Immobilization | ATLS | Upper vs Subaxial
- ATLS immobilization until cleared clinically and radiologically
- Upper cervical (C1-C2) injuries have specific patterns
- Subaxial cervical (C3-C7): Use SLIC score to guide treatment
- MRI if neurological deficit or to assess ligaments
- NEXUS or Canadian C-spine rules for clearance
- “Jefferson fracture: Lateral mass spread greater than 7mm = TAL rupture
- “Odontoid Type II (base of dens) has high nonunion rate
- “Hangman's is usually stable (paradoxically) unless severe
- “SLIC greater than or equal to 5 = surgery, 3-4 = equivocal, less than 3 = conservative
Clinical Imaging
Imaging Atlas


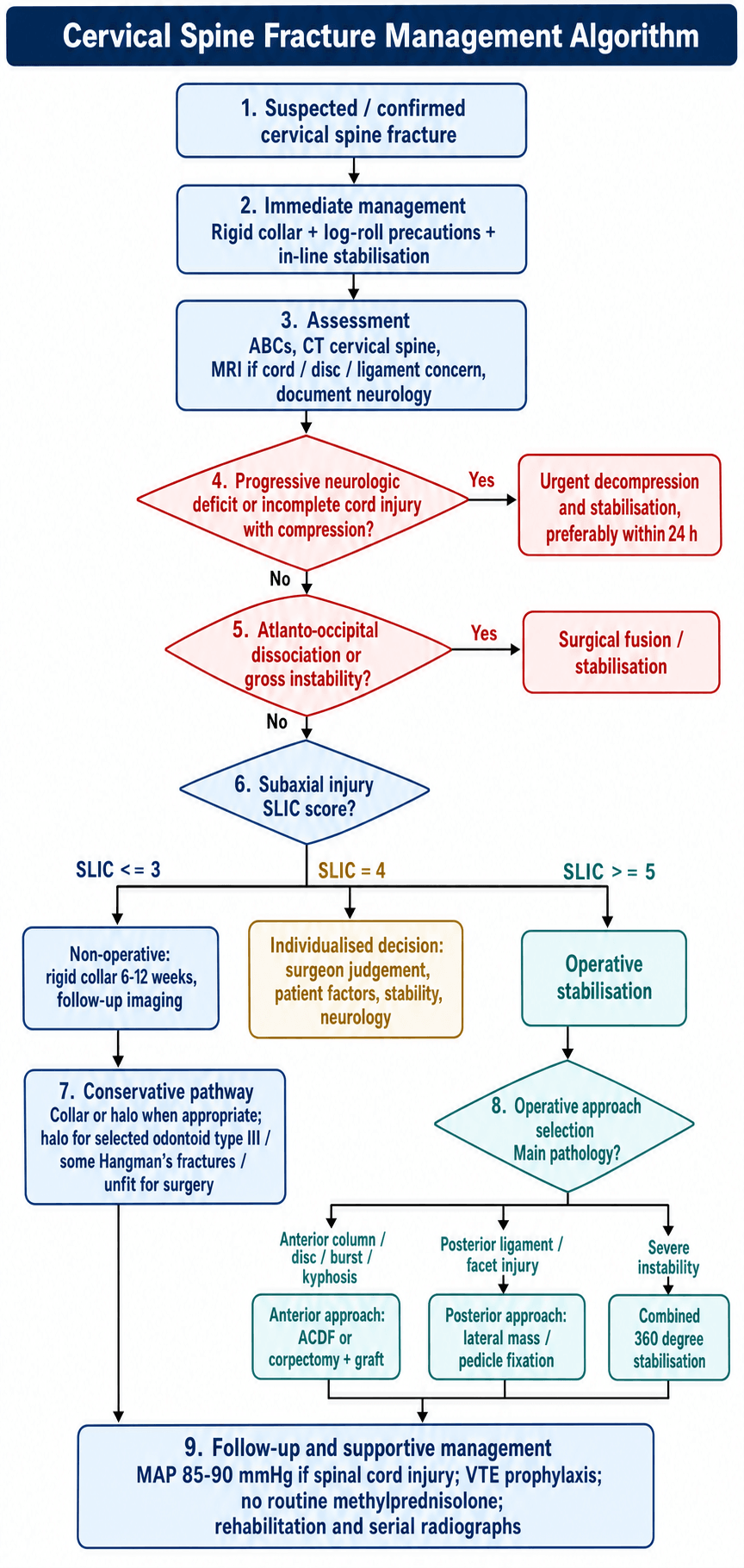
All trauma patients: Assume C-spine injury until cleared. Rigid collar, log-roll, in-line immobilization for intubation. NEXUS/Canadian C-spine rules guide clearance.
