Giving the Cut Nerve Somewhere to Go
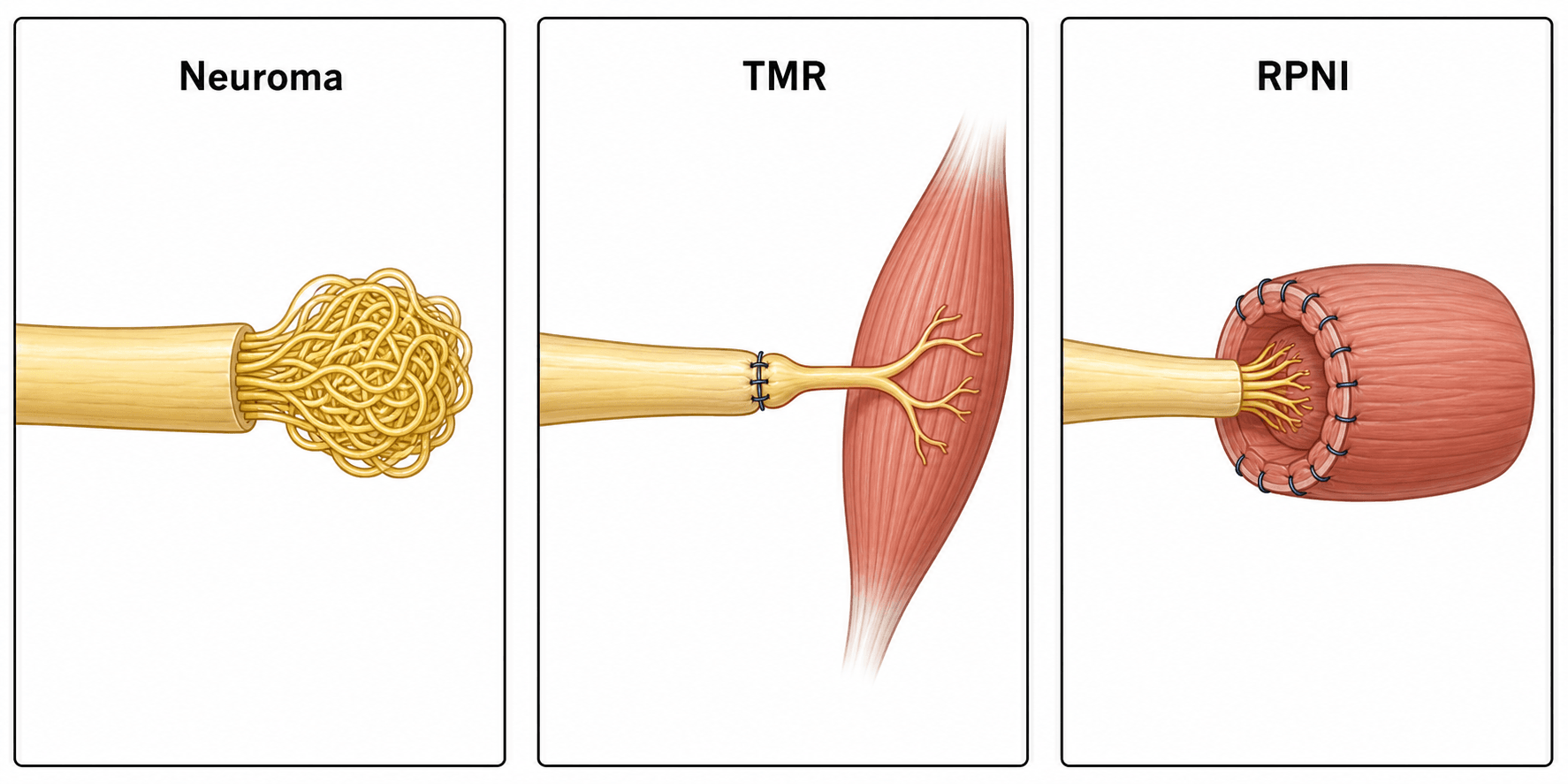
- A NEUROMA forms when a transected peripheral nerve regenerates with NO distal target - producing a disorganised, hypersensitive nerve-ending bulb that can cause severe residual-limb and neuropathic pain; amputees also suffer PHANTOM LIMB PAIN.
