Vertebral Artery Injury in Cervical Trauma
More than half of VAIs are clinically silent at presentation, yet untreated they cause stroke in 10–40% with the risk peaking in the first 24 hours. Don't wait for symptoms - screen by injury pattern (foramen-transversarium fracture, facet dislocation, C1–C3) with CTA.
Closed reduction or operative manipulation of a high-risk cervical injury can propagate a dissection. Screen with CTA where feasible and coordinate antithrombotic timing with the spinal plan - without unduly delaying urgent reduction of a cord-threatening injury.
Overview & Epidemiology
Vertebral artery injury is one half of blunt cerebrovascular injury (BCVI) - blunt trauma to the carotid or vertebral arteries. It matters because it is a potentially preventable cause of posterior-circulation (vertebrobasilar) stroke: the diagnosis is made on imaging, not symptoms, and early antithrombotic therapy markedly reduces both stroke and death (EAST: stroke odds ratio 0.20, mortality odds ratio 0.17). Detection rises sharply when a screening protocol is used (odds ratio ~4.7) and is far higher among high-risk cervical injuries than low-risk ones (odds ratio ~12.7). The whole topic is therefore an argument for structured early screening of the right cervical-trauma patients.
Pathophysiology & Anatomy
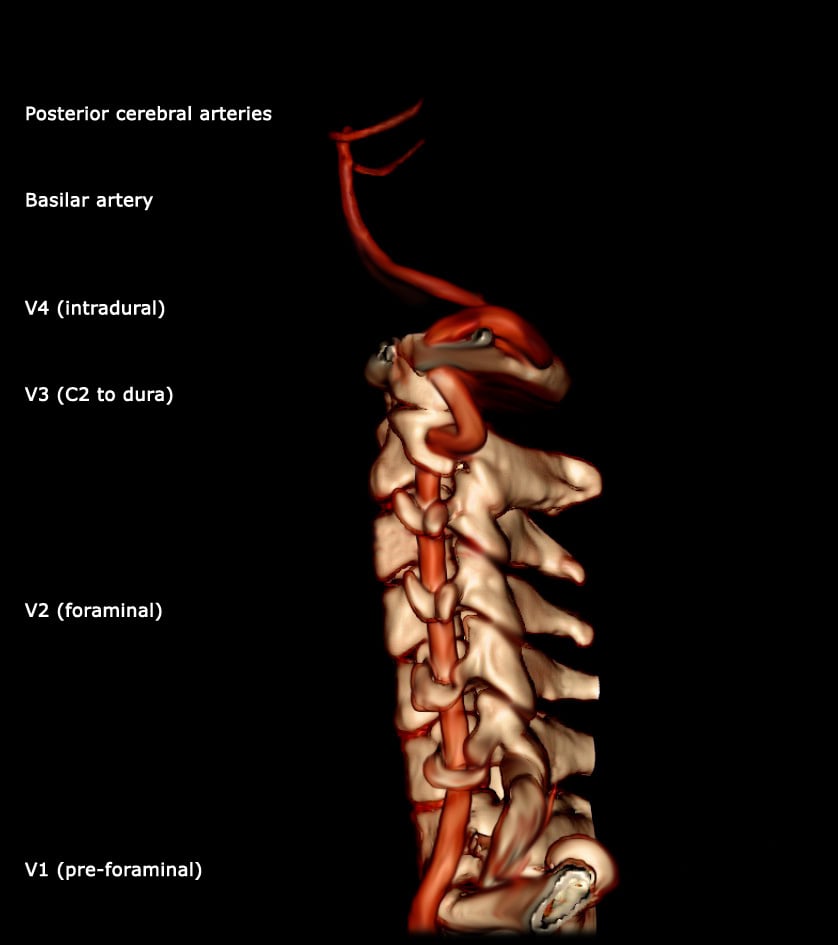
The vertebral artery has four segments: V1 (pre-foraminal) from the subclavian to C6; V2 (foraminal) ascending through the transverse foramina from C6 to C2; V3 (extraspinal) from C2, looping around the atlas to pierce the dura; and V4 (intradural), joining its fellow to form the basilar artery. The V2 segment's bony, enclosed course through the transverse foramina, and the mobile V3 loop at the craniocervical junction, are what make the artery vulnerable in cervical trauma: a fracture that breaches the foramen transversarium, a facet dislocation/subluxation, a distraction injury, or an upper cervical fracture can stretch, compress or tear the vessel — causing intimal injury, dissection, thrombosis, pseudoaneurysm or occlusion.
