Rotator Cuff | Calcium Hydroxyapatite | Phases | Self-Limiting
- Calcium hydroxyapatite deposition
- Supraspinatus most common (insertion zone)
- Resorptive phase is most painful
- Self-limiting condition in most cases
- Ultrasound-guided barbotage is effective
- “Resorptive X-ray: fluffy, ill-defined calcium
- “Formative X-ray: dense, well-defined
- “Needling/barbotage is effective treatment
- “Shock wave therapy has evidence
Pre-calcific, Calcific (formative/resting), Resorptive, Post-calcific. Resorptive phase is most painful due to vascular invasion and inflammation.
Formative: dense, well-defined. Resorptive: fluffy, ill-defined, may have bursitis. X-ray appearance helps predict phase and prognosis.
Self-limiting in most cases. Calcium resorbs spontaneously. Most resolve within 1-3 years. Conservative treatment usually sufficient.
Needling/barbotage most effective intervention. US-guided aspiration and lavage. Shock wave therapy also effective. Surgery rarely needed.
- X-ray Appearance
- Dense, well-defined, homogeneous
- Symptoms
- May be asymptomatic or mild
- Prognosis
- May persist, needs intervention if symptomatic
- X-ray Appearance
- Dense, well-defined
- Symptoms
- May have mild symptoms
- Prognosis
- Stable phase, monitor
- X-ray Appearance
- Fluffy, ill-defined, irregular
- Symptoms
- Most painful, acute severe
- Prognosis
- GOOD - indicates resolution
PCRPCalcific Tendinitis Phases
Hook:PCRP - Phases of Calcium Rotation Process!
TEDRisk Factors - TED
Hook:TED causes Calcific Tendinitis!
Overview and Epidemiology
Calcium hydroxyapatite deposits in avascular zone of supraspinatus tendon (critical zone near insertion). Reason for deposition unclear. Cell-mediated process, not degenerative.
Pathophysiology and Mechanisms
Rotator cuff anatomy relevant to calcific tendinitis:
The supraspinatus tendon is most commonly affected (70-80% of cases), followed by infraspinatus (20%), teres minor, and subscapularis (rare).
- Located 1-2cm from the greater tuberosity insertion
- Area of relative hypovascularity
- Watershed zone between osseous and tendinous blood supply
