Bifurcate Ligament Avulsion | Lateral Foot Pain | Usually Conservative
- Anterior process calcaneus fracture = bifurcate ligament avulsion injury (calcaneonavicular and calcaneocuboid ligaments)
- Conservative management effective
- “Bifurcate ligament avulsion = calcaneonavicular and calcaneocuboid ligaments
- “Usually conservative treatment - most heal with immobilization
- “Often misdiagnosed as ankle sprain - look carefully on lateral X-ray
- “Excision for small symptomatic fragments if conservative fails
Bifurcate ligament avulsion - Anterior process is attachment site for bifurcate ligament (calcaneonavicular and calcaneocuboid ligaments). Forced inversion and plantarflexion causes avulsion.
Most heal with conservative treatment - Immobilization with cast or boot, non-weight bearing for 4-6 weeks. Surgery rarely needed. Excision for small symptomatic fragments if conservative fails.
Often misdiagnosed as ankle sprain - Similar mechanism and symptoms. High index of suspicion needed for lateral foot pain. Look carefully on lateral X-ray.
Surgery rarely needed - Only if large displaced fragment or persistent symptomatic nonunion. ORIF for large fragments, excision for small symptomatic fragments.
- Description
- Extra-articular (small / larger)
- First-line treatment
- Conservative or functional
- Comment
- Good-to-excellent in the majority
- Description
- Intra-articular, non-displaced
- First-line treatment
- Conservative; confirm with CT
- Comment
- Highest complication rate if missed
- Description
- Intra-articular, displaced
- First-line treatment
- ORIF (or excision)
- Comment
- Protect calcaneocuboid joint
BIFURCATEAnterior Process Features
Hook:BIFURCATE: Bifurcate ligament avulsion, Inversion mechanism, Foot pain, Usually conservative, Rarely surgical, Calcaneus anterior process, Avulsion injury, Treatment conservative, Excision if needed!
Overview and Epidemiology
Anterior process calcaneus fractures are rare injuries involving the anterior process of the calcaneus, which serves as the attachment site for the bifurcate ligament. These fractures are usually treated conservatively and are often misdiagnosed as ankle sprains.
Definition
Anterior process calcaneus fracture: Fracture of the anterior process of the calcaneus, which:
- Serves as attachment site for bifurcate ligament
- Forms part of calcaneocuboid joint
- Rare but important injury
Bifurcate ligament:
- Calcaneonavicular ligament: From anterior process to navicular
- Calcaneocuboid ligament: From anterior process to cuboid
- Function: Stabilises midfoot
- Avulsion: Forced inversion and plantarflexion causes avulsion
Epidemiology
- Incidence: Less than 1% of calcaneus fractures
- Age: Peak 20-40 years (sports, trauma)
- Gender: No clear predominance
- Mechanism: Forced inversion and plantarflexion (similar to ankle sprain)
- Associated injuries: Ankle sprains, other foot injuries
Bifurcate ligament avulsion - Anterior process is attachment site for bifurcate ligament (calcaneonavicular and calcaneocuboid ligaments). Forced inversion and plantarflexion causes avulsion. Usually treated conservatively.
Anatomy and Pathophysiology
Anterior Process Anatomy
Anterior process of calcaneus:
- Location: Anterior aspect of calcaneus
- Function: Attachment site for bifurcate ligament
- Articulation: Forms part of calcaneocuboid joint
- Size: Variable, typically 1-2cm
Bifurcate ligament:
- Calcaneonavicular ligament: From anterior process to navicular
- Calcaneocuboid ligament: From anterior process to cuboid
- Function: Stabilises midfoot, prevents excessive motion
- Avulsion: Forced inversion and plantarflexion causes avulsion
Calcaneocuboid joint:
- Articulation: Calcaneus and cuboid
- Anterior process: Part of joint
- Function: Lateral column stability
Pathophysiology
Injury mechanism:
- Forced inversion and plantarflexion: Classic mechanism (similar to ankle sprain)
- Bifurcate ligament tension: Excessive tension on bifurcate ligament
- Avulsion: Ligament avulses from anterior process with bone fragment
Why often missed:
- Similar to ankle sprain: Same mechanism and symptoms
- Subtle on X-ray: May be obscured or overlooked
- Misdiagnosis: Often diagnosed as ankle sprain
Why usually conservative:
- Small fragment: Usually small, non-displaced
- Good healing: Most heal with immobilization
- Low demand: Anterior process has low functional demand
Two Mechanisms: Avulsion vs Compression (Impaction)
The topic's default teaching — forced inversion and plantarflexion producing a bifurcate-ligament avulsion — accounts for the common small, extra-articular apex fragment (modified Degan type I/II). It does not, however, explain why some anterior process fractures are large, comminuted and intra-articular (type IIIA/IIIB). Trnka and colleagues noted that more than one mechanism has been described, and the two-mechanism model resolves this apparent contradiction.
