Tunnel Syndrome. Always check the neck (Spurling's test) and the elbow (Tinel's). TOS is a diagnosis of exclusion.
The Test
APB Wasting Look at the Abductor Pollicis Brevis (APB). Carpal Tunnel affects APB. Cubital Tunnel spares APB. TOS (Lower Trunk) affects APB (T1 fibers). TOS = Wasted APB + Wasted Interossei.
| Feature | Neurogenic (NTOS) | Venous (VTOS) | Arterial (ATOS) |
|---|---|---|---|
| Symptom | Pain, Paresthesia | Swelling, Cyanosis | Pallor, Claudication |
| Nerve/Vessel | Brachial Plexus (Lower) | Subclavian Vein | Subclavian Artery |
| Cause | Scalene Hypertrophy/Scar | Repetitive Overhead (Effort) | Cervical Rib |
| Test | Roos, Elvey | Ultrasound/Venogram | Loss of Pulse, Angio |
SIPSpaces of Compression
| S | Scalene Interscalene Triangle (Between Anterior/Middle Scalene). |
| I | Intercostal Costoclavicular Space (Between Clavicle/1st Rib). |
| P | Pectoralis Subcoracoid Space (Under Pectoralis Minor). |
| S | Scalene Interscalene Triangle (Between Anterior/Middle Scalene). |
| I | Intercostal Costoclavicular Space (Between Clavicle/1st Rib). |
| P | Pectoralis Subcoracoid Space (Under Pectoralis Minor). |
Hook:Take a SIP of air (Thorax).
LOAF-IGilliatt Sumner
| L | LOAF Thenar muscles (Median). |
| I | Interossei Intrinsics (Ulnar). |
| Sum | Summary Both median and ulnar intrinsics are wasted. |
| L | LOAF Thenar muscles (Median). |
| I | Interossei Intrinsics (Ulnar). |
| Sum | Summary Both median and ulnar intrinsics are wasted. |
Hook:Lower trunk hits everything in the hand.
EASTRoos Test
| E | Elevated Arms up (Abducted/Externally Rotated). |
| A | Arm Identify ischemic pain/fatigue. |
| S | Stress Open and close fists for 3 minutes. |
| T | Test Positive if patient drops arms. |
| E | Elevated Arms up (Abducted/Externally Rotated). | S | Stress Open and close fists for 3 minutes. |
| A | Arm Identify ischemic pain/fatigue. | T | Test Positive if patient drops arms. |
Hook:Hands up facing EAST.
Overview
Definition
Thoracic Outlet Syndrome (TOS) is a spectrum of disorders caused by compression of the neurovascular bundle (Brachial Plexus, Subclavian Artery, Subclavian Vein) as it exits the thoracic aperture to enter the axilla.
The compression typically occurs at three anatomical narrows: the Interscalene Triangle, the Costoclavicular Space, and the Retro-pectoralis Minor Space.
Pathophysiology and Mechanisms
1. Interscalene Triangle
- Borders: Anterior Scalene (Anterior), Middle Scalene (Posterior), First Rib (Inferior).
- Contents: Brachial Plexus (Trunks) and Subclavian Artery.
- Note: The Subclavian Vein passes ANTERIOR to the Anterior Scalene (outside the triangle). Thus, scalene hypertrophy affects Artery/Nerve but spares Vein.
The C8/T1 roots are most vulnerable at the base of the triangle.
Classification Systems
Neurogenic TOS (NTOS)
- Prevalence: Greater than 95% of cases.
- Demographics: Women affected more than men (approximately 3:1), age 20-50.
- Pathology: Scarring of scalenes, whiplash, repetitive stress.
- Symptoms: Pain in neck/trapezius/arm. Paresthesia in C8/T1 distribution (Ulnar forearm/hand). Weakness (late).
The diagnosis is often clinical, supported by exclusion of other causes.
Clinical Assessment
History
History
- Pain: "Toothache" in the trapezius/neck.
- Activities: Worse with overhead activity (brushing hair, hanging clothes).