- Site where calcium deposits typically form
- Cell-mediated process (not degenerative)
- Chondrocyte metaplasia of tenocytes
- Calcium hydroxyapatite crystal deposition
- Unknown trigger but associated with hypoxia
- Tendon compression between acromion and humeral head
- Repetitive microtrauma
- Impingement may coexist
The critical zone of the supraspinatus tendon is the watershed area 1-2cm from insertion - this is where calcification typically occurs due to relative hypovascularity.
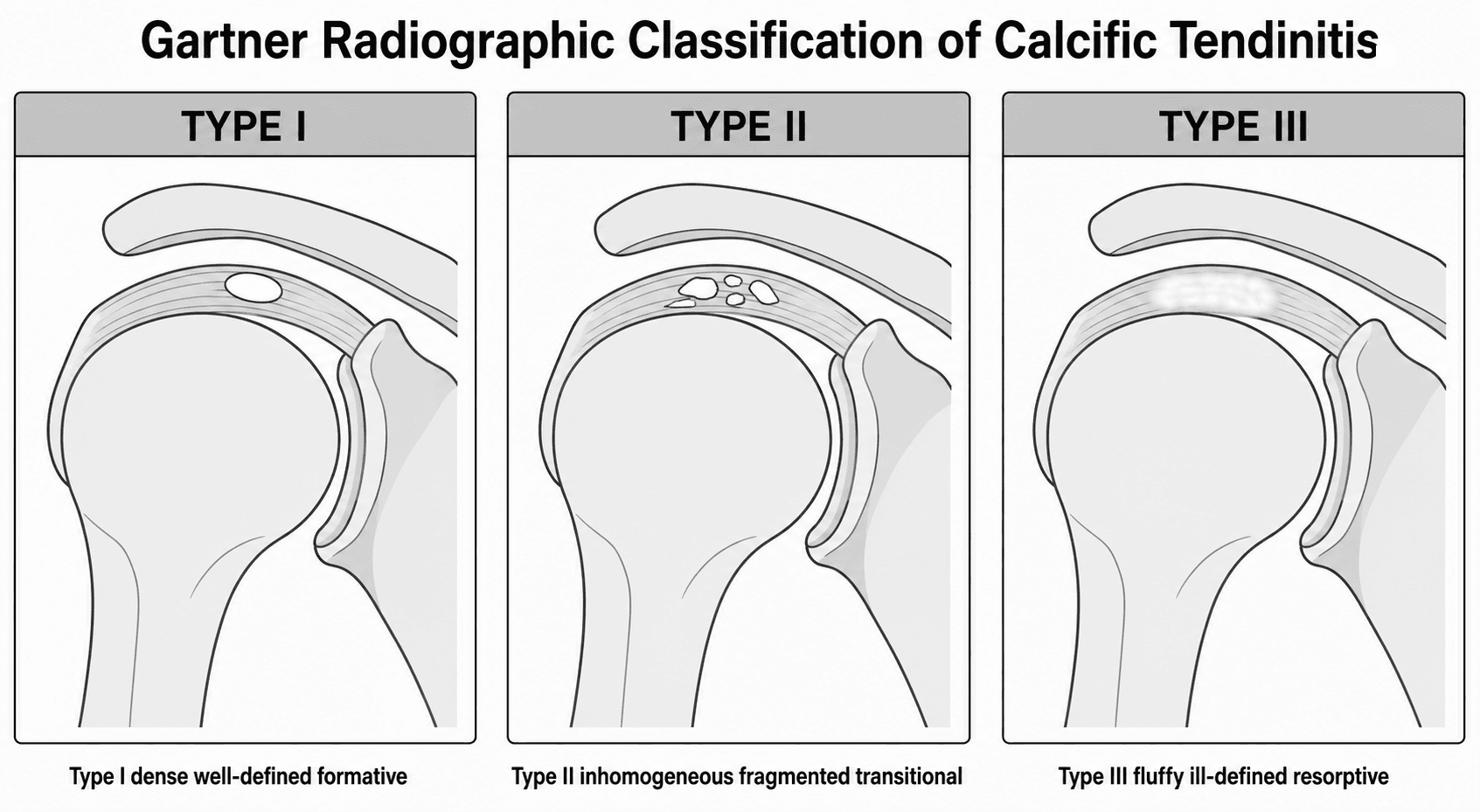
Classification Systems
Gartner Radiographic Classification
- Description
- Dense, well-defined, homogeneous
- Significance
- Formative phase, chronic
- Description
- Dense but inhomogeneous or fragmented
- Significance
- Transitional
- Description
- Fluffy, ill-defined
- Significance
- Resorptive phase, good prognosis
Gartner classification helps predict natural history and response to treatment.
Clinical Assessment
- Variable presentation
- May be asymptomatic (incidental)
- Chronic dull ache (formative)
- Severe acute pain (resorptive)
- Night pain common in acute phase
- May mimic frozen shoulder
Acute severe pain suggests resorptive phase.
- Painful arc
- Impingement signs may be positive
- ROM may be limited by pain
- Tenderness over greater tuberosity
- In acute phase, may be unable to move
Differentiate from rotator cuff tear.
When a calcific deposit ruptures into the subacromial bursa, it causes an intense inflammatory reaction (Acute Chemical Bursitis). The patient presents with a pseudoparalytic shoulder, severe pain, and warmth—mimicking septic arthritis. Always aspirate if in doubt.
NEVER inject corticosteroid directly into the tendon. Risk of tendon necrosis and rupture. Only inject into the subacromial bursa. Intratendinous injection also impairs the natural healing process.
Investigations
Plain Radiographs
AP, supraspinatus outlet, axillary
- Calcium deposit in supraspinatus insertion area
- Formative: dense, well-defined
- Resorptive: fluffy, ill-defined
X-ray appearance predicts phase and prognosis.