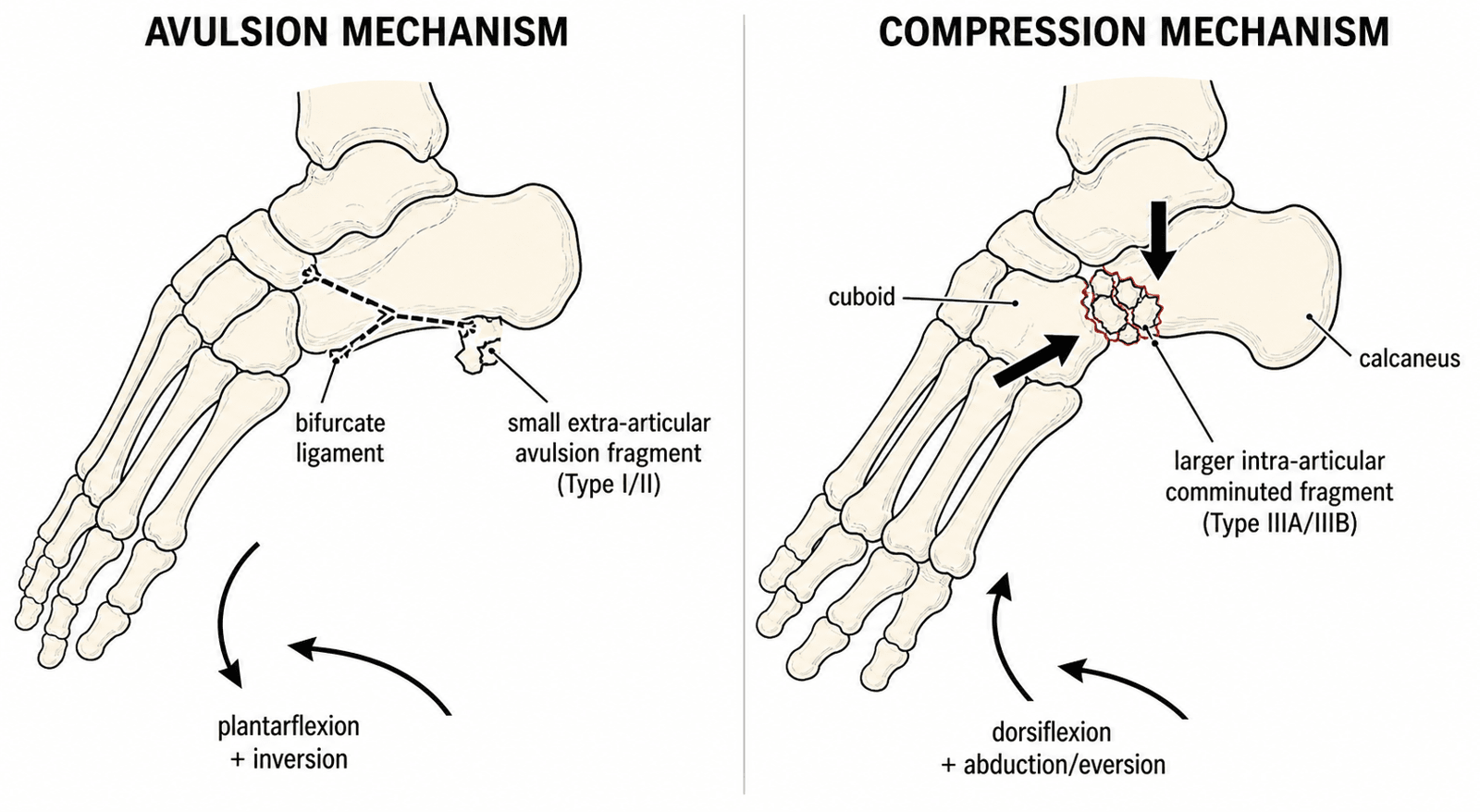
Avulsion mechanism (the common one)
- Forces: forced plantarflexion combined with inversion (supination/adduction).