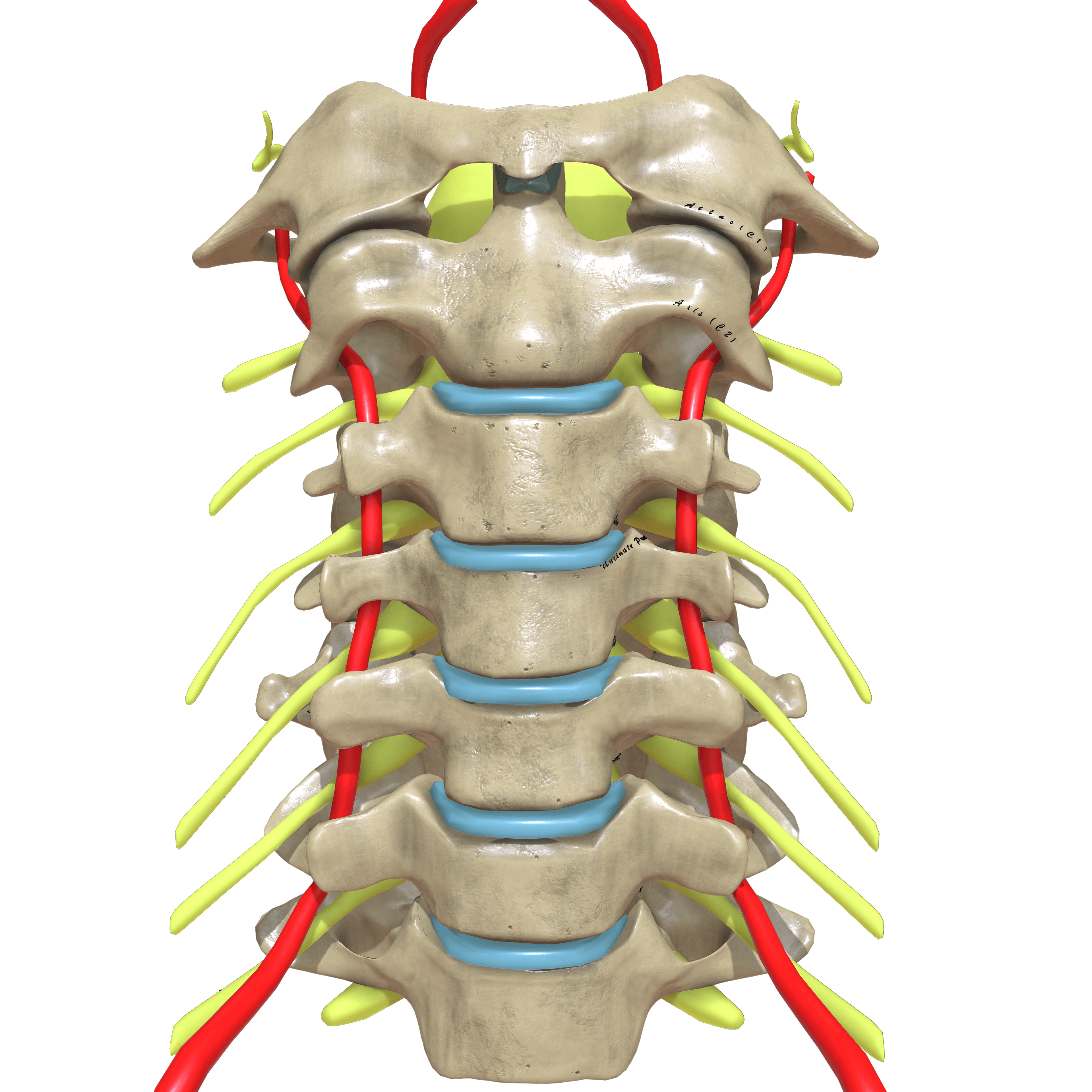
The reason an isolated unilateral VAI often does not cause a stroke is collateral flow: the two vertebral arteries unite to form the single basilar artery, and the posterior communicating arteries link the posterior (vertebrobasilar) to the anterior (carotid) circulation through the Circle of Willis - so the contralateral VA and the carotid system can still perfuse the territory if one VA occludes. This tolerance is conditional, and the exceptions are what make an injury dangerous: when the injured vessel is the dominant vertebral artery (one VA - often the left - is usually larger, and the contralateral may be hypoplastic or end in PICA without reaching the basilar), when both vertebral arteries are injured, or when thrombus embolises distally into the basilar/PICA territory rather than simply occluding locally. This is why an isolated, non-dominant grade IV occlusion is often tolerated on aspirin, whereas a dominant-artery or bilateral injury - or any embolic propagation - is far more dangerous, and why antithrombotics (which prevent embolism) matter even when flow looks preserved.
