Hydroxyapatite Crystal Deposition Disease
- Hydroxyapatite crystal deposition disease (HADD) is the deposition of BASIC CALCIUM PHOSPHATE - HYDROXYAPATITE - crystals in PERIARTICULAR soft tissues (tendons, tendon sheaths, joint capsules, ligaments, bursae and occasionally within joints); the more familiar subtypes are CALCIFIC TENDINOPATHY and CALCIFIC PERIARTHRITIS.
- The crystals are very small and are NOT seen on routine polarised light microscopy (unlike the needle-shaped negatively birefringent urate of gout and the rhomboid positively birefringent CPPD), so the diagnosis rests on the IMAGING appearance of AMORPHOUS, cloud-like periarticular CALCIFICATION rather than on crystal identification.
- CALCIFIC TENDINOPATHY is the commonest manifestation - classically of the SUPRASPINATUS/ROTATOR CUFF (also the gluteal tendons at the hip, the wrist and elsewhere) - and passes through a FORMATIVE phase (often asymptomatic) and a RESORPTIVE phase, during which an acute, intensely painful inflammatory attack (acute calcific PERIARTHRITIS) can occur as the deposit is resorbed.
- The ACUTE attack mimics SEPTIC arthritis/infection and crystal arthritis (gout/CPPD) - it is red, hot, swollen and very painful - but is SELF-LIMITING over days to weeks, and the radiograph (amorphous periarticular calcification, which may fade as the deposit resorbs) and the absence of other features distinguish it; the key DIFFERENTIAL therefore includes gout (urate, first MTP, tophi) and CPPD (chondrocalcinosis of fibro/hyaline cartilage).
- A destructive variant is the MILWAUKEE SHOULDER - a rapidly destructive, often haemorrhagic, rotator-cuff-deficient glenohumeral arthropathy in elderly women associated with basic calcium phosphate crystals - and, rarely, hydroxyapatite deposits in confined spaces can cause compressive syndromes (calcific deposits within the carpal tunnel from HADD-related calcific periarthritis are a rare cause of CARPAL TUNNEL SYNDROME).
- MANAGEMENT is largely CONSERVATIVE: the acute attack is treated with NSAIDs/analgesia and rest (it is self-limiting), and chronic calcific tendinopathy with physiotherapy and NSAIDs; for refractory deposits, ULTRASOUND-GUIDED BARBOTAGE (needle aspiration/lavage of the calcium, sometimes called needling) is the usual minimally invasive option, though the comparative evidence is limited and it was still being tested against SHAM in a 210-patient randomised trial; most deposits resorb within a year anyway (74-83% by 12 months after lavage). Surgical excision/removal is reserved for the few that fail, and any compressive syndrome (e.g. carpal tunnel from a deposit) is treated by decompression/removal.
- “HADD = basic calcium phosphate (HYDROXYAPATITE) crystals in PERIARTICULAR soft tissue. NOT seen on standard polarised microscopy (unlike urate/CPPD) - diagnosed by AMORPHOUS, cloud-like periarticular calcification on imaging.
- “Calcific tendinopathy (classically supraspinatus/rotator cuff) -> acute calcific PERIARTHRITIS in the RESORPTIVE phase (red/hot/swollen, mimics sepsis/gout, self-limiting). Milwaukee shoulder = destructive BCP arthropathy.
- “Differential: gout (urate, negatively birefringent) vs CPPD (chondrocalcinosis, positively birefringent) vs HADD (amorphous calcification). Treat conservatively; ultrasound-guided BARBOTAGE for refractory deposits.
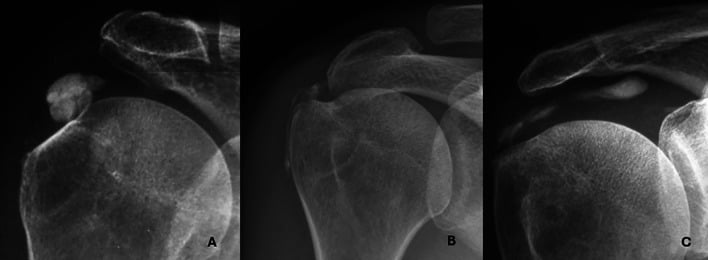
Amorphous, cloud-like periarticular calcification (often supraspinatus/rotator cuff). Crystals are invisible on standard polarised microscopy - it's an imaging diagnosis. Acute attack = the resorptive phase.
Gout = urate (needle, negatively birefringent, first MTP). CPPD = chondrocalcinosis (rhomboid, positively birefringent). HADD = amorphous calcification (hydroxyapatite).