- What happens: the bifurcate ligament (calcaneonavicular + calcaneocuboid limbs) tightens and avulses its bony origin from the dorsal anterior process.
- Result: a small, extra-articular flake at the apex of the process — Degan type I/II — that typically heals with functional or conservative care.
Compression / impaction mechanism ("the other pattern")
- Forces: forced dorsiflexion with forefoot abduction/eversion (a pronation-abduction pattern), driving the anterior process against the cuboid and talar head.
- What happens: the anterior process is crushed rather than pulled off — a shear/impaction injury of the process itself.
- Result: a larger, often comminuted, intra-articular fragment (Degan type IIIA/IIIB) that involves the calcaneocuboid articular surface and is the group most likely to need CT and, when displaced, ORIF. This mechanism is consistent with Massen's cohort, in which 82% of fractures were comminuted and 78% had concomitant Chopart-line injury — findings that fit a higher-energy compression/midtarsal loading pattern rather than a pure ligamentous avulsion.
Why this matters clinically
Recognising which mechanism produced the injury predicts the fracture morphology and the treatment lane: an avulsion history points to a small extra-articular fragment treated functionally, whereas a dorsiflexion/abduction crush should raise suspicion of an intra-articular fragment and prompt CT to assess the calcaneocuboid joint.
Two mechanisms, two fracture patterns. Plantarflexion + inversion → bifurcate-ligament avulsion → small extra-articular type I/II flake. Dorsiflexion + forefoot abduction/eversion → compression/impaction of the process against the cuboid → larger, comminuted intra-articular type IIIA/IIIB fragment. Do not confuse this with the cuboid "nutcracker" fracture (cuboid crushed between the calcaneus and the metatarsal bases), which is a separate lateral-column injury.
Classification Systems
Degan and Modified Degan Classification
The original Degan classification (Degan, JBJS Am 1982) was modified by Cibura et al. (BMC Musculoskelet Disord 2022) to subdivide the intra-articular type III into displaced and non-displaced subgroups, because the displaced subgroup is the one that most often needs surgery.
Type I: Small extra-articular fracture of the apex of the anterior process. Conservative / functional treatment.
Type II: Larger extra-articular fracture without calcaneocuboid joint involvement. Conservative / functional treatment.
Type IIIA: Large intra-articular fragment, non-displaced (no joint step-off). Conservative, but CT is advised — missed type IIIA fractures had the highest complication rate in Cibura's series.
Type IIIB: Large intra-articular fragment, displaced with calcaneocuboid step-off. Most likely to require ORIF (or excision for unreconstructable fragments).
Note: Massen et al. (Injury 2019) found fracture type did NOT predict functional outcome, so classification informs the surgical decision more than the prognosis.
Clinical Assessment
History
Symptoms:
- Lateral foot pain: Pain on lateral side of foot
- Swelling: Localised to lateral foot
- Difficulty weight bearing: Pain with weight bearing
- Mechanism: Forced inversion and plantarflexion (similar to ankle sprain)
Risk factors:
- Sports with inversion injuries
- High-energy trauma
- Ankle sprain mechanism
Physical Examination
Inspection:
- Swelling on lateral foot
- Ecchymosis (may be delayed)
- Deformity (rare)
Palpation:
- Tenderness over anterior process (anterior to lateral malleolus)
- Calcaneocuboid joint tenderness
- Ankle joint usually not tender
Range of Motion:
- Ankle ROM may be limited
- Midfoot ROM may be limited
- Inversion/eversion painful
Special tests:
- Anterior process palpation: Tenderness over anterior process
- Calcaneocuboid joint stress: Pain with stress
Differential Diagnosis
The classic trap is the "lateral ankle sprain that will not settle." Focal tenderness about 2 cm distal and anterior to the tip of the lateral malleolus (over the anterior process / calcaneocuboid joint) should redirect the differential.