Calcium Migration: The Imaging Trap
A calcific deposit does not always stay within the tendon. Recognising where it migrates prevents serious misdiagnosis.
- Bursal migration: rupture into the subacromial-subdeltoid bursa produces the acute chemical bursitis described above - intensely painful pseudoparalysis that can mimic a septic joint.
- Osseous (intraosseous) migration: the deposit can erode through the cortex into the greater tuberosity, producing a lytic or erosive lesion with surrounding bone-marrow oedema. On radiographs, CT or MRI this can convincingly mimic osteomyelitis or a bone tumour and has led to unnecessary biopsy.
- The clue is the adjacent or residual tendinous calcium and the clinical context; intraosseous migration remains part of the benign, self-limiting calcific process and is managed conservatively, not as a neoplasm or infection.
Q: A patient with shoulder calcific tendinitis develops a lytic lesion in the greater tuberosity with marrow oedema on MRI. What is the likely diagnosis? A: Intraosseous (cortical) migration of the calcific deposit - a recognised mimic of osteomyelitis and bone tumour. Look for residual tendinous calcium and correlate with the clinical picture before considering biopsy; it is part of the benign, self-limiting process and is treated conservatively.
CALCIFCALCIF - Calcific Tendinitis Essentials
Hook:CALCIF - Remember the essentials of CALCIfic tendinitis!
TREATTREAT - Treatment Ladder
Hook:TREAT - the treatment ladder for calcific tendinitis!
Differential Diagnosis
- Key Distinguishing Features
- Acute severe pain, pseudoparalysis, afebrile, calcium on X-ray
- Investigation
- Plain X-ray, ultrasound
- Key Distinguishing Features
- Fever, raised CRP/ESR, systemically unwell, effusion
- Investigation
- Aspiration, blood cultures, inflammatory markers
- Key Distinguishing Features
- Weakness rather than pure pain, positive lag signs, no calcium
- Investigation
- Ultrasound or MRI
- Key Distinguishing Features
- Global loss of active AND passive external rotation, gradual onset
- Investigation
- Clinical; X-ray usually normal
- Key Distinguishing Features
- Localised ACJ tenderness, pain on cross-body adduction
- Investigation
- X-ray of ACJ
- Key Distinguishing Features
- Crystal arthropathy, may affect glenohumeral joint
- Investigation
- Joint aspiration and polarised microscopy
Calcific tendinitis is calcium hydroxyapatite deposition - NOT calcium pyrophosphate (CPPD/pseudogout). This distinction is frequently tested.
The Destructive End of the Spectrum: Milwaukee Shoulder
The same crystal family - basic calcium phosphate (BCP), principally hydroxyapatite - that deposits reversibly in calcific tendinitis can, at the other extreme, drive a destructive arthropathy.
- Milwaukee shoulder is a BCP-crystal (hydroxyapatite) associated arthropathy seen typically in elderly women, characterised by a large, often blood-stained but non-inflammatory joint effusion, a massive rotator cuff tear and rapidly progressive glenohumeral destruction (cuff-tear arthropathy).
- BCP crystals are not birefringent under polarised light (unlike the negatively-birefringent urate of gout or the weakly-positively-birefringent CPPD of pseudogout), so they are easily missed - alizarin red staining or electron microscopy is needed to identify them.
- Management is largely supportive (analgesia, aspiration, activity modification); a reverse total shoulder arthroplasty is the reconstructive option for end-stage cuff-tear arthropathy, because the deficient cuff makes an anatomic replacement fail.
Q: How is Milwaukee shoulder related to calcific tendinitis, and how do their crystals appear on microscopy? A: Both involve basic calcium phosphate / hydroxyapatite crystals, but calcific tendinitis is a localised, self-limiting reactive deposition whereas Milwaukee shoulder is a destructive cuff-tear arthropathy of the elderly. BCP crystals are non-birefringent (invisible on standard polarised microscopy, demonstrated with alizarin red), distinguishing them from the birefringent crystals of gout and pseudogout.