The Spectrum: Tendinopathy, Acute Attack, Destruction
HADD is deposition of basic calcium phosphate (hydroxyapatite) crystals in periarticular soft tissues. The commonest form is calcific tendinopathy - classically of the supraspinatus/rotator cuff (also gluteal, hip, wrist) - which has a formative phase (often asymptomatic) and a resorptive phase, during which an acute, intensely painful calcific periarthritis attack can occur as the deposit is resorbed. This acute attack is red, hot and swollen and mimics infection and gout/CPPD, but is self-limiting. The crystals are not seen on routine polarised microscopy, so diagnosis rests on the amorphous, cloud-like periarticular calcification on imaging. A destructive variant is the Milwaukee shoulder (BCP-associated, cuff-deficient, elderly women).
- HADD (hydroxyapatite)
- Basic calcium phosphate (too small to see on light microscopy)
- Gout (urate)
- Monosodium urate - needle, negatively birefringent
- CPPD (pyrophosphate)
- Calcium pyrophosphate - rhomboid, positively birefringent
- HADD (hydroxyapatite)
- Amorphous periarticular/tendon calcification
- Gout (urate)
- Erosions w/ overhanging edges; tophi
- CPPD (pyrophosphate)
- Chondrocalcinosis (cartilage calcification)
- HADD (hydroxyapatite)
- Supraspinatus/rotator cuff (periarticular)
- Gout (urate)
- First MTP joint
- CPPD (pyrophosphate)
- Knee, wrist (triangular fibrocartilage)
- HADD (hydroxyapatite)
- Resorptive-phase calcific periarthritis
- Gout (urate)
- Acute gouty arthritis
- CPPD (pyrophosphate)
- Pseudogout
Pathogenesis and How the Crystals Inflame
- A cell-mediated pathogenesis (Uhthoff). Calcific tendinopathy is an actively regulated, cell-mediated process, not simple degeneration: pre-calcific (fibrocartilaginous metaplasia of tenocytes into chondrocyte-like cells in a hypoxic zone) → calcific (a formative phase laying down chalk-like calcium, then a resting phase, then a resorptive phase in which vascular invasion and macrophages/giant cells phagocytose the softened toothpaste-like deposit - the acutely painful phase) → post-calcific remodelling of the tendon back to normal collagen.
- How the crystals cause inflammation. Phagocytosed BCP crystals activate the NLRP3 inflammasome → caspase-1 → IL-1β release (the same final common pathway as urate and CPPD), and directly trigger cytokine/protease release - driving the acute, self-limiting resorptive-phase attack.
Q: What is the pathogenesis of calcific tendinopathy, and how do the crystals cause inflammation?
A: A cell-mediated process (Uhthoff), not simple degeneration: pre-calcific (fibrocartilaginous metaplasia of tenocytes) → calcific (formative - chalk deposit laid down; resting; resorptive - vascular invasion + macrophage/giant-cell phagocytosis of the softened deposit = the painful phase) → post-calcific remodelling. The crystals inflame by activating the NLRP3 inflammasome → caspase-1 → IL-1β (the same pathway as urate/CPPD), driving the acute self-limiting resorptive attack.
Management
- Acute attack (calcific periarthritis): NSAIDs/analgesia and rest - it is self-limiting over days to weeks (a subacromial corticosteroid injection may help the cuff).
- Chronic calcific tendinopathy: physiotherapy and NSAIDs.
- Refractory deposits: ultrasound-guided barbotage (needle aspiration/lavage of the calcium) is the usual minimally invasive option, with extracorporeal shockwave therapy an alternative - but the comparative evidence is limited, barbotage was still being tested against sham in a 210-patient trial, and most deposits resorb within a year regardless, so offer it for refractory symptoms rather than as established superiority. Surgical excision/removal for the few that fail.
- Compressive syndromes: a deposit causing, e.g., carpal tunnel syndrome is treated by decompression/removal of the calcific mass.
The main clinical trap in calcific periarthritis is the acute resorptive-phase attack: a red, hot, swollen, very painful joint/periarticular region that closely mimics septic arthritis and crystal arthritis. The discriminating features are the imaging - amorphous, cloud-like periarticular calcification (which may even fade as the deposit resorbs) rather than the erosions/tophi of gout or the chondrocalcinosis of CPPD - and the self-limiting course over days to weeks. Because the crystals are too small to see on standard polarised microscopy, the diagnosis is made on imaging rather than crystal identification, and where sepsis is a genuine possibility it must be excluded (aspiration/cultures) before attributing the picture to HADD. Treatment is largely conservative - NSAIDs and rest for the self-limiting attack, physiotherapy for chronic tendinopathy - with ultrasound-guided barbotage for refractory deposits and surgery reserved for the few that fail or for a deposit causing a compressive syndrome.
