Idiopathic and Post-SCFE
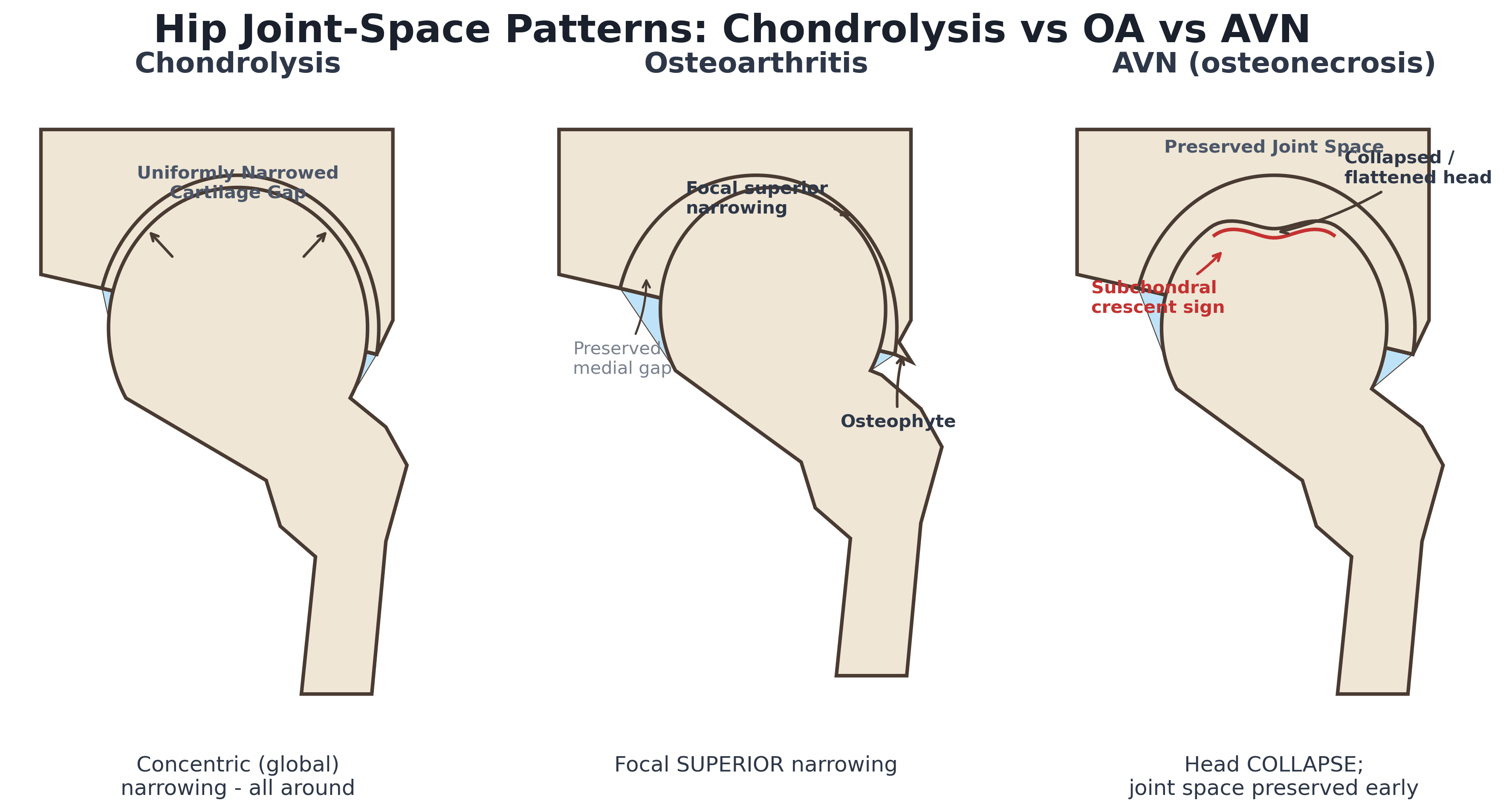
- Chondrolysis of the hip is a rapid loss of the articular cartilage producing CONCENTRIC (global, all-around) joint-space narrowing - this concentric pattern is the key radiographic feature that distinguishes it from osteoarthritis (focal, usually superior loss) and from avascular necrosis (femoral head collapse with preserved or asymmetric joint space early on); the clinical picture is a stiff, painful hip with reduced range of motion and contracture.
