Beta-2 Microglobulin Amyloidosis
- Dialysis-related amyloidosis (DRA) is a distinctive amyloidosis of long-term renal-failure and DIALYSIS patients caused by accumulation of BETA-2 MICROGLOBULIN - a protein normally cleared by the kidney and only poorly removed by conventional dialysis - which forms AMYLOID FIBRILS that deposit preferentially in OSTEOARTICULAR tissue (synovium, tendons, joint capsule and bone).
- PUT THE NUMBER ON DIALYSIS VINTAGE. Among patients on haemodialysis for at least 10 YEARS, the prevalence of DRA was 68 PERCENT with conventional dialysis versus 28 PERCENT with advanced high-flux, ultrapure dialysis, and carpal tunnel syndrome, bone cysts and arthropathy all appeared significantly EARLIER in the conventional group - so modern dialysis DELAYS and REDUCES the disease but does not abolish it. The amyloid fibrils (not the monomers) are directly cytotoxic to synovial fibroblasts, which is how the joint and bone are destroyed.
- KNOW THE LIMIT OF THAT EVIDENCE. The dialysis-technology comparison is OBSERVATIONAL. A Cochrane review of 20 randomised trials (657 patients) comparing convective modalities - haemofiltration, haemodiafiltration and acetate-free biofiltration - against haemodialysis found that NO trial assessed dialysis-related amyloidosis as an outcome at all. So 'optimise the membrane to slow progression' is a biologically reasonable, observationally supported practice, not a randomised finding.
- CARPAL TUNNEL SYNDROME is a hallmark and often the earliest manifestation (amyloid in the carpal tunnel compressing the median nerve), frequently bilateral; flexor TENOSYNOVITIS and TRIGGER FINGERS are related upper-limb features - so bilateral CTS in a long-term dialysis patient should raise DRA.
- The ARTHROPATHY is a chronic, often bilateral, large-joint disease - classically of the SHOULDER (chronic pain, stiffness, rotator-cuff/capsular thickening, the soft-tissue 'shoulder-pad' sign), and also the hips, knees and wrists - with effusions and synovial thickening that can mimic inflammatory arthritis.
- The BONE and SPINE features are clinically important: SUBCHONDRAL and periarticular amyloid BONE CYSTS (well-defined lucent lesions, e.g. in the femoral neck, humeral head, carpus, acetabulum) ENLARGE over time and predispose to PATHOLOGICAL FRACTURE, and a DESTRUCTIVE (erosive) SPONDYLOARTHROPATHY (especially CERVICAL) can cause disc/endplate destruction and INSTABILITY.
- MANAGEMENT is largely supportive and SURGICAL for complications - carpal tunnel DECOMPRESSION (and tenosynovectomy/trigger-finger release), management of large-joint disease, fixation/curettage-grafting of cystic lesions and prophylaxis/treatment of pathological fracture, and stabilisation of a destructive/unstable spine - with OPTIMISATION of dialysis (high-flux/ultrapure membranes) to slow progression; and successful RENAL TRANSPLANTATION is the only treatment that removes the SOURCE, normalising serum beta-2 microglobulin and typically relieving joint symptoms quickly. BE PRECISE ABOUT WHAT TRANSPLANT DOES AND DOES NOT DO: it stops NEW amyloid forming, but the DEPOSITS ALREADY LAID DOWN PERSIST - established amyloid has been demonstrated histologically after transplantation and has caused fatal complications in the immediate post-transplant period in a patient with 27 years of dialysis. Bone cysts do not disappear, so the fracture risk they carry is not transplanted away, and a long-vintage recipient still needs surveillance. Calling transplantation a 'cure' overstates it.
- “Dialysis-related amyloidosis = BETA-2 MICROGLOBULIN amyloid deposited in osteoarticular tissue in long-term dialysis patients (impaired clearance). Risk rises with dialysis vintage; reduced (delayed) by high-flux/ultrapure dialysis.
- “Hallmarks: carpal tunnel syndrome (often first, bilateral) + flexor tenosynovitis/trigger fingers; chronic SHOULDER/large-joint arthropathy; SUBCHONDRAL BONE CYSTS (-> pathological fracture); destructive (erosive) cervical SPONDYLOARTHROPATHY.
- “Management: surgery for compression (CTS decompression), cysts/fractures and spinal instability; optimise dialysis (observational evidence - no RCT of modality has ever measured amyloidosis); TRANSPLANTATION removes the source but does NOT clear established deposits, so cysts and their fracture risk remain.
Long-term dialysis patient with bilateral carpal tunnel syndrome, chronic shoulder/large-joint arthropathy, flexor tenosynovitis/trigger fingers, and subchondral bone cysts = beta-2 microglobulin (dialysis-related) amyloidosis.