The Crystal: Chemistry and How It Is Detected
- What the crystal is. The deposit is basic calcium phosphate (BCP) - principally calcium hydroxyapatite (Ca10(PO4)6(OH)2), with carbonate-substituted apatite and octacalcium phosphate - chemically distinct from CPPD (calcium pyrophosphate dihydrate). The individual crystals are only about 75-250 nm and aggregate into clumps/"microspheroids", which is why they are sub-microscopic and non-birefringent (invisible on the ordinary polarised microscopy used for urate and CPPD).
- How they are detected. Alizarin red S stain colours calcium deposits red-orange - a sensitive screening test on synovial fluid or tissue, but non-specific (it cannot separate BCP from other calcium crystals). Definitive identification needs electron microscopy, X-ray diffraction, Fourier-transform infrared spectroscopy (FTIR) or atomic-force microscopy.
Q: What is the crystal in HADD chemically, and how is it detected?
A: Basic calcium phosphate (BCP) - principally calcium hydroxyapatite (Ca10(PO4)6(OH)2), ± carbonate-apatite/octacalcium phosphate - chemically distinct from CPPD's calcium pyrophosphate. The crystals are ~75-250 nm and aggregate into microspheroids, so they are sub-microscopic and non-birefringent (invisible on ordinary polarised microscopy). Detection: alizarin red S stains calcium (sensitive screen, non-specific); definitive ID needs electron microscopy, X-ray diffraction or FTIR.
Mnemonics & Memory Aids
APATITE
Hook:APATITE: Amorphous calcification, Periarticular, Acute resorptive attack, Tendinopathy (cuff), Invisible crystals, Treat/barbotage, Extreme = Milwaukee shoulder.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has a sudden, very painful, hot, swollen shoulder; the radiograph shows a cloud-like calcific deposit in the supraspinatus. What is the diagnosis and how do you manage it?”
What it is
- Basic calcium phosphate (hydroxyapatite) crystals in periarticular soft tissue
- Calcific tendinopathy (classically supraspinatus/rotator cuff) + calcific periarthritis
- Crystals invisible on standard polarised microscopy - imaging diagnosis
Phases & attack
- Formative (often asymptomatic) -> resorptive (acute attack)
- Acute calcific periarthritis: red/hot/swollen, mimics sepsis/gout, self-limiting
- Amorphous, cloud-like periarticular calcification (may fade as it resorbs)
Differential
- Gout: urate (needle, negatively birefringent, first MTP, tophi)
- CPPD: pyrophosphate (rhomboid, positively birefringent, chondrocalcinosis)
- HADD: amorphous calcification; Milwaukee shoulder = destructive variant
Management
- Acute: NSAIDs/rest (self-limiting); subacromial steroid injection (cuff)
- Chronic tendinopathy: physiotherapy/NSAIDs
- Refractory: ultrasound-guided barbotage (or shockwave); surgery rarely; decompress compressive deposits
What the Randomised Evidence Actually Supports
Calling barbotage "an effective first-line procedure" is the standard line, and it is worth knowing how thin the comparative evidence beneath it is - and what the trials that do exist actually measured.
In a randomised, double-blinded trial of 132 patients with a symptomatic deposit larger than 5 mm, all of whom had ultrasound-guided puncture and lavage, the calcification had resorbed in 83 percent of the saline arm and 74 percent of the steroid arm at 12 months. That is the number missing from the usual claim that deposits "resorb": most do, within a year, in treated shoulders - and the steroid did not change the resorption rate, answering the common worry that it might suppress it.
In the same trial, saline could not be shown non-inferior to methylprednisolone 40 mg for the week's maximal pain (mean difference 11.76, 95 percent CI 3.78 to 19.75, against a prespecified 10 mm margin), and the steroid significantly improved pain at rest and on activity and function at 7 days and 6 weeks, with benefit on function persisting to about 3 months. So the subacromial steroid given at the end of the procedure is not decoration - it buys early comfort - but it does not accelerate clearance of the calcium.
The recommendation rests on cohort data rather than on placebo-controlled proof. A multicentre randomised, double-blinded, sham-controlled trial of 210 patients in Norway and Sweden was designed precisely because, in its authors' words, there are few randomised studies and conflicting evidence about the effectiveness of the available treatments - randomising barbotage plus subacromial steroid against sham barbotage plus steroid, and against sham barbotage plus local anaesthetic. The existence of that trial is the point to carry: much of the apparent benefit attributed to needling has never been separated from the steroid given with it, or from the natural history of a deposit that resorbs in most patients within a year anyway. Offer barbotage for a refractory deposit, but do not present it as established superiority over the alternatives.