- Night: Pain at night (sleeping with arms up).
- Neurological: Numbness in 4th/5th digits (C8).
Ask about trauma (whiplash) which scars the scalenes.
Provocative Tests
Provocative Tests
- Roos Test (EAST): Elevated Arm Stress Test. "Hands up, open/close fists for 3 mins." Positive if pain/heaviness/numbness forces arms down. (Most reliable).
- Adson's Test: Head turned TO side + Deep breath + Extension. Positive if pulse disappears AND symptoms reproduced. (Low specificity).
- Wright's Test: Hyperabduction. Pulse disappears. (Implicates Pec Minor).
- Elvey's Test (ULTT): Upper Limb Tension Test.
Most tests have high false positive rates.
Inspection
Inspection
- Posture: Drooped shoulders?
- Hand: Gilliatt-Sumner Hand (Severe ATOS/NTOS). Wasting of Thenar AND Hypothenar.
- Supraclavicular: Fullness? (Cervical rib or mass).
Cyanosis suggests Venous TOS.
Differential Diagnosis
NTOS is a diagnosis of exclusion - the great imitator. The exam favourite is distinguishing it from the conditions that share C8/T1 or ulnar-border symptoms. Anchor your answer on the pattern of motor wasting and the level of sensory loss.
| Condition | Sensory pattern | Motor/wasting | Discriminator |
|---|---|---|---|
| Neurogenic TOS (lower trunk) | Medial forearm + hand (T1/C8, incl. MABC) | Thenar AND hypothenar wasting (Gilliatt-Sumner) | Positive scalene block; medial forearm sensory loss (proximal to wrist) |
| Cubital tunnel (ulnar at elbow) | Ulnar 1.5 digits + dorsal ulnar hand | Hypothenar/interossei; APB SPARED | Spares thenar; positive elbow flexion test and Tinel at elbow; normal medial forearm |
| Carpal tunnel (median at wrist) | Radial 3.5 digits, spares palm | APB/thenar only; spares hypothenar | Positive Phalen/Tinel at wrist; no proximal sensory loss |
| C8/T1 cervical radiculopathy | Dermatomal C8/T1 | Variable intrinsic wasting | Positive Spurling; neck pain; MRI disc/foraminal disease |
| Pancoast (apical lung) tumour | T1 with medial arm pain; Horner's | Lower trunk wasting | Constitutional symptoms; apical mass on CXR/CT - must exclude |
| Motor neurone disease (ALS) | NONE (pure motor) | Split-hand wasting, fasciculations, UMN signs | No sensory loss; widespread fasciculations; EMG |
Two cannot-miss diagnoses
Before labelling hand wasting as TOS, exclude a Pancoast tumour (apical CXR/CT, look for Horner's) and motor neurone disease (purely motor, no sensory loss, fasciculations). Both masquerade as lower-trunk plexopathy.
Imaging and Electrodiagnostics
Plain Films
- Cervical Spine: Look for a Cervical Rib (an accessory rib arising from the C7 transverse process, articulating with or fused to the first rib).
- Chest: Anomalous first rib? Clavicle malunion? apical lung tumor (Pancoast)?
Look for elongated C7 transverse processes.
Management Algorithm
Neurogenic TOS
- First Line: Conservative.
- PT: Postural correction, strengthening trapezius (elevate shoulder girdle), stretching scalenes/pec minor.
- Meds: Gabapentin/pregabalin, NSAIDs.
- Scalene block: Local anaesthetic injection into the anterior scalene is mainly diagnostic/prognostic (a positive response is part of the SVS NTOS criteria and predicts surgical benefit). Note: a placebo-controlled RCT (Finlayson 2011) found scalene Botox gave no therapeutic pain benefit, so it should not be relied on as a treatment.
- Surgery: If conservative measures fail (typically over 3-6 months). First Rib Resection plus Scalenectomy.
Surgery is reserved for refractory cases with significant disability.