C1 (Atlas): Jefferson (burst) - TAL integrity key. C2 (Axis): Odontoid (Type I/II/III) and Hangman's (bilateral pars). Require specialized imaging and often halo or surgery.
Subaxial Injury Classification (C3-C7). Scores morphology, disco-ligamentous complex, neurology. Score greater than or equal to 5 = surgery. 3-4 = equivocal. Less than 3 = conservative.
Essential if: Neurological deficit, obtunded patient, suspected ligamentous injury. May show disc herniation, cord contusion, ligament disruption.
At a Glance
Cervical spine fractures require immediate immobilization until clinically and radiologically cleared using NEXUS or Canadian C-spine rules. Upper cervical injuries (C1-C2) include Jefferson fracture (C1 burst - lateral mass spread greater than 7mm indicates TAL rupture), odontoid fractures (Type II at dens base has highest nonunion rate requiring surgery), and Hangman's fracture (bilateral C2 pars - paradoxically stable unless severely displaced). Subaxial injuries (C3-C7) are classified using the SLIC score combining morphology, disco-ligamentous complex status, and neurological status; scores ≥5 indicate surgery, ≤2 conservative management, 3-4 equivocal. MRI is essential for neurological deficit or suspected ligamentous injury.
1-2-3Odontoid Fracture Types
Hook:Type II = Trouble (high nonunion)!
Overview
Cervical spine fractures are potentially devastating injuries. The priority is to protect the spinal cord while evaluating and treating the bony and ligamentous injury.
ATLS Approach
- Immobilize in rigid collar
- Log-roll for turns
- In-line immobilization for airway management
- Do NOT remove collar until cleared
Imaging
X-rays: Less commonly used now (CT is standard).
CT: Primary imaging for bony injury.
MRI: For neurological deficit, to assess ligaments, disc, and cord.
Upper Cervical (C1-C2)
Jefferson Fracture: Burst fracture of C1 (atlas) - typically 4-part fracture of both arches.
Mechanism: Axial load (e.g., diving).
Key: Assess transverse atlantal ligament (TAL) integrity.
Rule of Spence: Combined lateral mass overhang greater than 7mm on open-mouth X-ray suggests TAL rupture → unstable.
Treatment:
- TAL intact: Rigid collar or halo
- TAL ruptured: Surgical stabilization (C1-C2 fusion)


Subaxial Cervical (C3-C7)
Subaxial injuries (C3-C7) are graded with the SLIC score (morphology + disco-ligamentous complex + neurology) and described morphologically with the AOSpine system. The full SLIC and AOSpine tables are in the Classification section below; the summary threshold is: less than 4 conservative, 4 surgeon discretion, greater than 4 operative.
Common Patterns
Facet Dislocation: Unilateral or bilateral. Rotational/translational injury. Usually requires reduction and fusion.
Compression Fracture: Anterior wedging. May be stable if posterior elements intact.
Burst Fracture: Retropulsion into canal. May need surgery if cord compression.
MDNSLIC Score Components
Hook:Add Morphology + DLC + Neurology: less than 4 conservative, 4 discretion, greater than 4 operate
The primary goal in cervical spine trauma is to protect the spinal cord from further injury. Maintain immobilization until fully assessed. Any neurological deterioration requires urgent MRI and surgical consultation.