- Mechanism / Clue
- Forced inversion + plantarflexion
- Key Tenderness
- Anterior process / calcaneocuboid joint
- Distinguishing Feature
- Irregular non-corticated fragment; oblique X-ray or CT positive
- Mechanism / Clue
- Inversion in plantarflexion
- Key Tenderness
- Anterior to lateral malleolus (ATFL)
- Distinguishing Feature
- Anterior drawer positive; normal foot films
- Mechanism / Clue
- None (incidental ossicle)
- Key Tenderness
- Usually asymptomatic
- Distinguishing Feature
- Smooth corticated margins; often bilateral; up to 5% prevalence
- Mechanism / Clue
- Inversion; peroneus brevis pull
- Key Tenderness
- Base of 5th metatarsal
- Distinguishing Feature
- Tenderness at styloid; proximal transverse line
- Mechanism / Clue
- Adolescent, recurrent sprains
- Key Tenderness
- Sinus tarsi / dorsolateral midfoot
- Distinguishing Feature
- Anteater-nose sign on lateral X-ray; CT confirms bar
- Mechanism / Clue
- Axial load / snowboarder mechanism
- Key Tenderness
- Cuboid or lateral talar process
- Distinguishing Feature
- Different tender point; CT localises
High index of suspicion needed - Anterior process fractures are often misdiagnosed as ankle sprains. Look carefully on lateral X-ray. Tenderness over anterior process (anterior to lateral malleolus) is key finding.
Investigations
Standard X-ray Protocol
Lateral view (best view):
- Shows anterior process
- Look carefully - often subtle
- May be obscured by overlapping structures
Oblique view:
- May show fracture better
- Calcaneocuboid joint view
AP view:
- May show fracture
- Less reliable than lateral
Key point: Often missed on initial X-rays - high index of suspicion needed.


MISSDiagnosis
Hook:MISS: Misdiagnosed as ankle sprain, Inversion mechanism, Suspicion needed, Sprain-like symptoms!
Role of MRI and Bone Scintigraphy
The Investigations section covers plain films and CT, but two clinical problems this topic itself raises are answered better by MRI — the acutely painful foot with normal or equivocal radiographs, and the corticated density that could be a fracture or a calcaneus secundarius.
When MRI adds value
- Occult fracture with normal X-rays: anterior process fractures are subtle and frequently missed. Where clinical suspicion is high but films are normal and CT is unavailable or negative for a cortical break, MRI shows bone-marrow oedema and a hypointense fracture line, confirming an acute injury.
- Fracture vs accessory ossicle (acuity, not just shape): CT best shows margin corticication, but MRI adds the physiological answer — an acute fracture has surrounding marrow oedema, whereas an asymptomatic calcaneus secundarius has a quiescent, corticated, oedema-free ossicle. This complements the margin-based distinction (irregular non-corticated fracture vs smooth corticated ossicle) used on plain films and CT.
- Associated soft-tissue and osteochondral injury: because the same inversion/midtarsal mechanism injures the bifurcate ligament and the wider Chopart line (concomitant in a large proportion of cohorts), MRI can demonstrate bifurcate/calcaneocuboid ligament tears, osteochondral lesions and other midtarsal injuries that plain films miss and that flag a higher-risk, slower-recovering injury.
Bone scintigraphy — historical / adjunct role
A technetium bone scan is sensitive but non-specific: focal anterior-process uptake supports an occult acute fracture when cross-sectional imaging is unavailable, but it cannot characterise fragment size, displacement or joint involvement. In modern practice CT (for bony detail and surgical planning) and MRI (for acuity and soft tissue) have largely superseded it.
X-ray/oblique = first-line, easily missed; CT = fragment size, displacement, calcaneocuboid joint involvement and surgical planning (Cibura advises CT for any clinical suspicion); MRI = occult fracture on normal films, marrow oedema to confirm an acute fracture versus a quiescent calcaneus secundarius, and associated bifurcate/Chopart ligament or osteochondral injury. A systematic foot-and-ankle imaging approach is developed in the imaging-ankle-foot topic.