- IDIOPATHIC chondrolysis of the hip (ICH) typically affects ADOLESCENTS (classically girls), presenting with a single painful stiff hip, a claudication (antalgic) gait and pelvic tilt without specific clinical signs; crucially the inflammatory and infective work-up is NORMAL (normal blood count, ESR, CRP, rheumatoid factor, autoimmune tests and TB tests), so it is a DIAGNOSIS OF EXCLUSION.
- ICH has a HIGH MISDIAGNOSIS RATE because there are no specific clinical or laboratory tests, so EARLY MRI is a critical reference for diagnosis (it shows cartilage loss, effusion and often surrounding marrow/soft-tissue changes before the radiographic joint space narrows); the disease can progress rapidly to joint degeneration or ankylosis in adolescence if not treated.
- POST-SCFE chondrolysis is chondrolysis complicating slipped capital femoral epiphysis; the classic and most important avoidable association is PIN or IMPLANT PENETRATION of the joint (persistent, often unrecognised, intra-articular hardware), so intra-operative and post-operative confirmation that the implant is NOT in the joint (multiplanar imaging / approach-withdrawal technique) is a key preventive step - although chondrolysis is also reported after SCFE without documented penetration.
- MANAGEMENT is largely NON-OPERATIVE and aimed at preserving motion and controlling inflammation: rest/protected weight-bearing, anti-inflammatory measures, physiotherapy to maintain range, and traction/manipulation; in post-SCFE cases any intra-articular hardware must be removed. Evidence supports active early treatment - intra-articular steroid, manipulation and traction immobilisation improve pain and function, and earlier-stage disease responds best (late/Stage III narrowing is hard to reverse).
- Outcomes range across a spectrum from full recovery to fibrous ANKYLOSIS; the earlier the (MRI) stage at which treatment starts, the better the outcome, and end-stage hips with painful stiffness or ankylosis may ultimately require salvage (e.g. arthrodesis or, in the mature skeleton, arthroplasty) - so the emphasis is on early recognition and joint-preserving treatment.
- “Chondrolysis = rapid cartilage loss with CONCENTRIC (global) joint-space narrowing - the pattern that distinguishes it from OA (focal/superior) and AVN (head collapse).
- “Idiopathic chondrolysis = adolescent (often girl), stiff painful hip, NORMAL inflammatory markers (diagnosis of exclusion); EARLY MRI is key.
- “Post-SCFE chondrolysis is classically linked to PIN/IMPLANT JOINT PENETRATION - confirm hardware is out of the joint; management mainly non-operative, earlier responds best.
Concentric (global) joint-space narrowing in a stiff, painful adolescent hip - not the focal superior loss of OA, not the head collapse of AVN. Inflammatory markers are normal.
In a post-SCFE hip, exclude pin/implant penetration of the joint; in an otherwise-well adolescent, think idiopathic chondrolysis and get an early MRI.
Recognition, Causes & Imaging
Chondrolysis is a rapid loss of articular cartilage of the hip, producing concentric (global, all-around) joint-space narrowing - the pattern that distinguishes it from the focal superior loss of osteoarthritis and from the head collapse of avascular necrosis. Clinically the hip is stiff and painful with reduced range and contracture. Idiopathic chondrolysis (ICH) affects adolescents (classically girls) with a single painful stiff hip, claudication and pelvic tilt and is a diagnosis of exclusion - the inflammatory and infective work-up (FBC, ESR, CRP, rheumatoid factor, autoimmune and TB tests) is normal. Because there are no specific tests and the misdiagnosis rate is high, early MRI is critical. The other key form is post-SCFE chondrolysis, classically associated with pin or implant penetration of the joint.
Put a number on it. The conventional radiographic threshold is a joint space of less than about 3 mm, or a loss of more than half the joint space compared with the contralateral hip — measured on a properly positioned AP pelvis so the comparison is fair. That quantitative definition is what separates "narrowed" from "chondrolysis" when the examiner asks how you would prove it.
The causes worth listing. Idiopathic and post-SCFE dominate paediatric practice, but chondrolysis is best understood as a final common pathway with several triggers: prolonged immobilisation or joint distraction, untreated sepsis, inflammatory arthritis, trauma, burns, and — importantly for the adult surgeon — iatrogenic chondrotoxicity. The best-recognised iatrogenic form is post-arthroscopic glenohumeral chondrolysis, in which a continuous intra-articular infusion of local anaesthetic (classically bupivacaine via a "pain pump"), with or without thermal or radiofrequency energy, destroys the articular cartilage over months. Local anaesthetic chondrotoxicity is concentration- and duration-dependent, which is why continuous intra-articular catheters have been abandoned. A single injection is a different exposure from a 48-hour infusion — a distinction worth making explicitly if asked.