Clinical Presentation
The defining clinical feature of VAI is that it is commonly asymptomatic at first - more than half of patients have no neurological signs at presentation, so the injury is found on screening imaging rather than examination. When it does declare, it produces a posterior-circulation (vertebrobasilar) stroke or TIA: vertigo, ataxia, diplopia, dysarthria, visual-field loss, or a depressed conscious level - often a day or more after the injury. Other clues are local: neck pain, a cervical bruit or thrill, or an expanding neck haematoma. The teaching point for the exam is blunt: a normal neurological examination does not exclude VAI, and the window to prevent the stroke is in the first hours.
When VAI does cause a posterior-circulation infarct, expect recognisable patterns rather than vague "dizziness":
- Lateral medullary (Wallenberg) syndrome - the classic VA/PICA-territory stroke: ipsilateral facial pain/temperature loss, Horner's syndrome, ataxia, vertigo/nystagmus and bulbar signs (dysphagia, hoarseness), with contralateral body pain/temperature loss - a "crossed" sensory pattern.
- Basilar artery occlusion - the catastrophic end: fluctuating or reduced consciousness, quadriparesis and cranial-nerve signs, the locked-in syndrome - a time-critical neurological emergency.
- Cerebellar infarction - vertigo, ataxia and vomiting; the danger is that a large cerebellar infarct swells, compressing the fourth ventricle and brainstem and causing obstructive hydrocephalus, which can require suboccipital decompressive craniectomy with or without an external ventricular drain.