- Traditional neuroma management (traction neurectomy, burying the nerve in muscle/bone, capping, excision) has INCONSISTENT results and high recurrence because it does not give the nerve a physiologic target.
- TARGETED MUSCLE REINNERVATION (TMR) transfers the cut major nerve to a small, expendable MOTOR nerve of a nearby muscle - giving the regenerating axons 'somewhere to go and something to do', which prevents/treats neuroma and ALSO creates amplified myoelectric signals for intuitive PROSTHESIS control.
- REGENERATIVE PERIPHERAL NERVE INTERFACE (RPNI) implants the cut nerve end into an autologous FREE skeletal muscle graft, which the axons reinnervate - similarly providing a target (preventing neuroma) and a signal source for prosthetic control.
- Both are most effective done PROPHYLACTICALLY at the time of amputation, but also TREAT established symptomatic neuroma/phantom pain; systematic-review data show improvement in neuroma pain in roughly 75-100% and phantom limb pain in ~45-80% of patients, with complication rates around 13-31% (most often delayed wound healing).
- TMR and RPNI are now mainstream additions to amputation surgery and the surgical management of symptomatic neuromas; randomised, longer-term comparisons are still maturing.
- “The unifying principle: a cut nerve forms a neuroma when it has no target - TMR and RPNI both PROVIDE a target ('somewhere to go').
- “TMR = nerve transferred to a motor nerve of a muscle; RPNI = nerve buried in a free muscle GRAFT. Both also generate signals for myoelectric prostheses.
- “Do it PROPHYLACTICALLY at amputation for the best pain prevention - but they also work as treatment for established neuroma/phantom pain.
Traction neurectomy, burying in muscle/bone, capping, simple excision - the nerve still has no distal target, so axons sprout into a disorganised neuroma again. Results are inconsistent with high recurrence.
Both give the regenerating axons a physiologic target to reinnervate - a denervated muscle's motor nerve (TMR) or a free muscle graft (RPNI) - so they do not form a painful neuroma, and the reinnervated muscle generates myoelectric signals usable by a prosthesis.
The Problem: Neuroma & Phantom Limb Pain
When a peripheral nerve is transected (as in amputation or nerve injury) and the regenerating axons have no distal target to reinnervate, they sprout into a disorganised tangle - a neuroma - which forms a hypersensitive free nerve ending that can cause debilitating residual-limb (stump) pain and neuropathic symptoms. Amputees may additionally experience phantom limb pain. Together these are a major cause of pain, poor prosthesis use and disability after amputation, and no traditional technique has given consistent relief.
Targeted Muscle Reinnervation (TMR)
In TMR, the cut major (mixed) nerve is coapted (transferred) to a small, expendable motor nerve that supplies a nearby muscle (which is thereby reinnervated). This gives the regenerating axons a target to reinnervate ('somewhere to go and something to do'), so they do not form a neuroma. Originally developed to create additional myoelectric control sites for advanced prostheses, TMR was then found to prevent and treat neuroma and phantom limb pain as well. It is performed by (or with) a surgeon experienced in nerve transfers, commonly at the time of amputation or as a secondary procedure.
Eliminates the cut nerve's neuroma by redirecting axons into a functioning muscle; effective for both prevention (at amputation) and treatment of established neuroma/phantom pain.
Reinnervated muscle segments produce amplified, intuitive EMG signals that a myoelectric prosthesis can read - improving control (the original purpose of TMR).