Why the Cartilage Is Lost: Proposed Pathophysiology
The aetiology is genuinely uncertain, which is why treatment remains anti-inflammatory and immunomodulatory rather than targeted. Two broad mechanisms are proposed, and both are worth knowing.
- An immune / inflammatory mechanism (idiopathic form). An abnormal, probably autoimmune, response directed at the articular cartilage is proposed: synovial inflammation with a lymphoplasmacytic infiltrate and raised intra-articular immunoglobulins/complement have been reported, and this inflammatory hypothesis is the rationale for the intra-articular steroid and the recombinant TNF-receptor fusion protein used in the cited series.
- A mechanical mechanism (post-SCFE form). Direct chondral injury from an intra-articular pin/implant is the classic avoidable trigger; even without documented penetration, the altered joint mechanics and increased contact stress of the slip deformity, plus raised intra-articular pressure, can drive cartilage loss.
- Other reported associations: prolonged immobilisation, trauma and severe burns - but many idiopathic cases have no identifiable trigger.
- The common pathway. Whatever the trigger, accelerated chondrocyte and matrix loss thins the cartilage globally, giving the concentric narrowing, capsular contracture and - if unchecked - fibrous ankylosis; this is also why treatment that calms inflammation and preserves motion works best before the cartilage is irreversibly lost.
Cause is uncertain: an immune/inflammatory attack on cartilage (idiopathic - hence steroid/anti-TNF is tried) versus a mechanical insult (post-SCFE pin penetration or the slip's increased contact stress). Both end in global cartilage loss = concentric narrowing, which is why the disease behaves so differently from the focal loss of OA. (The underlying cartilage matrix biology is developed in our Articular Cartilage topics.)
Differential of the Stiff Adolescent Hip with Concentric Narrowing
Because idiopathic chondrolysis is a diagnosis of exclusion, the examinable skill is the structured differential of a stiff, painful adolescent hip with global joint-space loss - and how each is told apart.
- Discriminating features
- CONCENTRIC global narrowing, NORMAL inflammatory markers, MRI cartilage loss/effusion; ask about prior SCFE and intra-articular hardware
- The test that settles it
- Normal CRP/ESR/WCC with concentric narrowing - a diagnosis of exclusion once infection is off the table
- Discriminating features
- Can also narrow concentrically and destroy, but RAISED CRP/ESR/WCC (TB more indolent, contact history)
- The test that settles it
- Aspiration with Gram stain, culture and cell count; add mycobacterial culture and PCR if indolent
- Discriminating features
- Often polyarticular, morning stiffness, uveitis, systemic features
- The test that settles it
- Raised inflammatory markers and serology, plus a slit-lamp examination for uveitis
- Discriminating features
- Femoral-head COLLAPSE / crescent sign with relatively preserved joint space early (NOT concentric)
- The test that settles it
- MRI showing a focal subchondral lesion rather than global cartilage loss
- Discriminating features
- Younger child; epiphyseal sclerosis and fragmentation rather than pure cartilage loss
- The test that settles it
- Radiographic epiphyseal changes with an age that fits (typically the younger child)
- Discriminating features
- Effusion with juxta-articular erosions
- The test that settles it
- Gradient-echo MRI blooming from haemosiderin - the finding that names it
- Discriminating features
- Recurrent haemarthrosis, characteristic chronic changes
- The test that settles it
- Coagulation screen and factor assay; the bleeding history usually precedes the hip
Each of these is developed separately in septic arthritis of the paediatric hip, tuberculous arthritis, juvenile idiopathic arthritis, avascular necrosis of the hip, Legg-Calve-Perthes disease, PVNS and haemophilia.
The single fastest discriminator is the inflammatory work-up: it is normal in chondrolysis and raised in septic/tuberculous arthritis and JIA. Then the pattern separates the rest - chondrolysis is concentric cartilage loss, AVN is head collapse, Perthes is epiphyseal fragmentation. Always ask about a treated SCFE and possible intra-articular hardware before settling on idiopathic chondrolysis.
Management
- Largely non-operative. Rest/protected weight-bearing, anti-inflammatory measures, and physiotherapy to maintain range; traction/manipulation to preserve and recover motion.