Management Algorithm
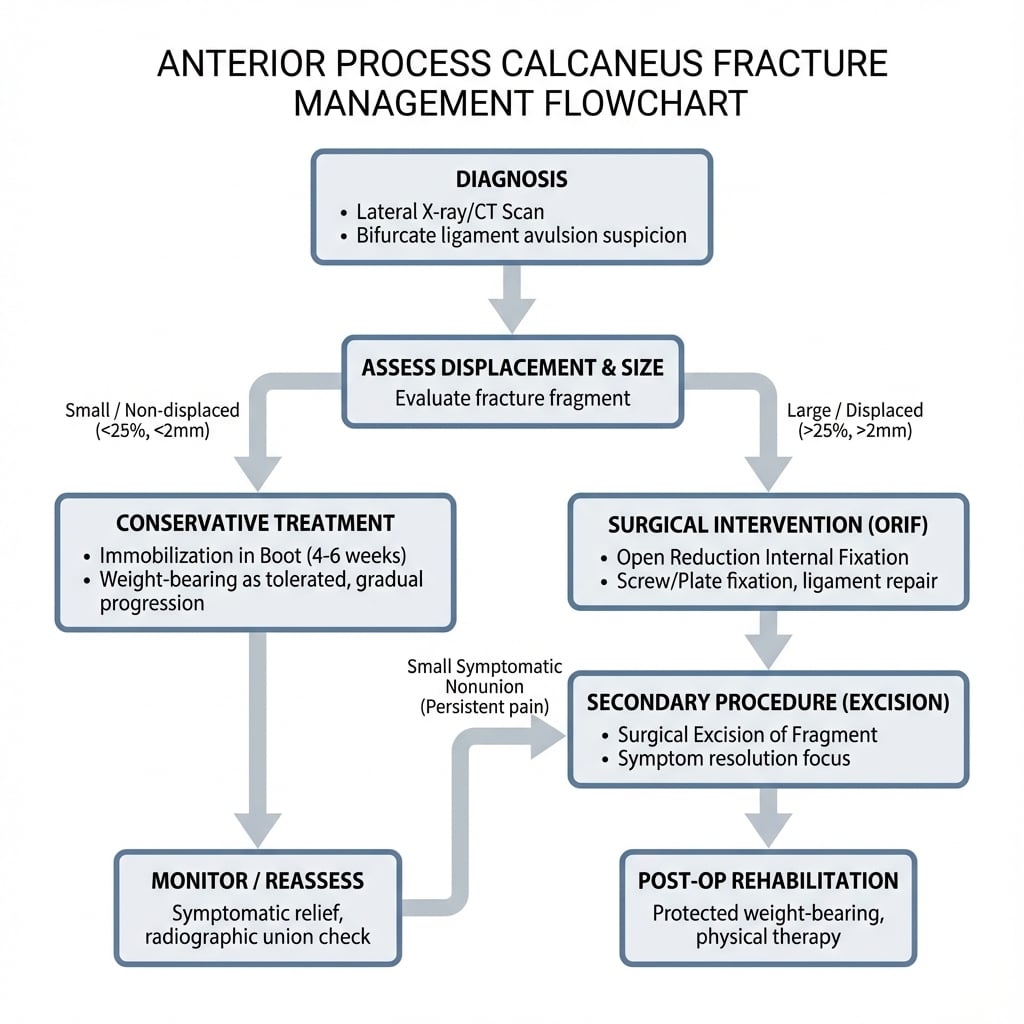
Management Pathway
Anterior Process Calcaneus Fracture Management
Often misdiagnosed as ankle sprain - look carefully on lateral X-ray. CT recommended if suspected clinically but X-ray negative. Tenderness over anterior process is key finding.
Most fractures do well with conservative or functional treatment — cast/boot with protected weight-bearing, or immediate full weight-bearing for non-displaced fractures (Massen, Injury 2019). Good-to-excellent results in the majority.
Surgery is reserved for displaced intra-articular (type IIIB) fragments (ORIF to protect the calcaneocuboid joint) or persistent symptomatic nonunion.
Excision is appropriate for a small symptomatic fragment with established nonunion; it relieves pain and is preferable to unreliable fixation of a tiny fragment (Degan, JBJS Am 1982).
CONSERVATIVETreatment Decision
Hook:CONSERVATIVE: Conservative first-line, Often heals, Non-weight bearing, Small fragments excision, Excision if needed, Rarely surgical, Very rare indication, Avulsion injury, Treatment conservative, Immobilization, Very good outcomes, Excellent prognosis!
Surgical Technique
ORIF Technique (For Large Fragments)
Indications:
- Large fragment (over 25% of process)
- Displaced (greater than 2mm)
- Calcaneocuboid joint instability
Approach:
- Lateral approach to anterior process
- Expose fragment
- Protect peroneal tendons
Technique:
- Exposure: Lateral approach to anterior process
- Reduction: Anatomic reduction of fragment
- Fixation: Lag screws (2.0-2.7mm) or mini-fragment screws
- Verification: Confirm reduction and hardware position fluoroscopically
Advantages:
- Preserves calcaneocuboid joint
- Prevents nonunion
- Better outcomes than excision for large fragments
ORIF for large displaced fragments.