Management

First-Line Treatment
- NSAIDs
- Ice
- Subacromial injection (steroid)
- Activity modification
- Physical therapy
- Time (self-limiting)
- NSAIDs as needed
Most resolve within 1-3 years spontaneously.
Surgical Technique
Arthroscopic Calcific Deposit Excision
- Failed conservative management (6+ months)
- Failed ultrasound-guided barbotage
- Failed ESWT
- Large symptomatic deposit
- Beach chair or lateral position
- Standard posterior viewing portal
- Diagnostic arthroscopy - assess cuff, labrum, biceps
- Locate deposit using spinal needle under fluoroscopy
- Incise bursal surface over deposit
- Curette and evacuate calcium (paste-like material)
- Avoid excessive debridement of healthy tendon
- Subacromial decompression if impingement present
- Consider side-to-side repair if large defect
- Calcium may be deep within tendon
- Needle localization helpful
- Do not repair small defects (heal spontaneously)
- Repair defects greater than 1cm transverse dimension
Minimize debridement of healthy tendon tissue. The goal is to evacuate calcium, not remove tendon. Small defects heal without repair.
Complications
- Prolonged symptoms (rare, condition usually self-limiting)
- Frozen shoulder (may develop secondary stiffness)
- Chronic pain if resorption does not occur
- Post-procedure pain flare (common, 24-48 hours)
- Infection (rare, less than 0.1%)
- Neurovascular injury (rare with proper technique)
- Incomplete calcium removal
- Rotator cuff tear (iatrogenic during debridement)
- Incomplete excision (residual calcium)
- Infection (less than 1%)
- Stiffness/frozen shoulder (2-5%)
- Failure to improve symptoms
- Recurrence is rare (less than 10%) after complete resolution
- More common if calcium incompletely removed during surgery
Warn patients that pain may temporarily worsen after barbotage or surgery due to inflammatory response to calcium crystal release. This typically settles within 48-72 hours.
Postoperative Care
After barbotage:
- Sling for comfort only (24-48 hours)
- Ice, analgesia (NSAIDs)
- Resume normal activities as tolerated
- Physiotherapy for ROM and strengthening
- Review at 6-8 weeks with repeat imaging
After arthroscopic excision:
Rehabilitation Protocol
Protection phase: Sling for comfort, pendulum exercises, gentle passive ROM
Motion phase: Progressive active ROM, no resistance, avoid impingement positions
Strengthening phase: Rotator cuff strengthening, scapular stabilization, progressive resistance
Return to activity: Sport-specific training, full activities when strength recovered
If rotator cuff repair performed:
- Standard cuff repair rehabilitation protocol
- No active elevation for 6 weeks
- Sling for 4-6 weeks
Outcomes
Prognostic Factors
Resorptive phase (will resolve), soft deposits, smaller size.
Dense formative deposits, large deposits, associated cuff tears.
Guidelines, Registries & Global Practice
Global epidemiology
- Radiographic calcific deposits are found in roughly 3-8% of adults, the majority asymptomatic.
- Peak incidence is in the 30-60 year age group, with a female predominance in most cohorts (around 60-65%).
- The supraspinatus is involved in the large majority of cases; bilateral disease occurs in roughly 10-20% and is a negative prognostic marker (Ogon et al, Arthritis Rheum 2009, PMID 19790063).
- Associations reported across populations include diabetes mellitus, thyroid disorders and a possible genetic/metabolic predisposition, although causation is unproven.
- First-line
- Education, analgesia, physiotherapy, activity modification
- Refractory deposit
- US-guided barbotage and/or ESWT
- Surgery
- Arthroscopic removal after failed non-operative care
- First-line
- Reassurance about self-limiting course, analgesia, physiotherapy
- Refractory deposit
- Barbotage; high-energy ESWT where available
- Surgery
- Arthroscopic excision reserved for true failure
- First-line
- Conservative with staged escalation per Uhthoff phase
- Refractory deposit
- Barbotage plus subacromial steroid; ESWT
- Surgery
- Arthroscopic excision; avoid routine acromioplasty
- First-line
- Conservative first - most resolve
- Refractory deposit
- Barbotage + subacromial steroid favoured by pooled RCT data
- Surgery
- Last resort; do NOT routinely add decompression
Registry and evidence notes
- Calcific tendinitis is a soft-tissue disorder, so it is not tracked by arthroplasty/implant registries (NJR, AJRR, AOANJRR). The strongest evidence base is from RCTs and meta-analyses rather than registries.