Anatomy
Upper Cervical Spine (C0-C2)
Atlantooccipital Joint (C0-C1)
- Allows 50% of cervical flexion-extension
- Stabilized by tectorial membrane, alar ligaments, cruciate ligament
Atlas (C1)
- Ring structure without vertebral body
- Anterior and posterior arches with lateral masses
- Articulates with occipital condyles superiorly, C2 inferiorly
Axis (C2)
- Contains odontoid process (dens) projecting superiorly
- Dens articulates with anterior arch of C1
- Transverse atlantal ligament (TAL) holds dens against C1 anterior arch
- Large spinous process and pars interarticularis
Key Ligaments
- Transverse Atlantal Ligament (TAL): Primary stabilizer of C1-C2; prevents anterior translation of C1
- Alar Ligaments: Limit rotation
- Tectorial Membrane: Continuation of PLL to occiput
- Cruciate Ligament: TAL + vertical bands
Subaxial Cervical Spine (C3-C7)
Vertebral Structure
- Anterior column: Vertebral body, intervertebral disc
- Posterior column: Pedicles, lateral masses, facet joints, laminae, spinous processes
- Uncovertebral joints (joints of Luschka): Unique to cervical spine
Disco-Ligamentous Complex (DLC)
- Anterior longitudinal ligament (ALL)
- Posterior longitudinal ligament (PLL)
- Intervertebral disc
- Facet joint capsules
- Ligamentum flavum
- Interspinous ligament
Neural Structures
- Spinal cord: Terminates as conus at L1-L2
- Cervical roots exit above same-numbered vertebra (C6 root exits at C5-C6)
- Vertebral arteries traverse foramen transversarium C6-C1
Pathophysiology
Cervical spine injury results from the interaction of applied force vector and host bone/ligament quality. Understanding the mechanism predicts the pattern and the risk to neural structures.
Mechanism to Pattern
- Axial load: Burst patterns - Jefferson (C1) and subaxial burst fractures with retropulsion into the canal
- Hyperextension: Hangman's fracture (C2 pars), anterior tension-band (Type B3) injuries, and central cord syndrome in the spondylotic spine
- Flexion / flexion-distraction: Wedge compression, facet subluxation/dislocation, posterior ligamentous (tension-band) failure
- Flexion-rotation: Unilateral facet dislocation
- Distraction: Atlanto-occipital dissociation and highly unstable distraction injuries
Primary vs Secondary Cord Injury
- Primary injury: immediate mechanical disruption (contusion, laceration, compression) at the moment of impact - irreversible
- Secondary injury: an evolving cascade of oedema, ischaemia, excitotoxicity, free-radical damage and inflammation over hours to days. This is the therapeutic target of immobilisation, MAP augmentation (~85-90 mmHg) and early decompression
Host Factors
- Ankylosing spondylitis / DISH: the rigid, brittle, osteoporotic spine fails like a long bone - low-energy, often transverse, three-column, highly unstable fractures that are easily missed
- Osteoporosis and pre-existing canal stenosis: lower the force threshold for both fracture and cord injury, explaining the elderly fall-related odontoid and central cord patterns
Classification
Occipital Condyle Fractures (Anderson & Montesano)
- Description
- Impaction from axial load
- Stability
- Stable
- Description
- Basilar skull fracture extension
- Stability
- Stable
- Description
- Avulsion by alar ligament
- Stability
- Potentially unstable
Atlantooccipital Dissociation (Traynelis)
- Direction
- Anterior
- Treatment
- Fusion
- Direction
- Longitudinal (distraction)
- Treatment
- Fusion
- Direction
- Posterior
- Treatment
- Fusion
C1 Ring Fractures (Jefferson)
- Burst fracture from axial load
- Typically 4-part (both arches)
- Rule of Spence: Lateral mass overhang greater than 7mm = TAL rupture = unstable