Recognising these as the consequence of an untreated VAI is what links the silent injury to the urgent screen.
Investigations: Screening & Grading
Because BCVI is frequently clinically silent initially, screening is based on injury patterns and risk factors (modified Denver/Memphis-type criteria). Screen for VAI/BCVI with:
- Cervical spine fractures — especially through the foramen transversarium, C1–C3 fractures, and facet (sub)luxation/dislocation or fracture-subluxation;
- Severe head injury (low GCS), basilar skull fracture, Le Fort II/III facial fractures;
- Cervical bruit/thrill, expanding neck haematoma, seatbelt sign over the neck, or near-hanging;
- Focal neurology unexplained by brain imaging, or a stroke/TIA pattern.
A pragmatic rule (and the EAST practice guideline position): screen any patient whose injuries would otherwise prompt a CT of the neck or chest — liberal screening catches the silent majority.
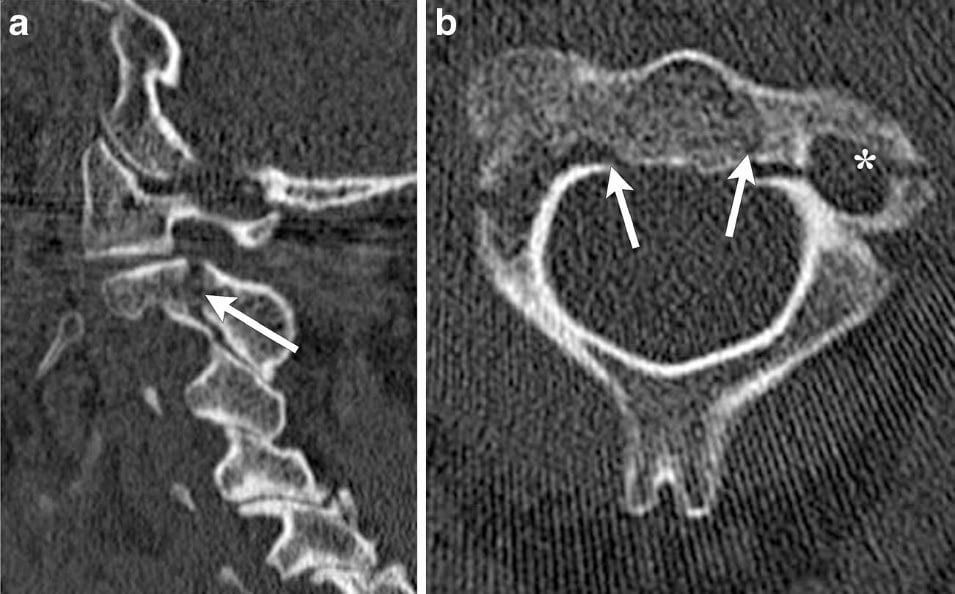
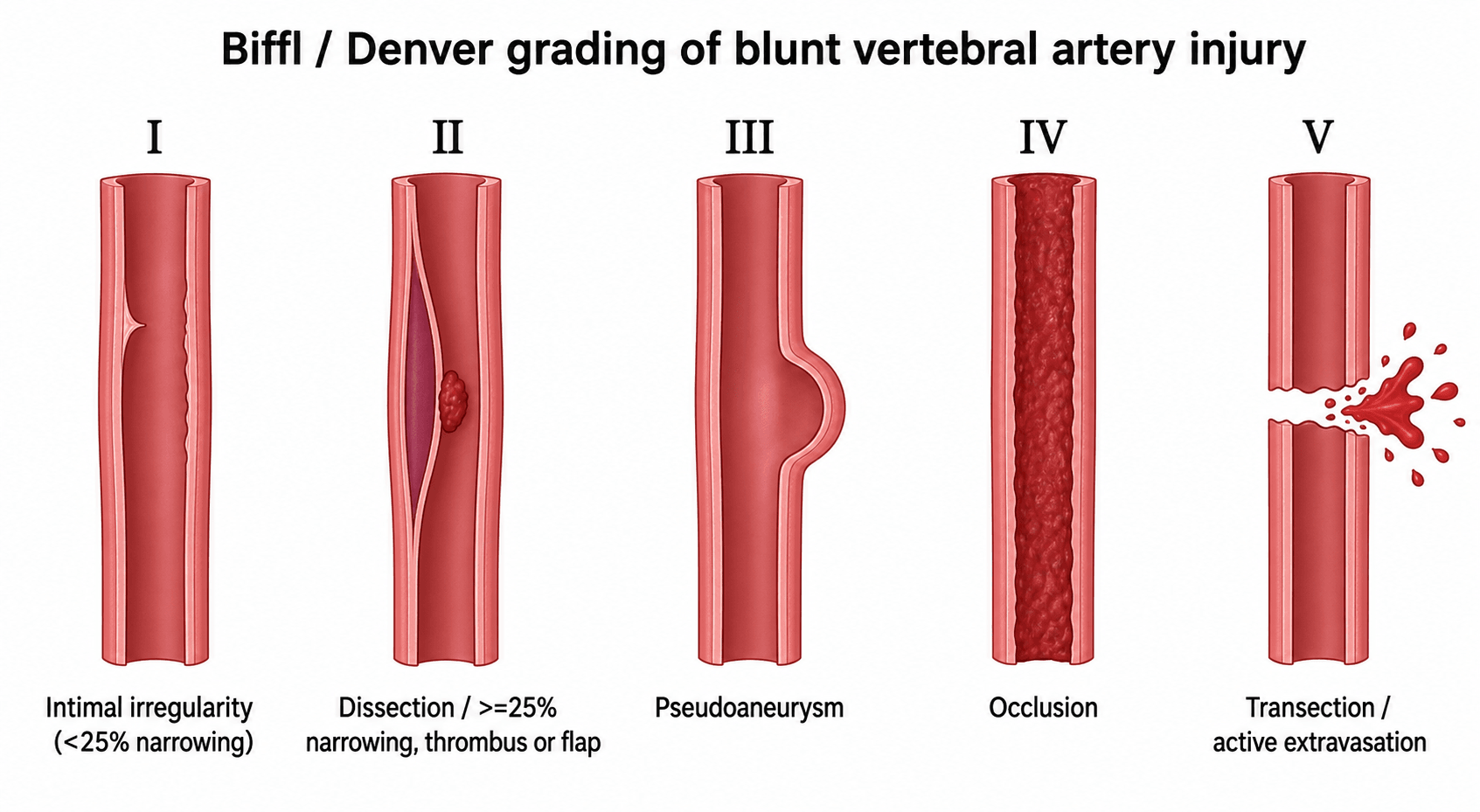
CT angiography (CTA) of the neck is the screening modality of choice (widely available, fast); digital subtraction angiography (DSA) remains the reference standard and is used in selected/equivocal cases or for intervention. Injuries are graded by the Biffl/Denver scale (I–V), which guides treatment and prognosis, and follow-up imaging is often used to track lesion evolution.