Complications
- Incidence
- 5-10%
- Risk Factors
- Displacement, inadequate immobilization
- Prevention/Management
- Adequate immobilization, ORIF if needed
- Incidence
- 10-15%
- Risk Factors
- Nonunion, fragment size
- Prevention/Management
- Excision if symptomatic
- Incidence
- ~30% (Cibura 2022)
- Risk Factors
- Similar to ankle sprain
- Prevention/Management
- High index of suspicion, CT if needed
- Incidence
- 5-10%
- Risk Factors
- Malunion, joint involvement
- Prevention/Management
- Anatomic reduction
Nonunion
5-10% incidence:
- Cause: Displacement, inadequate immobilization
- Prevention: Adequate immobilization, ORIF if needed
- Management: Excision if symptomatic, ORIF if large fragment
Persistent Pain
10-15% incidence:
- Cause: Nonunion, fragment size, joint involvement
- Prevention: Adequate treatment, anatomic reduction
- Management: Excision if symptomatic, activity modification
Postoperative Care
Immediate Postoperative
- Immobilisation: Short leg cast or boot
- Weight bearing: Non-weight bearing (4-6 weeks)
- ROM: Ankle ROM after cast removal
- PT: Midfoot ROM and strengthening
Rehabilitation Protocol
Weeks 0-4:
- Short leg cast, non-weight bearing
- Elevation to reduce swelling
- Ankle ROM exercises (if stable)
Weeks 4-6:
- Cast removal
- Transition to walking boot
- Progressive weight bearing
Weeks 6-12:
- Full weight bearing
- Progressive activity
- Return to sport (3-4 months)
Outcomes and Prognosis
Overall Outcomes (what the evidence actually shows)
Conservative / functional treatment (the default for most fractures):
- Massen et al. (Injury 2019): immediate full weight-bearing gave good-to-excellent results — median VAS-FA 95, Karlsson 90 — with return to work at ~2 weeks and return to sport at ~3 months.
- Xiao et al. (OTSR 2023): of 84 conservatively treated patients, 31% had an unfavourable result (Karlsson ≤80) at 2 years, so outcome is not uniformly perfect.
Surgery (reserved for displaced intra-articular fragments or symptomatic nonunion):
- Cibura et al. (BMC 2022): of 13 surgically treated displaced intra-articular (type IIIB) fractures, only one nonunion occurred.
- Degan (JBJS Am 1982): excision relieved symptoms in most, but failed in patients with established missed nonunions — arguing for correct early diagnosis rather than primary excision.
Predictors of Poorer Outcome
- Concomitant talonavicular joint fracture (OR 3.6) and age ≥47.5 years (OR 5.0) independently predicted an unfavourable functional result (Xiao, OTSR 2023).
- Missed / delayed diagnosis is associated with higher complication rates and more frequent need for surgery (Cibura, BMC 2022).
Note: Stratified single-figure "success rates" by treatment type are not supported by high-quality data; the numbers above are quoted directly from the published series.
Guidelines, Registries & Global Practice
Global Epidemiology
- Frequency: Classically described as rare; quoted figures range from under 1% of calcaneal fractures to as high as ~15% of calcaneal injuries in radiology series, the variation driven mainly by under-recognition (Hodge, J Emerg Med 1999).
- Demographics: Adults across a wide age range; one of the larger functional-treatment cohorts was 74% female with a median age of 38 years (Massen, Injury 2019). Mechanism is forced inversion and plantarflexion — the same as a lateral ankle sprain.
- Associated injuries: Concomitant Chopart-line / talonavicular injuries are common and predict slower recovery (Xiao, OTSR 2023).
Guidelines & Society Positions (side by side)
There is no dedicated AAOS / BOA-BOAST / NICE / AO / EFORT clinical practice guideline specifically for the anterior process calcaneal fracture — a point worth stating directly in a viva. Practice is therefore extrapolated from foot-and-ankle trauma principles and the small published series.