Surgical Technique
Approaches
- Transaxillary: Most common. Cosmetically superior. "Roos Approach". Access to 1st rib. Hard to see C-rib or reconstruct vessels.
- Supraclavicular: Best for Nerve visualization and Cervical Rib. Standard for NTOS/ATOS.
- Infraclavicular: Good for Venous (Vein exposure).
Robotic First Rib Resection is emerging.
Complications
Intraoperative Complications
- Pneumothorax: Pleura is attached to the undersurface of the 1st rib via Sibson's fascia (15-30% risk). Chest X-ray in recovery is mandatory.
- Vascular Injury: Subclavian artery or vein laceration - requires immediate vascular repair.
- Brachial Plexus Injury: Direct trauma or excessive traction during first rib resection.
- Phrenic Nerve Palsy: Lies on anterior scalene - must protect during scalenectomy. Results in diaphragm paralysis.
- Long Thoracic Nerve: Injury causes scapular winging - avoid excessive retraction.
- Thoracic Duct Injury: Chylothorax (left-sided approach) - requires drainage and dietary modification.
Careful anatomical dissection and nerve identification prevents most complications.
Rehabilitation
- Monitoring: Chest X-ray in recovery to exclude pneumothorax.
- Protection: Arm sling for comfort (not immobilization).
- ROM: Gentle active-assisted range of motion - avoid overhead activity.
- Activity: No lifting greater than 1kg, avoid driving.
- Wound Care: Keep incision clean and dry, sutures out at 10-14 days.
Pain control with simple analgesia - avoid opioids long-term.
- ROM: Progressive active ROM in all planes.
- PT Focus: Postural correction, scapular setting, cervical stretches.
- Strengthening: Isometric exercises for shoulder girdle.
- Activity: Light activities of daily living, no repetitive overhead work.
- Driving: May resume at 3-4 weeks if comfortable.
Continue physiotherapy addressing underlying postural issues.
- PT Focus: Scapular stabilization, trapezius strengthening, pectoralis stretching.
- Progressive Loading: Gradual increase in resistance exercises.
- Work: Gradual return to desk work, avoid heavy manual labor.
- Sports: No contact sports or heavy lifting yet.
- Nerve Recovery: May take several months for complete sensory recovery.
Address any ergonomic factors at workplace.
- Full Activity: Unrestricted activity by 3 months if symptoms resolved.
- Sports: Gradual return to sports including overhead activities.
- Work: Full duties including manual labor.
- Maintenance: Continue postural exercises long-term to prevent recurrence.
- Review: Final assessment at 3-6 months post-surgery.
Some patients may require ongoing physiotherapy if postural issues persist.
Prognosis
Surgical Outcomes by Type
- NTOS: 80-90% good outcomes if diagnosis is correct and confirmed by positive scalene block response. Poorer results in "Disputed" TOS or workers' compensation cases.
- VTOS: Excellent outcomes with early thrombolysis and first rib resection. Greater than 90% long-term vein patency if treated within 2 weeks.
- ATOS: Good outcomes if arterial reconstruction is patent and no embolic sequelae. May require staged procedures.
Conservative management for NTOS achieves 50-70% improvement with dedicated physiotherapy.
Controversies and Areas of Uncertainty
Does 'disputed' NTOS exist?
The biggest controversy. Many patients have subjective outlet symptoms with no objective neurophysiology and no anatomical lesion. Some surgeons operate on the basis of a positive scalene block alone; others argue this group should rarely be offered surgery given high failure rates. The SVS 4-criteria standard was created largely to discipline this grey zone.
Provocative tests: low value
Adson's, Wright's and Roos/EAST all have high false-positive rates in asymptomatic people (a large proportion of normal individuals lose the radial pulse on Adson's). No single physical test is diagnostic - they support, never confirm, the diagnosis.
Routine venoplasty in VTOS
Balloon venoplasty must NEVER precede rib resection (the rib is the anvil - the balloon fails or ruptures the vein). Even after decompression, meta-analysis (Lugo 2015) shows adding venoplasty gives no symptom benefit over rib resection alone, so routine post-decompression venoplasty is questioned.