- Pooled RCT evidence (network meta-analysis, PMID 27554465) ranks US-guided needling plus subacromial corticosteroid as the preferred non-surgical option, with high-energy ESWT (PMID 14625334) a reasonable alternative.
High- vs limited-resource practice variation
- In well-resourced settings, ultrasound-guided barbotage and high-energy ESWT are widely available and used early for refractory deposits.
- Where musculoskeletal ultrasound or ESWT machines are scarce, management leans on plain radiographs, analgesia, physiotherapy, and image-free subacromial injection, reserving referral for arthroscopy in persistent cases.
- Across all settings the message is the same: counsel patients on the strongly self-limiting natural history before escalating to any intervention.
Controversies & Areas of Uncertainty
High-energy ESWT outperforms low-energy and placebo (PMID 14625334), but the ideal energy flux density, number of sessions and use of imaging guidance remain debated.
Single- vs two-needle technique, optimal needle gauge, and whether to add a subacromial steroid are not standardised, though pooled data favour adding steroid.
After complete excision, evidence is split between leaving small defects to heal and routine repair (PMID 20151109). Most surgeons repair only structurally significant defects.
The trigger for fibrocartilaginous metaplasia and hydroxyapatite deposition is still unknown; hypoxia and a cell-mediated reactive process are favoured over simple degeneration.
MCQ Practice Points
Q: Which phase of calcific tendinitis is most painful? A: Resorptive phase. Vascular invasion and inflammation cause severe pain.
Q: What is the X-ray appearance of resorptive phase? A: Fluffy and ill-defined. Formative phase is dense and well-defined.
Q: What is the most effective non-surgical intervention? A: Ultrasound-guided barbotage (needling). 60-80% success rate.
Q: Which Gartner type has the best prognosis? A: Type III (fluffy, ill-defined) - indicates resorptive phase with active resolution.
Q: What is the most common location for calcific tendinitis? A: Supraspinatus tendon (70-80%), specifically in the critical zone 1-2cm from insertion.
Q: Why should you avoid intratendinous steroid injection? A: It increases the risk of tendon necrosis and rupture and impairs healing. Only inject into the subacromial bursa.
Q: How do you differentiate acute calcific tendinitis from septic arthritis? A: Both present with severe pain and pseudoparalysis, but calcific tendinitis patients are typically afebrile with normal inflammatory markers (CRP/ESR). Aspiration is definitive if in doubt.
Q: Does adding subacromial decompression improve outcomes in surgical excision of calcific tendinitis? A: No. Comparative evidence (Marder et al., JSES 2011) shows no benefit and actually slower recovery; the pathology is intrinsic tendon metaplasia, not extrinsic impingement.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old woman presents with sudden severe shoulder pain starting last night. She cannot move her shoulder. X-ray shows a fluffy, ill-defined calcific deposit at the supraspinatus insertion with surrounding soft tissue swelling. What is your diagnosis and management?”
“A 50-year-old male desk worker has chronic shoulder pain for 18 months. X-ray shows a dense, well-defined calcific deposit in the supraspinatus. He has had physiotherapy and two steroid injections without relief. What is your management?”
“A 42-year-old woman had a shoulder X-ray for trauma (normal result). Incidentally, a 1cm dense calcific deposit is seen in the supraspinatus. She has no shoulder pain. How do you manage this?”