- Relevant contribution
- Anatomic restoration of articular surfaces; protect the lateral column
- Practical message
- Reduce and fix displaced intra-articular (type IIIB) fragments
- Relevant contribution
- Soft-tissue assessment, timely senior review, CT for intra-articular injury
- Practical message
- Low threshold for CT when an inversion injury stays focally tender
- Relevant contribution
- Classification literacy (Degan / modified Degan) and outcome data
- Practical message
- Match treatment to fragment size and displacement, not type alone
- Relevant contribution
- Best available Level IV evidence
- Practical message
- Conservative first; surgery for displaced intra-articular or symptomatic nonunion
Registry Evidence
National joint/trauma registries (NJR, AJRR, AOANJRR, SHAR/Swedish, Norwegian, NZJR) do not capture this non-arthroplasty fracture, so there is no registry-level survival or revision data. Evidence remains confined to single-centre retrospective series — a genuine limitation of the field.
High- vs Limited-Resource Practice
- High-resource settings: CT is readily available and is used liberally to confirm the diagnosis, size the fragment, and assess calcaneocuboid involvement (Cibura, BMC 2022). Displaced intra-articular fragments may be offered ORIF.
- Limited-resource settings: Diagnosis relies on lateral and oblique foot radiographs (Trnka, 1998); where CT is unavailable, clinical suspicion plus oblique films guides a default of functional/conservative care, which gives good outcomes in the majority. The main avoidable harm worldwide is the missed diagnosis mislabelled as an ankle sprain.
A common foot-and-ankle viva trap. Know the bifurcate-ligament avulsion mechanism, the modified Degan classification, and that most fractures do well with conservative/functional treatment. State clearly that the evidence is Level IV with no dedicated society guideline, reserve surgery for displaced intra-articular fragments or symptomatic established nonunion, and remember the calcaneus secundarius differential and the talonavicular-injury / older-age predictors of poorer outcome.
Controversies & Areas of Uncertainty
The evidence base is entirely Level IV-V (small retrospective series and case reports). There is no randomised trial and no validated, universally adopted classification, so the following questions remain genuinely open.
Reported incidence ranges from "rare / under 1% of calcaneal fractures" to claims of up to 15% of calcaneal injuries (Hodge). The discrepancy reflects how often the fracture is missed and whether Chopart-line avulsions are counted, so any quoted figure should be hedged.
Traditional teaching is non-weight-bearing cast for 4-6 weeks, but Massen et al. reported good-to-excellent results with immediate full weight-bearing for non-displaced fractures. The optimal duration and need for any immobilisation are unsettled.
Degan (and the modified Cibura version) is the most used scheme, yet Massen found fracture type did NOT predict outcome. Whether classification should drive treatment, or only the size/displacement of an intra-articular fragment, is debated.
For displaced intra-articular (type IIIB) fragments threatening the calcaneocuboid joint, some favour ORIF to preserve the joint while others excise. Numbers are too small for a definitive answer; surgeon experience and fragment quality drive the choice.
State explicitly that the evidence is low-level (no RCTs). Anchor your answer on principles: most fractures do well conservatively; image with CT when suspected; reserve surgery for displaced intra-articular fragments or symptomatic established nonunion; and counsel older patients and those with concomitant Chopart/talonavicular injury that recovery may be incomplete.
MCQ Practice Points
Q: What is the bifurcate ligament and how does it relate to anterior process calcaneus fractures? A: Bifurcate ligament consists of calcaneonavicular and calcaneocuboid ligaments - Attaches to anterior process of calcaneus. Forced inversion and plantarflexion causes avulsion, resulting in anterior process fracture. Usually treated conservatively.
Q: What is the treatment approach for anterior process calcaneus fractures? A: Usually conservative or functional treatment - Cast/boot with protected weight-bearing, or immediate full weight-bearing for non-displaced fractures, giving good-to-excellent results in the majority. Surgery is reserved for displaced intra-articular (type IIIB) fragments (ORIF) or persistent symptomatic nonunion (excision).
Q: Why are anterior process calcaneus fractures often missed initially? A: Similar mechanism and symptoms to ankle sprain - about 30% are missed at presentation (Cibura, BMC 2022). High index of suspicion needed, especially with lateral foot pain after inversion injury. CT recommended if suspected clinically but X-ray negative.
Q: When is surgery indicated for anterior process calcaneus fractures? A: Rarely needed - Only for displaced intra-articular fragments (modified Degan IIIB, ORIF) or persistent symptomatic nonunion (excision). Most fractures do well with conservative/functional treatment.