Surgical approach
No randomised trial settles transaxillary versus supraclavicular first rib resection. Supraclavicular favours plexus neurolysis and cervical rib excision; transaxillary favours cosmesis and direct rib access. Robotic and thoracoscopic resection are emerging but unproven against open surgery.
Evidence Base
Evidence health-warning
TOS has very few randomised data. Diagnosis of neurogenic TOS remains a clinical construct without a gold-standard reference test, and most surgical evidence comes from retrospective single-centre series. Read the numbers below in that light, and beware over-interpreting any single observational study.
SVS Reporting Standards: defining NTOS
- Society for Vascular Surgery consensus reporting standards for NTOS, VTOS and ATOS
- NTOS diagnosis requires 3 of 4 criteria: local outlet pain/tenderness, distal nerve compression signs, absence of alternative pathology, and a positive scalene muscle block
- Defines standardised work-up and outcome measures to allow comparison between series
- Explicitly frames the three TOS subtypes as separate (occasionally overlapping) entities
Gilliatt-Sumner Hand: wasting with a cervical rib/band
- Nine patients with unilateral hand wasting from an elongated C7 transverse process or rudimentary cervical rib
- Wasting was most marked in the lateral (thenar) part of the hand but involved all intrinsics in several patients - the classic Gilliatt-Sumner pattern
- A fibrous band angulating the C8/T1 roots or lower trunk was found at operation in every case
- Band division relieved pain and arrested progression, but established muscle wasting did not recover even at 8 years
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: The Swollen Arm
"A 22-year-old male weightlifter presents with specific, blue, swollen right arm after a gym session. No pain initially, now heavy."
Scenario 2: The Wasting Hand
"A 60-year-old woman has wasting of her right hand. Thenar and Hypothenar eminence are flat. Sensation is reduced in the medial forearm."
Scenario 3: The Violinist
"A professional violinist complains of pain in the neck and numbness in the 4th/5th digits when playing. Adson's is positive."
Scenario 4: Recurrent Symptoms Post-Surgery
"A 35-year-old woman had first rib resection 18 months ago for NTOS. She presents with recurrent neck and arm pain similar to pre-operative symptoms."
MCQ Practice Points
Anatomy
Q: Which structure passes ANTERIOR to the Anterior Scalene muscle? A: The Subclavian Vein. (Artery and Plexus are posterior).
Clinical Signs
Q: What is the most sensitive test for NTOS? A: Roos Test (EAST).
Pathology
Q: Which muscle fibers are most affected in 'Gilliatt-Sumner' hand? A: Both Thenar (Median) and Hypothenar (Ulnar) - C8/T1.
Management
Q: What is the treatment for Venous TOS? A: Thrombolysis followed by First Rib Resection.
Cervical Rib
Q: Which type of TOS is almost always associated with a cervical rib? A: Arterial TOS (ATOS). Bony abnormality causes post-stenotic dilation and aneurysm formation.
Compression Site
Q: What is the most common site of compression in TOS? A: Interscalene triangle (between anterior and middle scalene muscles, above first rib).
Guidelines, Registries & Global Practice
Global Epidemiology
- Distribution: Neurogenic TOS makes up roughly 90-95% of cases, venous ~3-5%, arterial ~1%.
- Sex/age: NTOS predominantly affects women (about 3:1) aged 20-50; venous (effort) thrombosis predominantly affects young athletic men.
- Cervical rib: Present in approximately 0.5-1% of the general population (radiographic studies), more common in women; only a minority ever become symptomatic. Arterial TOS is almost always associated with a bony anomaly.
- Provoking factors: Repetitive overhead work and sport (throwers, swimmers, weightlifters), prior clavicle fracture/malunion, and post-whiplash scalene scarring.
The true incidence of NTOS is unknown worldwide because there is no gold-standard diagnostic test.