Phases
- Pre-calcific: fibrocartilage metaplasia of tenocytes
- Calcific (formative): calcium deposition, may be asymptomatic
- Resorptive: MOST PAINFUL phase, vascular invasion
- Post-calcific: healing and tendon reconstitution
- Phase determines prognosis and treatment approach
X-ray Appearance
- Formative: dense, well-defined, homogeneous
- Resorptive: fluffy, ill-defined, irregular
- Gartner Type I = formative, Type III = resorptive
- X-ray appearance predicts phase and prognosis
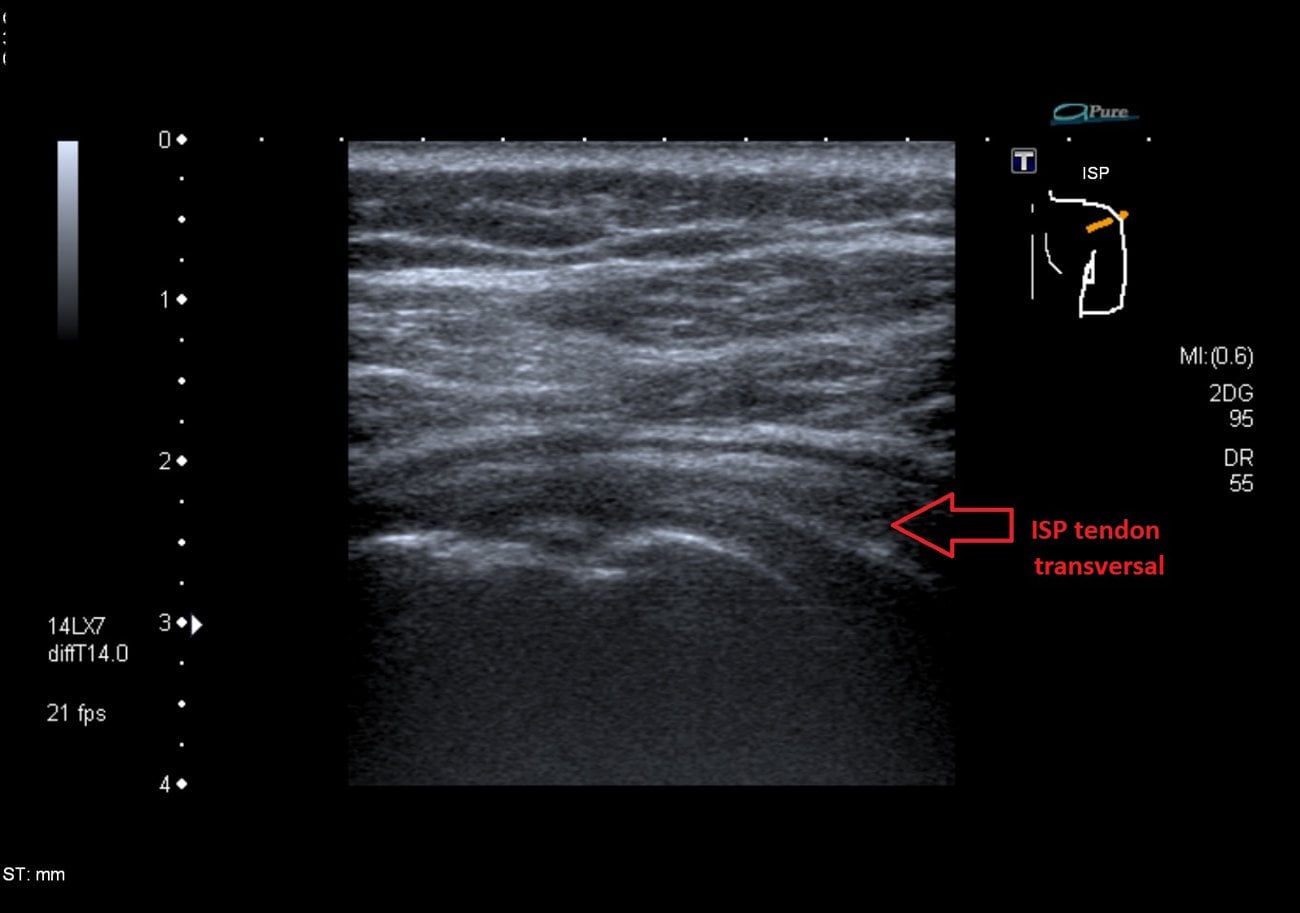
- Ultrasound shows soft vs hard calcium consistency
Natural History
- Self-limiting in 80-90% of cases
- Resolves spontaneously in 1-3 years
- Resorptive phase = resolution coming (good sign)
- Symptoms resolve before radiographic changes
- 3-7% adult prevalence, often asymptomatic
Treatment Ladder
- Conservative first: NSAIDs, ice, physio, injection
- Barbotage: 60-80% success (most effective)
- ESWT: 50-70% success, good before surgery
- Arthroscopic excision: 90%+ success, last resort
- Rarely need surgery if barbotage/ESWT offered
Key Exam Points
- Supraspinatus most common (70-80%), critical zone
- Acute severe pain = resorptive = GOOD prognosis
- Dense deposit = chronic, may need intervention
- Counsel about self-limiting nature of condition
- Calcium hydroxyapatite crystals (not CPPD)
Evidence Base
Prognostic Factors in Non-operative Therapy (Ogon)
- Prospective cohort of 420 patients (488 shoulders), mean age 51 years, 64% female
- Failure of non-operative therapy in 114 patients (27%)
- Negative prognostic factors: bilateral disease, anterior acromial localisation, medial (subacromial) extension, large deposit volume
- Positive prognostic factors: Gärtner type III deposit and lack of sonographic sound extinction
Barbotage + Subacromial Steroid vs Injection Alone (de Witte 1-year RCT)
- RCT of 48 patients: US-guided barbotage plus subacromial steroid (group 1) vs isolated subacromial steroid (group 2)
- 1-year Constant score 86.0 vs 73.9 in favour of barbotage (P = .005)
- Mean calcification size reduced 11.6 mm vs 5.1 mm (P = .001)
- More patients in the injection-only group needed additional procedures
Barbotage vs Injection at 5 Years (de Witte midterm RCT)
- 5-year follow-up of the same RCT (48 patients)