Odontoid Fractures (Anderson & D'Alonzo)
- Location
- Tip (avulsion)
- Nonunion Risk
- Low
- Treatment
- Collar
- Location
- Base (waist)
- Nonunion Risk
- High (40%)
- Treatment
- Surgery often
- Location
- Into C2 body
- Nonunion Risk
- Low
- Treatment
- Halo
Hangman's Fracture (Levine-Edwards)
- Displacement
- Less than 3mm
- Angulation
- Minimal
- Treatment
- Collar
- Displacement
- Greater than 3mm
- Angulation
- Present
- Treatment
- Halo or surgery
- Displacement
- Minimal
- Angulation
- Severe
- Treatment
- Surgery (traction contraindicated)
- Displacement
- Facet dislocation
- Angulation
- Severe
- Treatment
- Surgery
Clinical Assessment
Primary Survey (ATLS)
Airway with C-spine protection
- In-line stabilization for intubation
- Avoid neck extension
- Consider awake fiberoptic intubation if time permits
Breathing and Circulation
- Neurogenic shock: Hypotension + bradycardia (loss of sympathetic tone)
- Differentiate from hypovolemic shock
Disability
- GCS and pupillary response
- Spinal cord injury level
Neurological Examination
Motor Assessment (ASIA/ISNCSCI)
- Key Muscle
- Biceps
- Action
- Elbow flexion
- Key Muscle
- Wrist extensors
- Action
- Wrist extension
- Key Muscle
- Triceps
- Action
- Elbow extension
- Key Muscle
- FDP (middle finger)
- Action
- Finger flexion
- Key Muscle
- Interossei
- Action
- Finger abduction
Sensory Assessment
- Key Dermatome
- Top of shoulders
- Key Dermatome
- Lateral arm
- Key Dermatome
- Thumb
- Key Dermatome
- Middle finger
- Key Dermatome
- Little finger
- Key Dermatome
- Medial arm
ASIA Impairment Scale
- A: Complete - No motor/sensory function in S4-S5
- B: Sensory incomplete - Sensory but no motor below level, including S4-S5
- C: Motor incomplete - Motor function preserved, majority of key muscles less than 3/5
- D: Motor incomplete - Motor function preserved, majority ≥3/5
- E: Normal
Clearance Criteria
Canadian C-Spine Rules
- Any high-risk factor? → Imaging
- Age ≥65, dangerous mechanism, paresthesias
- Any low-risk factor allowing ROM? → Can assess ROM
- Simple rear-end MVC, ambulatory, delayed pain onset
- Can actively rotate 45° each direction? → No imaging needed
NEXUS Criteria (all must be present)
- No midline tenderness
- No focal neurological deficit
- Normal alertness
- No intoxication
- No distracting injury
NSAIDNEXUS - Who Can Be Cleared Clinically
Hook:All five NSAID criteria satisfied = no imaging needed
Investigations
Imaging Algorithm
CT Cervical Spine (First-line)
- Indicated for all significant trauma
- Skull base to T1 (include C7-T1 junction)
- 100% sensitivity for fractures
- Assess: Alignment, fracture pattern, canal compromise

MRI Cervical Spine
- Indications:
- Neurological deficit
- Obtunded patient (cannot clinically clear)
- Suspected ligamentous injury (DLC)
- Suspected disc herniation
- Findings: Cord edema/contusion, disc herniation, ligament rupture (bright T2 signal)
- Timing: Within 24-72 hours for acute injury
CT Angiography
- Indications:
- Fracture through foramen transversarium
- Facet subluxation/dislocation
- High-energy mechanism
- Screens for vertebral artery injury (dissection, occlusion)
Key Imaging Findings
Upper Cervical
- Jefferson: Open-mouth (odontoid) view - lateral mass overhang
- Odontoid: Sagittal CT - fracture line location
- Hangman: Bilateral C2 pars fractures
Subaxial
- Facet dislocation: Perched or locked facets on sagittal CT
- DLC disruption on MRI: Bright signal in ligaments/disc
- Canal compromise: Measure for surgical planning
Laboratory Studies
- FBC, coagulation profile (pre-operative)
- Group and screen
- Consider arterial blood gas if respiratory compromise
Management
Immediate Management
Immobilization