- Lesion
- Intimal irregularity / dissection with under 25% luminal narrowing
- Lesion
- Dissection or intramural haematoma with 25% or more narrowing, intraluminal thrombus, or a raised intimal flap
- Lesion
- Pseudoaneurysm
- Lesion
- Complete occlusion
- Lesion
- Transection with active extravasation (or AV fistula in some schemes)
Management
The goal is stroke prevention. Antithrombotic therapy — aspirin or therapeutic anticoagulation (heparin) — is the mainstay and has proven safety in trauma patients; treatment is guided by the grade of injury and started as early as the overall injury burden safely allows (given the early stroke window). For isolated vertebral artery injury the stroke rate is low and aspirin is generally effective (particularly for grade I and IV). Endovascular intervention (stent, coil/occlusion) is reserved for selected lesions — e.g. an enlarging pseudoaneurysm (grade III) or a grade V injury (the EAST guideline recommends against routine stenting as an adjunct to antithrombotics for grade II–III). The choice of agent and timing is individualised by balancing stroke risk against bleeding risk (concomitant TBI, solid-organ injury, planned surgery).
Aspirin or therapeutic anticoagulation is the core treatment and reduces both stroke and mortality. Start as early as the injury burden allows; for isolated VAI the stroke rate is low and aspirin is generally effective (especially grades I and IV). Balance against bleeding risk (TBI, solid-organ injury, surgery) and arrange follow-up imaging for grade II/III lesions, which can progress.
- Lesion
- Intimal irregularity / under 25% narrowing
- Typical management
- Antithrombotic (often aspirin); usually resolves
- Lesion
- Dissection/haematoma ≥25% narrowing, thrombus, intimal flap
- Typical management
- Antithrombotic; follow-up imaging (can progress)
- Lesion
- Pseudoaneurysm
- Typical management
- Antithrombotic; endovascular if enlarging/symptomatic
- Lesion
- Occlusion
- Typical management
- Antithrombotic (aspirin); monitor for posterior-circulation stroke
- Lesion
- Transection / active extravasation
- Typical management
- Endovascular/surgical control (often vessel occlusion)
- 1Suspect by patternForamen-transversarium fracture, facet (sub)luxation/dislocation, distraction injury, or C1–C3 fracture — plus the broader Denver criteria. A normal neuro exam does not exclude VAI.
- 2Screen early with CTACT angiography of the neck is the screening test of choice; DSA for equivocal cases or intervention. Screen within the first hours — stroke risk peaks at 24 h.
- 3Grade and start antithromboticsGrade with Biffl/Denver. Start aspirin or therapeutic anticoagulation as soon as the overall injury burden allows; isolated VAI does well on aspirin (esp. grades I and IV).
- 4Think of the vessel before you reduceManipulation/closed reduction can propagate a dissection — screen where feasible and coordinate antithrombotic timing with the spinal plan, without unduly delaying urgent reduction of a cord-threatening injury.
In a high-risk cervical injury (facet dislocation, foramen-transversarium fracture), remember the vertebral artery when planning closed reduction or operative manipulation — screen with CTA where feasible and weigh the small risk of propagating a dissection, while not unduly delaying urgent reduction of a cord-threatening injury. Coordinate antithrombotic timing with the spinal surgical plan and any associated injuries.
Complications & Prognosis
- Detail
- The dominant complication: 10-40% untreated, risk highest in the first 7 days and peaking within 24 hours - the reason for urgent screening and treatment
- Detail
- Grade II dissections/haematomas can progress despite therapy; pseudoaneurysms (III) may enlarge - hence follow-up imaging
- Detail
- Grade I often resolves; grade IV occlusion does not recanalise early but isolated VAI still has a low stroke rate on aspirin; grade V is the most dangerous
- Detail
- Antithrombotics must be balanced against TBI, solid-organ injury and planned surgery - though they are proven safe in trauma overall
- Detail
- Early antithrombotic therapy substantially reduces stroke and mortality (EAST: stroke OR 0.20, mortality OR 0.17)
Mnemonics & Memory Aids
ARTERYThe artery at risk
Hook:The ARTERY at risk: at-risk patterns, runs in V2/V3, time-critical, CTA, reduce risk with antithrombotics.