- Treat early. Evidence supports active early treatment - intra-articular steroid injection, manipulation and traction immobilisation improve pain and function; earlier-stage disease responds best, and late (Stage III) narrowing is hard to reverse.
- Remove intra-articular hardware. In post-SCFE chondrolysis, any pin/implant penetrating the joint must be removed; confirm at the index operation that hardware is not intra-articular.
- Salvage for end-stage. Painful stiffness or ankylosis may need salvage - arthrodesis, or arthroplasty in the mature skeleton - but the priority is early recognition and joint preservation.
Two reflexes prevent missed or worsened chondrolysis. First, recognise the CONCENTRIC joint-space narrowing: because chondrolysis loses cartilage all around the joint rather than focally, a young patient with global narrowing and a stiff hip should prompt the diagnosis and an early MRI rather than being labelled as early osteoarthritis or transient synovitis. Second, in any hip treated for SCFE, actively EXCLUDE intra-articular implant penetration: unrecognised hardware in the joint is the classic, avoidable cause of post-SCFE chondrolysis, so confirm with multiplanar imaging at surgery and remove any penetrating implant. Because the disease can progress rapidly to ankylosis, early diagnosis and joint-preserving treatment are what protect the hip.
Mnemonics & Memory Aids
CHONDRO
Hook:CHONDRO: Concentric narrowing, Hip stiff, Of exclusion, Note SCFE/pin, Diagnose on MRI, preserve Range, Outcome depends on early treatment.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“An adolescent has a stiff, painful hip with concentric joint-space narrowing on X-ray and normal blood tests. What is your differential and diagnosis?”
“How would you manage chondrolysis of the hip?”
Recognition
- Rapid cartilage loss -> CONCENTRIC (global) joint-space narrowing
- Stiff, painful hip; reduced range, contracture, claudication, pelvic tilt
- Distinguish from OA (focal/superior) and AVN (head collapse)
Idiopathic (ICH)
- Adolescents (classically girls); single hip
- NORMAL inflammatory/infective work-up - diagnosis of exclusion
- Early MRI critical (high misdiagnosis rate; stage guides prognosis)
Post-SCFE
- Complicates slipped capital femoral epiphysis
- Classic avoidable cause: intra-articular pin/implant penetration
- Confirm hardware not in joint; remove if penetrating
Management
- Largely non-operative: rest, anti-inflammatories, physio, traction/manipulation
- Active early treatment (intra-articular steroid, manipulation) - earlier responds best
- End-stage ankylosis -> salvage (arthrodesis; arthroplasty if mature)
Evidence & Key Studies
Diagnosis and treatment of idiopathic chondrolysis of the hip
- Idiopathic chondrolysis of the hip presents with single hip pain, claudication gait and pelvic tilt without specific clinical signs, and with NORMAL laboratory tests (FBC, ESR, CRP, rheumatoid factor, autoimmune and TB tests) - so it has a high misdiagnosis rate and early MRI is a critical reference for diagnosis.
- The disease can progress rapidly, with joint degeneration or ankylosis in adolescence without effective treatment; an MRI staging (Camarnat) was used and earlier stages responded better.
- Active treatment (here including a TNF-receptor fusion protein and, in one case, anterior capsular release) helped earlier-stage disease, while late (Stage III) narrowing responded poorly.
Minimally invasive treatment for idiopathic chondrolysis of the hip: 41 cases
- Idiopathic chondrolysis of the hip is characterised by loss of the articular cartilage with a spectrum ranging from full recovery to fibrous ankylosis.
- Intra-articular steroid injection, joint manipulation and traction immobilisation significantly improved range of motion, pain (VAS) and function (CHOHES) at a minimum 2-year follow-up.
- At final follow-up 62% achieved painless mobility, supporting a minimally invasive, joint-preserving approach that reduces the need for further surgery.
The clinical picture (single hip pain, claudication, pelvic tilt), the NORMAL inflammatory/ infective work-up making it a diagnosis of exclusion, the high misdiagnosis rate, the critical early role of MRI (with staging), and the rapid progression to degeneration/ankylosis come from the cited Guan series; the cartilage-loss definition with its spectrum from full recovery to fibrous ankylosis and the benefit of minimally invasive treatment (intra-articular steroid, manipulation, traction immobilisation) from the cited Patwardhan series. The concentric-narrowing radiographic pattern (vs OA and AVN) and the classic post-SCFE association with intra-articular pin/implant penetration are standard, well-established teaching. (See also our Slipped Capital Femoral Epiphysis and Avascular Necrosis of the Hip topics.)