- Rigid cervical collar (properly sized)
- Log-roll precautions
- In-line stabilization for all procedures
Hemodynamic Support
- Target MAP 85-90 mmHg for spinal cord injury
- Differentiate neurogenic from hypovolemic shock
- Vasopressors if needed (norepinephrine)
Steroids
- Methylprednisolone NO LONGER recommended
- AANS/CNS guidelines: Risks outweigh benefits
- May increase infection, GI bleeding risk
Thromboprophylaxis
- High risk for VTE
- Mechanical prophylaxis immediately
- Chemical prophylaxis within 72 hours (if no active bleeding)
Surgical Technique
C1-C2 Fusion Techniques
Posterior C1-C2 Fusion (Harms Technique)
- C1 lateral mass screws + C2 pedicle screws
- Rod fixation
- Bone graft between C1-C2
- Advantages: Direct visualization, high fusion rate
- Risks: Vertebral artery injury (C2 pedicle)
Gallie Fusion
- Sublaminar wire around C1 and C2
- Structural bone graft
- Older technique, less rigid than screw fixation
Brooks Fusion
- Bilateral sublaminar wires around C1-C2
- Two bone blocks
Anterior Odontoid Screw
Indications:
- Type II odontoid fracture (favorable pattern)
- Non-comminuted, not too oblique
- Preserved transverse ligament
Technique:
- Anterior Smith-Robinson approach to C2-C3
- Cannulated screw from C2 body into dens
- Preserves C1-C2 rotation
Contraindications:
- Transverse fracture line (screw parallel to fracture)
- Oblique fracture (from anterosuperior to posteroinferior)
- Pathological bone

Complications
Neurological Complications
Spinal Cord Injury Progression
- Secondary injury from edema, ischemia
- Prevented by: Immobilization, MAP support, early decompression
Iatrogenic Injury
- Screw malposition (cord, nerve root, vertebral artery)
- Excessive retraction
- Decompression injury
Surgical Complications
Anterior Approach
- Dysphagia: 2-60% (usually transient)
- Recurrent laryngeal nerve palsy: 2-11% (hoarseness)
- Esophageal injury: Rare but serious
- Vascular injury: Carotid, vertebral artery
Posterior Approach
- Vertebral artery injury: 0.1-4% (C2 pedicle screws highest risk)
- C5 palsy: 2-16% (deltoid weakness)
- Wound infection: 1-3%
Hardware Complications
- Screw pullout
- Rod fracture
- Cage subsidence
- Plate migration
Fusion Complications
Nonunion (Pseudarthrosis)
- Risk factors: Smoking, multilevel, osteoporosis
- Higher in upper cervical injuries
Adjacent Segment Disease
- Increased stress on adjacent levels
- May require extension of fusion
Medical Complications
- DVT/PE (high risk in SCI)
- Pneumonia (especially high cervical SCI)
- Pressure ulcers
- Autonomic dysreflexia (injuries above T6)
Postoperative Care
Immediate
- Neuromonitoring: hourly motor/sensory checks for 24-48h; low threshold for urgent MRI if any deterioration (exclude haematoma)
- Airway: anterior surgery risks airway swelling - consider delayed extubation, swallow assessment for dysphagia
- Haemodynamics: maintain MAP ~85-90 mmHg in SCI; watch for neurogenic shock
Immobilisation & Rehabilitation
- Rigid collar typically 6-12 weeks after fusion (construct-dependent); halo pin care with daily cleaning and torque checks where used
- Early mobilisation when fixation is stable, with physiotherapy and occupational therapy; SCI patients transfer to a specialist unit for multidisciplinary rehabilitation, bladder/bowel and skin programmes
Follow-up
- 2 weeks wound check, 6 weeks clinical review with flexion-extension films, 3 months fusion assessment, 12 months final outcome and CT for fusion
Outcomes
Neurological Recovery
- Complete SCI (ASIA A): poor prognosis for significant motor recovery; rehabilitation focuses on adaptation and ADLs