SCREENWho to screen
Hook:SCREEN for VAI by pattern, not symptoms: Spine pattern, Cervical signs, Reduced GCS, Established neuro, Everyone needing CT neck/chest, Near-hanging.
I to VBiffl/Denver grades
Hook:Biffl I-V: intimal, narrowing/dissection, pseudoaneurysm, occlusion, transection.
Viva practice
Practise clinical reasoning and management decisions out loud
“A patient with a cervical facet dislocation and a fracture through the foramen transversarium is neurologically intact. Why are you concerned about the vertebral artery, who would you screen, and how?”
“CTA confirms a grade II vertebral artery dissection with 30% narrowing. How would you manage it, and how does treatment vary by grade? What if you also need to reduce the cervical injury?”
Anatomy & risk
- V1 pre-foraminal, V2 foraminal (transverse foramina), V3 atlas loop, V4 intradural to basilar
- V2/V3 most at risk; injures posterior (vertebrobasilar) circulation
- At-risk injuries: foramen transversarium fracture, facet (sub)luxation, distraction, C1-C3 fracture
Why it matters
- Blunt cerebrovascular injury to stroke in 10-40% if untreated
- More than half SILENT initially; stroke risk peaks first 24h (highest first 7 days)
- Screen early - don't wait for symptoms
Screen & grade
- CTA neck = screening modality of choice (DSA reference standard in select cases)
- Screen Denver-type criteria + anyone needing CT neck/chest
- Biffl/Denver grades I-V guide treatment
Management
- Antithrombotics (aspirin or anticoagulation) = mainstay, safe in trauma; grade-guided
- Isolated VAI: low stroke rate, aspirin effective (esp. I, IV); follow-up imaging for II
- Endovascular for enlarging pseudoaneurysm (III)/grade V; not routine stenting II-III; consider vessel before cervical reduction
Evidence
Blunt carotid arterial injuries: implications of a new grading scale
- Derived the Biffl/Denver I-V grading scale from 76 patients with 109 blunt arterial injuries, with prognostic and therapeutic implications.
- Grade-specific behaviour: two-thirds of grade I healed regardless of therapy; grade II progressed in ~70% despite heparin; only 8% of grade III pseudoaneurysms healed with heparin but 89% resolved after stenting; grade IV occlusions did not recanalise; grade V transections were lethal.
- Stroke risk increased with injury grade - the basis for grade-guided treatment.
Evaluation and management of blunt cerebrovascular injury: A practice management guideline from the Eastern Association for the Surgery of Trauma
- GRADE-based systematic review/meta-analysis (23 studies): a screening protocol increased BCVI detection (OR 4.74), and high-risk cervical injuries had far higher detection than low-risk (OR 12.7).
- Antithrombotic therapy reduced stroke (OR 0.20) and mortality (OR 0.17) versus no antithrombotic therapy.
- Recommends screening protocols, CTA for high-risk cervical injuries, antithrombotic therapy for diagnosed BCVI, and AGAINST routine stenting as an adjunct to antithrombotics for grade II-III injuries.
Management of Blunt Cerebrovascular Injury
- Untreated BCVI causes stroke in 10-40% of patients, but more than half do not present with stroke symptoms initially; stroke risk is highest in the first 7 days (peak in the first 24 hours).
- CT angiography is the screening modality of choice (DSA in selected cases); screen all patients with injuries that would otherwise prompt CT of the neck or chest.
- Antithrombotic therapy is the mainstay and is safe in trauma patients; endovascular intervention benefits selected patients; treatment is guided by injury grade.
Blunt Traumatic Vertebral Artery Injuries: Incidence, Therapeutic Management, and Outcomes
- 156 isolated blunt vertebral artery injuries: most patients (135/156) were treated with aspirin alone; the risk of stroke after cervical vertebral artery injury was low.
- Aspirin prophylaxis was efficacious in grade I and grade IV injuries; data are limited for grades II and III.
- The three strokes that occurred were detected within 24 hours of admission, before treatment was started - reinforcing early screening and treatment.
The I-V grading scale comes from Biffl et al. 1999 (DOI); the screening and antithrombotic recommendations (and the detection/stroke/mortality odds ratios) from the EAST practice guideline (Kim et al. 2020, DOI); the stroke-risk figures and CTA-screening synthesis from Stone et al. 2018 (DOI); and the isolated-vertebral-artery outcomes from Zeineddine et al. 2022 (DOI). The segmental vertebral-artery anatomy is standard, well-established reference. (See also our cervical-trauma topics.)