Regenerative Peripheral Nerve Interface (RPNI)
In RPNI, the transected nerve end is implanted into an autologous free skeletal muscle graft (a small, devascularised piece of muscle that revascularises and is reinnervated by the implanted axons). The graft provides the axons with a target - preventing neuroma formation - and acts as a biological signal transducer that amplifies neural signals for prosthetic control. Because it uses a small free muscle graft rather than a nerve transfer, RPNI is technically simpler in some respects and can be used for multiple individual nerves/fascicles.
| 0 | 1 | 2 |
|---|---|---|
| What is done | Cut nerve coapted to a muscle's motor nerve (nerve transfer) | Cut nerve implanted into a free skeletal muscle graft |
| Target provided | Denervated nearby muscle (via its motor nerve) | Autologous free muscle graft |
| Main aims | Neuroma/phantom pain prevention + prosthesis control | Neuroma prevention/treatment + prosthesis signal |
| Best timing | At amputation (prophylaxis) or secondary | At amputation (prophylaxis) or secondary |
| Notes | Requires a suitable expendable motor nerve/target muscle | Uses a small free muscle graft; good for multiple nerve ends |
Evidence & Complications
A systematic review of TMR and RPNI for pain found that, for treatment of established pain, the techniques improved neuroma pain in about 75-100% of patients and phantom limb pain in about 45-80%, with average reductions of several points on pain scales. Used prophylactically at amputation, many patients reported no neuroma pain (48-100%) or no phantom limb pain (45-87%) at follow-up. Patient- reported outcome measures consistently favoured the techniques. Complication rates ranged from 13% to 31%, most commonly delayed wound healing. The evidence base is still maturing (mostly cohort studies with a small number of randomised data), so longer-term randomised comparisons are awaited.
TMR and RPNI are now mainstream adjuncts to amputation surgery and to the management of symptomatic neuromas, often involving collaboration between orthopaedic and plastic/peripheral-nerve surgeons. They should be considered at the time of amputation (prophylaxis) and offered for established, refractory neuroma or phantom pain. The choice between TMR and RPNI depends on the available targets, the number of nerves, and local expertise.
Evidence & Key Studies
Targeted muscle reinnervation and regenerative peripheral nerve interfaces for pain prophylaxis and treatment: a systematic review
- 17 studies (14 TMR, 366 patients; 3 RPNI, 75 patients): for treatment, TMR/RPNI improved neuroma pain in 75-100% and phantom limb pain in 45-80% of patients.
- Used prophylactically, many patients reported no neuroma pain (48-100%) or phantom limb pain (45-87%) at follow-up; PROMIS scores consistently improved.
- Complication rates 13-31% (most often delayed wound healing); randomised, longer-term comparisons with traditional management are still needed.
Regenerative peripheral nerve interfaces for the treatment and prevention of neuromas and neuroma pain
- A neuroma occurs when a regenerating transected nerve has no distal target, producing a hypersensitive painful nerve ending; no traditional technique gives consistent results.
- RPNI implants the transected nerve into an autologous free skeletal muscle graft, providing a physiologic target.
- Early clinical studies show promising results for RPNI in both treating and preventing symptomatic neuromas.
According to PubMed, the outcome figures and complication rates come from the cited systematic review, and the RPNI rationale/technique from the cited Hand Clinics review. (See also our Foot & Ankle Amputation Levels topic for amputation principles.)
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Why do amputees develop neuroma pain, and how do targeted muscle reinnervation and regenerative peripheral nerve interfaces address it? How do they differ?”
“What does the evidence show for TMR and RPNI, what are the main complications, and how would you use them in practice?”
Mnemonics & Memory Aids
TARGET
Hook:Give the nerve a TARGET: TMR (motor nerve) or RPNI (muscle graft).
TMR-vs-RPNI
Hook:TMR transfers to a motor nerve; RPNI implants into a muscle graft.
The problem
- Cut nerve with no target -> neuroma (painful disorganised bulb) + phantom limb pain
- Traditional methods (traction neurectomy, bury, cap) inconsistent, recur
- Solution: give the nerve a physiologic target
TMR
- Cut major nerve coapted to a small expendable MOTOR nerve of a nearby muscle
- Originally for myoelectric prosthesis control; also prevents/treats pain
- Needs a suitable target muscle/motor nerve
RPNI
- Cut nerve end implanted into an autologous FREE skeletal muscle graft
- Provides target + amplifies signal for prosthesis
- Useful for multiple nerve ends; technically simpler in some respects
Evidence & use
- Neuroma pain improved ~75-100%; phantom pain ~45-80% (systematic review)
- Complications ~13-31% (mostly delayed wound healing)
- Best done prophylactically at amputation; also treats refractory neuroma; evidence maturing