- Incomplete SCI (ASIA B-D): better prognosis, improved further by early decompression (STASCIS); central cord syndrome characteristically recovers legs before hands
- Root injury: good prognosis, with meaningful improvement in the majority
Fracture-Specific & Functional
- Odontoid Type II: high halo-vest nonunion (see evidence) vs high fusion rates with surgery; Jefferson does well in a collar if TAL intact, otherwise after fusion; Hangman's Types I-II generally excellent
- Subaxial: SLIC-guided treatment with posterior instrumentation achieves high fusion rates
- Long-term: chronic neck pain and reduced ROM (especially after fusion) are common; adjacent-segment disease accrues over years
- Mortality: highest in complete SCI and in elderly odontoid fractures (high regardless of treatment), and when upper-cervical injury is associated with head injury
Differential Diagnosis
The key task is distinguishing an unstable bony or ligamentous injury (needing immobilisation and often surgery) from mimics that change management. Neck pain after trauma is never assumed benign until the spine is cleared.
| Diagnosis | Distinguishing features | Key discriminator |
|---|---|---|
| Unstable cervical fracture/dislocation | Bony fracture line on CT, malalignment, neurological deficit | CT shows fracture; MRI confirms cord/ligament injury |
| Purely ligamentous (DLC) injury | Normal or near-normal CT but persistent pain, facet widening, kyphosis on flexion | MRI shows high T2 signal in ligaments; CT can be deceptively normal |
| Ankylosing spondylitis / DISH fracture | Trivial mechanism, rigid fused spine, often transverse 'carrot-stick' fracture, frequently occult | Low threshold for whole-spine CT; highly unstable despite minor force |
| Central cord syndrome (no fracture) | Hyperextension in spondylotic spine, hands worse than legs, often no bony injury | MRI cord signal change with preserved alignment |
| Cervical sprain (whiplash) | Soft-tissue pain, full painless ROM achievable, meets NEXUS/Canadian low-risk criteria | Diagnosis of exclusion after clinical clearance |
| Os odontoideum (congenital) | Smooth corticated ossicle separate from dens, no acute fracture line | Rounded corticated margins vs sharp acute fracture edges |
| Vertebral artery injury | Fracture through foramen transversarium, facet subluxation, posterior-circulation symptoms | CT angiography |
Controversies & Areas of Uncertainty
- MRI before closed reduction of facet dislocation: Up to 40-50% of facet dislocations harbour a traumatic disc herniation. Whether to obtain MRI first (to avoid pushing disc into the canal) or to reduce immediately in an awake patient (to decompress the cord sooner) remains debated; many centres reduce awake when MRI would cause significant delay and the patient is deteriorating.
- Elderly Type II odontoid fracture - operative vs non-operative: Surgery improves union rates but carries operative risk, while non-operative care accepts a high rate of stable fibrous nonunion. Mortality is high regardless of treatment, so management is individualised by physiological reserve and patient goals rather than age alone.
- Steroids in acute SCI: Although NASCIS suggested a marginal subgroup benefit, AANS/CNS now recommend against routine methylprednisolone; some clinicians still consider it case-by-case despite the complication signal.
- Timing of decompression: STASCIS supports decompression within 24 hours, but the practical definition of "early" and the benefit in complete injuries or polytrauma remain debated.
- SLIC score of 4: The 3-4 range is deliberately equivocal; treatment is surgeon discretion, and reliability of the disco-ligamentous component is the weakest part of the score.