- Constant scores converged: 90 (barbotage) vs 87 (injection), no significant difference (P = .58)
- Total resorption 62% vs 73% (P = .45)
- Far fewer additional treatments after barbotage: 4 vs 16 patients (P less than .001)
ESWT for Chronic Calcifying Tendinitis (Gerdesmeyer RCT)
- Double-blind RCT of 144 patients: high-energy vs low-energy ESWT vs sham
- 6-month Constant-Murley improvement 31 (high-energy) vs 15 (low-energy) vs 6.6 (sham), P less than .001
- High-energy ESWT significantly superior to low-energy (P less than .001)
- Improved function, reduced pain and diminished deposit size; no serious adverse events
Arthroscopic Excision - Midterm Results (Balke)
- Case series of 70 shoulders (62 patients), mean 6-year follow-up
- ASES scores improved significantly after surgery but remained below the healthy contralateral shoulder
- Partial supraspinatus tears more frequent on the operated side (11 vs 3 contralateral on ultrasound)
- Additional subacromial decompression did not improve overall scores but reduced postoperative pain
Network Meta-analysis of Non-operative Treatments (Arirachakaran)
- Network meta-analysis of 7 RCTs comparing ESWT, US-guided lavage (barbotage), subacromial injection and combinations
- Combined US-guided needling plus subacromial corticosteroid most improved Constant score and pain VAS and most reduced deposit size
- ESWT significantly better than placebo for pain and function
- No clinically important difference in adverse events between treatments
Subacromial Decompression Adds No Benefit (Marder)
- Comparative study of 50 patients: debridement of the deposit alone (25) vs debridement plus subacromial decompression (25)
- Final QuickDASH and UCLA scores equal in both groups (both high function) at mean 5-year follow-up
- Time to pain-free unrestricted activity shorter WITHOUT decompression (11 vs 18 weeks, P less than .006)
- Adding decompression delayed recovery without improving outcome
Complete Removal + Cuff Repair After Excision (Yoo)
- 35 patients undergoing arthroscopic COMPLETE removal of the calcific deposit
- 18 had a resulting full-thickness defect repaired with suture anchors; 17 had side-to-side repair or debridement
- Pain relief within 6 months in 30 of 35; good clinical outcomes at median 31 months
- 10 of 35 developed secondary stiff shoulder