Clinical summary
Anatomy
- •Triangle: Ant/Mid Scalene + Rib 1
- •Vein is Anterior to Triangle
- •C8/T1 Roots (Lower Trunk)
- •Subclavian artery passes through triangle
Types
- •Neurogenic (95%) - Pain/Numb
- •Venous (4%) - Blue/Swollen
- •Arterial (1%) - Emboli
- •Disputed - Subjective, no objective findings
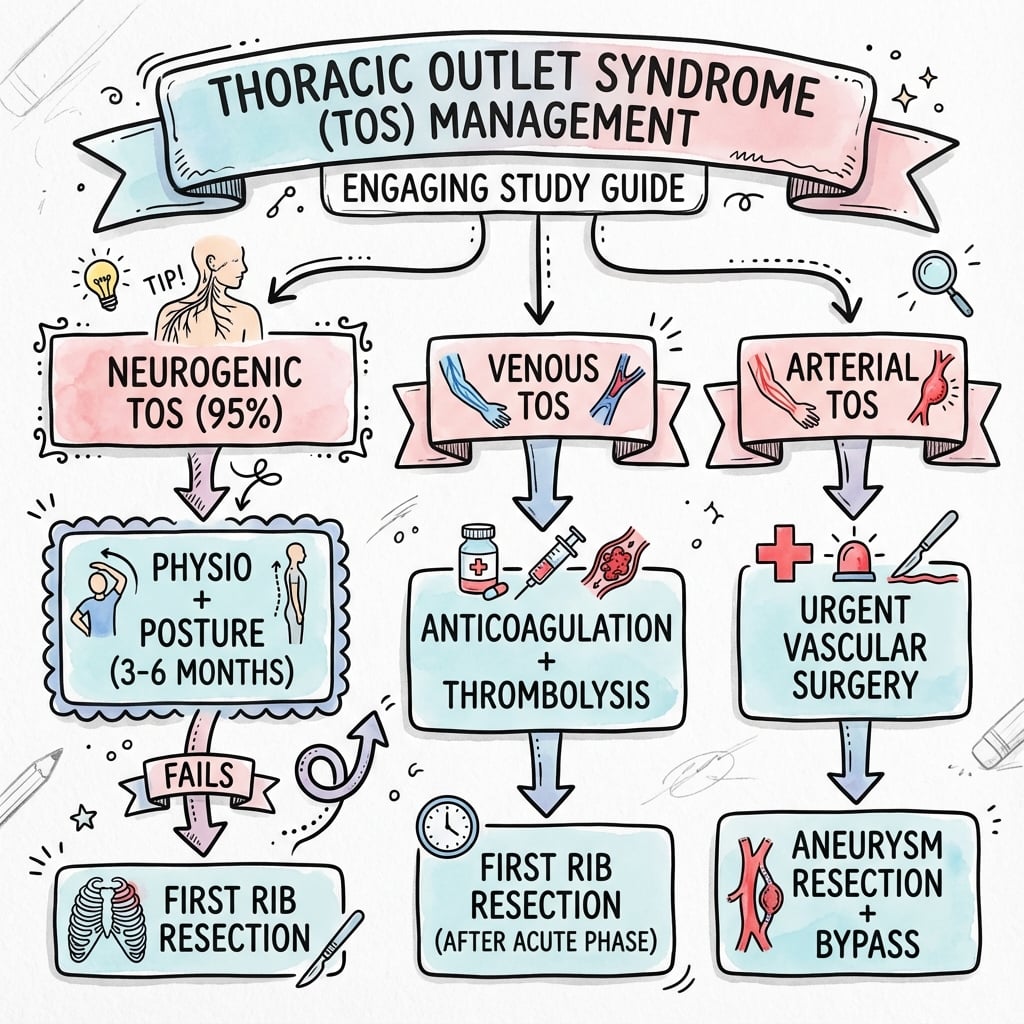
Management
- •NTOS: Physio then Resection
- •VTOS: Lysis then Resection
- •ATOS: Resection + Graft
- •First rib resection is definitive treatment