- Collar vs halo for stable upper-cervical injuries: Halo immobilisation is poorly tolerated in the elderly (pneumonia, pressure sores), and many now favour a rigid collar or early surgery over prolonged halo use.
- MRI clearance of the obtunded patient: With modern multidetector CT, the added value of routine MRI to clear the cervical spine in the obtunded but neurologically intact patient is contested.
Evidence Base
STASCIS - Timing of Decompression in Cervical SCI
- Prospective multicentre cohort, 313 adults with acute cervical SCI; 182 early (mean 14.2h) vs 131 late (mean 48.3h) decompression
- 19.8% of early-surgery patients achieved 2 or more grade ASIA improvement at 6 months vs 8.8% with late surgery (adjusted OR 2.83, 95% CI 1.10-7.28)
- Complication rates similar (24.2% early vs 30.5% late, p=0.21)
- Decompression before 24h is safe and associated with improved neurological recovery
NASCIS III - Methylprednisolone in Acute SCI
- Double-blind RCT, 499 patients within 8h of acute SCI; 24h vs 48h methylprednisolone vs 48h tirilazad
- 48h regimen improved motor recovery only in the subgroup treated 3-8h after injury
- 48h steroid associated with more severe sepsis and severe pneumonia
- Marginal benefit and complication signal led AANS/CNS to recommend AGAINST routine use
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An 80-year-old man falls and has neck pain. CT shows a fracture at the base of the odontoid (Type II). How do you manage?”
“A 45-year-old presents following a motor vehicle accident with severe neck pain and neurological deficit. He has reduced power in his hands bilaterally (4/5) but normal lower limb power and sensation. CT cervical spine shows bilateral facet dislocation at C5-C6 with significant anterior translation. You classify this as ASIA C incomplete spinal cord injury. The neurosurgical team asks whether you want to proceed with closed reduction in the emergency department or obtain an MRI first. What are the key considerations and how would you proceed?”
“A 52-year-old underwent posterior cervical fusion C4-C7 with lateral mass screw fixation yesterday for a burst fracture of C5 with SLIC score of 6. Pre-operatively he had intact neurology (ASIA E). Post-operative day 1, he reports new onset weakness in both shoulders. On examination, you find bilateral deltoid weakness (3/5) and biceps weakness (3/5), but normal triceps, wrist extensors, and hand function. Sensation is intact. He is otherwise well with stable vital signs and no wound issues. What is your differential diagnosis and how would you manage this?”
MCQ Practice Points
Q: What are the Canadian C-Spine Rules for determining need for radiography?
A: High-risk factors (mandates imaging): Age 65+; Dangerous mechanism (fall greater than 1m, axial load to head, MVC greater than 100km/h, rollover, ejection, bicycle struck by vehicle); Paresthesias in extremities. Low-risk factors (allows ROM assessment): Simple rear-end MVC, sitting in ED, ambulatory, delayed pain onset, no midline tenderness. If low-risk present AND can actively rotate neck 45° L and R = no imaging needed. High sensitivity for clinically significant injury.
Q: What is the classification of upper cervical (C0-C2) injuries?
A: Occipital condyle fractures (Anderson & Montesano): Types I-III based on mechanism. Atlantooccipital dissociation (Traynelis): Type I-III based on direction. C1 ring fractures (Jefferson): Burst pattern from axial load. Odontoid fractures (Anderson & D'Alonzo): Type I (tip), II (waist - most common, highest nonunion), III (body). Hangman's fracture (Levine & Edwards): Bilateral C2 pars fractures, Types I-III.
Q: What is the SLIC classification for subaxial cervical spine injuries?
A: Subaxial Injury Classification (SLIC) guides treatment. Morphology: Compression (1), Burst (2), Distraction (3), Translation/Rotation (4). Disco-ligamentous complex (DLC): Intact (0), Indeterminate (1), Disrupted (2). Neurological status: Intact (0), Root injury (1), Complete cord (2), Incomplete cord (3), Ongoing compression with deficit (+1). Total score: Less than 4 = non-operative; 4 = surgeon discretion; greater than 4 = operative.