Q: When is excision appropriate for anterior process calcaneus fractures? A: Small symptomatic fragments with persistent pain or established nonunion - Excision relieves symptoms and is preferable to unreliable fixation of a tiny fragment (Degan, JBJS Am 1982). It is a salvage step, not a primary strategy.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old athlete presents with lateral foot pain after forced inversion and plantarflexion injury. Initial diagnosis was ankle sprain, but pain persists 3 weeks later. Clinical examination shows tenderness over anterior process of calcaneus (anterior to lateral malleolus). Lateral X-ray shows small fracture of anterior process. CT shows non-displaced fracture.”
“A 30-year-old patient presents with persistent lateral foot pain 3 months after anterior process calcaneus fracture treated conservatively. X-rays show nonunion of small fragment (under 25% of process). The fragment is causing persistent pain and calcaneocuboid joint irritation.”
“A 45-year-old recreational hiker presents with mild dorsolateral midfoot ache after twisting the foot a week ago. A lateral foot X-ray shows a small bony density anterior to the calcaneus, overlying the talar head. The emergency team has labelled this an anterior process fracture and applied a cast. The patient asks whether this is really a fracture.”
Key Concepts
- Bifurcate ligament avulsion = calcaneonavicular + calcaneocuboid ligaments
- Anterior process is attachment site for bifurcate ligament
- Forced inversion and plantarflexion mechanism
- Usually conservative/functional treatment with good-to-excellent results
Classification (modified Degan)
- Type I / II: Extra-articular (small / larger) - conservative or functional
- Type IIIA: Intra-articular, non-displaced - conservative; confirm with CT
- Type IIIB: Intra-articular, displaced (CC step-off) - ORIF or excision
- Type drives the SURGICAL decision more than prognosis (Massen 2019)
Treatment
- Most fractures: Conservative (cast or boot, NWB 4-6 weeks)
- Large displaced fragment: ORIF (preserves joint)
- Small symptomatic fragment: Excision (relieves pain)
- Surgery rarely needed - only for specific indications
Surgical Technique
- ORIF: Lateral approach, anatomic reduction, lag screws (2.0-2.7mm)
- Excision: Same approach, remove fragment, smooth edges
- Preserve calcaneocuboid joint stability
- Verify reduction fluoroscopically
Complications
- Nonunion: 5-10% (prevent with adequate immobilization)
- Persistent pain: 10-15% (excision if symptomatic)
- Missed diagnosis: ~30% missed at presentation (Cibura 2022)
- Calcaneocuboid arthritis: 5-10% (prevent with anatomic reduction)
Evidence Base
Degan: Surgical excision — classic series
- 18 of 25 healed with cast immobilisation
- Excision failures were both missed/untreated nonunions
- Early excision usually NOT necessary
- Correct initial diagnosis is the key determinant of outcome
Cibura: Modified Degan classification & treatment algorithm
- Modified Degan: type IIIA (undisplaced) vs IIIB (displaced) intra-articular
- 29.3% missed at presentation
- Missed fractures: higher complication rate, more surgery
- Low-threshold CT for any clinical suspicion
Massen: Functional (full weight-bearing) treatment outcomes
- Full weight-bearing gave good-to-excellent outcomes
- Fast return to work (~2 weeks), slower return to sport (~3 months)
- Fracture type did NOT predict outcome in this cohort
- Most fractures are comminuted and have Chopart-line associations
Xiao: Predictors of poor functional outcome
- 31% unfavourable outcome at 2 years despite conservative care
- Concomitant talonavicular fracture predicts poor outcome (OR 3.6)
- Age ≥47.5 years predicts poor outcome (OR 5.0)
- Outcome is not uniformly benign
Trnka: Often-misdiagnosed fracture, oblique views
- Oblique foot X-rays are the key plain-film view
- Diagnosis is commonly missed
- Large intra-articular fragments risk calcaneocuboid arthrosis
- Do not delay surgery for significant displaced fragments
Hodge: Fracture vs calcaneus secundarius
- Calcaneus secundarius is an accessory ossicle (up to 5% prevalence)
- Smooth corticated margins favour ossicle; irregular margins favour fracture
- Clinical tenderness and mechanism distinguish the two
- Bilateral symmetric ossicles support a normal variant
Sarrafian: Bifurcate ligament & calcaneocuboid anatomy
- Bifurcate ligament = calcaneonavicular + calcaneocuboid limbs
- Origin is the dorsal anterior process of the calcaneus
- Stabiliser of the Chopart (midtarsal) joint
- Anterior process contributes to the calcaneocuboid joint surface