Three numbers worth having: the deposit had resorbed in 74 to 83 percent by 12 months after lavage regardless of whether steroid was given; the steroid improves pain and function at 7 days to 6 weeks but not resorption; and the trials use a deposit larger than 5 mm as the entry criterion for intervention. The comparative evidence between barbotage, shockwave and conservative care remains limited.
Evidence & Key Studies
Calcific periarthritis (HADD) causing carpal tunnel syndrome - management with ultrasound-guided barbotage
- Hydroxyapatite crystal deposition disease (HADD) results from deposition of calcium hydroxyapatite crystals in periarticular soft tissues - tendons, tendon sheaths, joint capsules, ligaments, bursae and occasionally within joints; the better-known subtypes are calcific tendinopathy and calcific periarthritis.
- Carpal tunnel syndrome can rarely be caused by calcific deposits within the carpal tunnel in HADD-related calcific periarthritis, with imaging (ultrasound and radiographs) crucial in distinguishing it from idiopathic carpal tunnel syndrome.
- Ultrasound-guided barbotage, a minimally invasive procedure, gave significant clinical improvement and is a viable first-line management option as an alternative to surgery.
Are corticosteroids needed after needling and lavage? Randomised, double-blind, non-inferiority trial
- Multicentre randomised, double-blinded non-inferiority trial in France: 132 patients (66 per arm) with a symptomatic rotator-cuff calcification larger than 5 mm, all undergoing ultrasound-guided puncture and lavage, then 1 mL of saline or methylprednisolone 40 mg into the subacromial bursa; 12-month follow-up.
- Non-inferiority of saline could NOT be established for the first week's maximal pain (mean difference 11.76, 95 percent CI 3.78 to 19.75; prespecified margin 10 mm on a 0 to 100 scale).
- Steroid significantly improved pain at rest and on activity and function at 7 days and 6 weeks, with functional benefit over the following 3 months.
- Steroid did NOT change the rate of calcification resorption, which occurred in 83 percent of the saline group and 74 percent of the steroid group by 12 months.
- The trial compares two adjuncts to lavage; it does not test lavage itself against no procedure, so it cannot show how much of the resorption reflects natural history.
Sham-controlled trial of barbotage: designed because the evidence was conflicting
- Protocol for a pragmatic, randomised, three-arm, double-blinded, SHAM-controlled multicentre trial in six institutions in Norway and Sweden, with 2-year follow-up.
- 210 patients aged 30 or older with a painful arc, positive impingement sign and a calcium deposit larger than 5 mm, randomised to barbotage plus subacromial steroid, SHAM barbotage plus steroid, or sham barbotage plus short-acting local anaesthetic; all received 8 weeks of standardised home physiotherapy.
- The stated rationale is that few randomised studies exist and the evidence about the effectiveness of the various treatments is conflicting.
- Primary outcome the Oxford Shoulder Score at 4 months, with follow-up to 24 months.
- This is the protocol paper - it establishes that the question was genuinely open and defines the design, and reports no results.
The nature of HADD (calcium hydroxyapatite crystal deposition in periarticular soft tissues, with calcific tendinopathy and calcific periarthritis as the main subtypes), a rare presentation as carpal tunnel syndrome, and the use of ultrasound-guided barbotage as a minimally invasive alternative to surgery in that single case come from the cited Ariyaratne report. The formative/resorptive phases, the acute attack mimicking sepsis/gout, the distinction from gout (urate) and CPPD (chondrocalcinosis), and the Milwaukee shoulder are standard, well- established teaching. The resorption rates, the steroid's effect on pain and function, and its absence of effect on resorption come from the cited Darrieutort-Laffite trial, which randomised two adjuncts to lavage rather than lavage against nothing, so it cannot separate the procedure's effect from natural history. That the comparative evidence is limited and conflicting, and that barbotage was still being tested against sham, come from the cited Moosmayer protocol - a design paper reporting no results. No trial establishing the superiority of barbotage over extracorporeal shockwave therapy or over conservative care was retrieved, and no validated threshold of deposit size, symptom duration or failed conservative treatment defining when to intervene exists beyond the "larger than 5 mm" entry criterion those trials used - so the decision remains clinical. See also calcific tendinitis of the shoulder, Milwaukee shoulder, gout and crystal arthropathy, pseudogout and CPPD disease and crystalline arthropathy of the hand. For the compressive presentation see carpal tunnel.