Q: What imaging is recommended for cervical spine trauma evaluation?
A: CT cervical spine: First-line imaging for all significant trauma; Includes skull base to T1; Superior to plain films for bony injury. MRI: Indicated for neurological deficit; Assesses spinal cord, disc herniation, ligamentous injury (DLC); Timing controversial but generally within 24-72 hours. CT angiography: If vertebral artery injury suspected (fracture through foramen transversarium, facet subluxation). Flexion-extension X-rays: Rarely used acutely; May assess stability after collar period.
Q: What are the principles of initial management of cervical spine injuries?
A: Immobilization: Rigid collar (properly sized), log-roll precautions, in-line stabilization. Airway: Early intubation if needed using in-line stabilization (avoid neck extension). Methylprednisolone: Previously standard, now not recommended (AANS/CNS guidelines - risks outweigh benefits). Maintain MAP: Greater than 85-90 mmHg for spinal cord injury to optimize perfusion. Early surgery: Consider for incomplete SCI with ongoing compression, deteriorating neurology, unstable injuries. DVT prophylaxis: High risk population.
Guidelines, Registries & Global Practice
Global Epidemiology
- Bimodal age distribution: a young-male peak (high-energy road traffic and sports/diving trauma) and an older peak (low-energy falls, often on osteoporotic or ankylosed spines)
- Cervical spine is the most common level of traumatic spinal cord injury, and the proportion of geriatric, fall-related injury is rising worldwide as populations age
- Odontoid fractures are the single most common cervical fracture in patients over 70, frequently from a simple ground-level fall
- Mechanism shift by setting: high-income/ageing populations are dominated by elderly falls; younger road-traffic and diving injuries predominate in many low- and middle-income settings
Side-by-Side Guidelines
- Focus
- Acute SCI management
- Key position
- Recommend against routine high-dose methylprednisolone; support MAP augmentation (target ~85-90 mmHg)
- Focus
- Timing & classification
- Key position
- Early decompression (within 24h) for traumatic cervical SCI; AOSpine subaxial and upper-cervical classifications for communication
- Focus
- Spinal trauma pathways
- Key position
- Selective CT clearance, MRI for neurology/obtunded; consultant-led pathways and specialist transfer
- Focus
- Clearance imaging
- Key position
- CT first-line in significant trauma; clinical clearance via NEXUS / Canadian C-Spine Rule in alert, low-risk patients
Decision Rules for Imaging
- NEXUS and the Canadian C-Spine Rule are the two validated tools for clinical clearance in alert, stable patients; the Canadian rule is more specific (fewer images) while both have very high sensitivity
- CT is first-line whenever imaging is indicated; MRI is reserved for neurological deficit, obtunded patients, or suspected disco-ligamentous injury
High- vs Limited-Resource Practice Variation
- Well-resourced systems: rapid CT and MRI access, dedicated spinal-injury units, early (within 24h) decompression, and structured multidisciplinary rehabilitation
- Limited-resource settings: greater reliance on plain radiographs and clinical decision rules, prolonged collar/halo immobilisation where surgical capacity is constrained, and longer pre-hospital times that increase the importance of meticulous immobilisation and transfer
- Ankylosing spinal disorders (ankylosing spondylitis, DISH) demand a low threshold for CT (often the whole spine) everywhere, as fractures are frequently occult, highly unstable, and easily missed on plain films
Immediate Management
- ATLS immobilization
- Rigid collar until cleared
- CT then MRI if indicated
Upper Cervical
- Jefferson (C1 burst): TAL integrity key
- Odontoid Type II: High nonunion, often surgery
- Hangman: Often neurologically intact
SLIC (Subaxial)
- Score morphology, DLC, neurology
- Score greater than or equal to 5 = surgery
- Less than 3 = conservative
Surgical Options
- Anterior: Corpectomy, ACDF
- Posterior: Lateral mass screws, fusion