Pathological fracture through amyloid bone cysts; destructive cervical spondyloarthropathy with instability. Optimise dialysis; transplantation stops new amyloid but existing deposits persist.
Pathophysiology & Manifestations
Dialysis-related amyloidosis arises because beta-2 microglobulin - normally cleared by the kidney - is poorly removed by conventional dialysis and accumulates, forming amyloid fibrils that deposit in osteoarticular tissue. Risk rises with dialysis duration and is reduced (delayed) by high-flux/ultrapure dialysis; the fibrils are directly cytotoxic to synovial cells. The hallmark is carpal tunnel syndrome (often the first manifestation, frequently bilateral), with flexor tenosynovitis/trigger fingers; a chronic, often bilateral, large-joint arthropathy (classically the shoulder, with the 'shoulder-pad' sign); subchondral bone cysts that enlarge and predispose to pathological fracture; and a destructive (erosive) spondyloarthropathy (especially cervical) with instability risk.
The Protein and the Amyloid Classification
- What beta-2 microglobulin is. The invariant light chain of the MHC class I molecule (about 11.8 kDa), shed from all nucleated cells into the circulation; normally filtered by the glomerulus and catabolised by the proximal tubule, so in renal failure it is not cleared and serum levels rise many-fold. Conventional low-flux membranes cannot remove it (its size exceeds their pores) - high-flux/high-cutoff membranes and haemodiafiltration clear it better - and advanced-glycation (AGE) modification enhances its amyloidogenicity and its tropism for collagen-rich osteoarticular tissue.
- Where it sits in the amyloid classification. Amyloid is named by its fibril protein: Abeta2M (beta-2 microglobulin - dialysis, characteristically osteoarticular), versus the systemic AL (immunoglobulin light chain - plasma-cell dyscrasia/myeloma), AA (serum amyloid A - chronic inflammation) and ATTR (transthyretin - hereditary or wild-type). Abeta2M's strong osteoarticular predominance is what distinguishes it clinically - but predominance is not exclusivity: extra-osteoarticular deposition does occur, including in the walls of blood vessels and the gastrointestinal tract, and it has caused fatal haemorrhage in a long-vintage patient. So a dialysis patient with an unexplained visceral problem is not automatically outside the diagnosis.
Q: What is beta-2 microglobulin, and where does Abeta2M sit among the amyloids?
A: The invariant light chain of MHC class I (about 11.8 kDa), shed from all nucleated cells, normally filtered + catabolised by the proximal tubule → not cleared in renal failure (levels rise many-fold; conventional low-flux membranes cannot remove it; high-flux/haemodiafiltration do). Amyloid is named by fibril protein: Abeta2M (beta-2 microglobulin, dialysis, osteoarticular) vs systemic AL (light-chain/myeloma), AA (serum amyloid A/chronic inflammation), ATTR (transthyretin).
Differential & Imaging
- Bone cysts: well-defined lucent subchondral/periarticular lesions (femoral neck, humeral head, acetabulum, carpus) that enlarge over time - distinguish from brown tumours of hyperparathyroidism, gout and infection (correlate with the dialysis history and distribution).
- Spondyloarthropathy: destructive disc/endplate changes with relatively little osteophyte - distinguish from infective spondylodiscitis (a key mimic) and from the spondyloarthropathies.
- Arthropathy: synovial thickening/effusion mimicking inflammatory arthritis - the renal/dialysis context and cyst pattern point to amyloid.
Management
- Carpal tunnel/tenosynovitis: carpal tunnel decompression (often bilateral), tenosynovectomy and trigger-finger release.
- Bone cysts/fracture: monitor enlarging cysts; curettage and grafting and prophylactic/therapeutic fixation for impending or actual pathological fracture.
- Spine: stabilise a destructive/unstable (especially cervical) spondyloarthropathy; exclude infection.
- Large joints: symptomatic care; arthroplasty for end-stage joint disease (with awareness of bone quality).
- Optimise dialysis: high-flux/ultrapure membranes are associated with roughly half the prevalence at 10 years (28 vs 68 percent) - observational, since no randomised trial of dialysis modality has ever measured amyloidosis as an outcome.
- Transplantation: successful renal transplantation normalises beta-2 microglobulin, stops new amyloid forming and usually relieves joint symptoms quickly - but it does not clear deposits already laid down, so the bone cysts and their fracture risk remain and a long-vintage recipient still warrants surveillance.
The related conditions worth reading alongside are the ones that share the presentation. The median-nerve compression is managed as for carpal tunnel syndrome, and the digital triggering as for trigger finger, though in this population both are frequently bilateral and recur. The other skeletal consequence of renal failure, and the source of the brown tumours that mimic amyloid cysts, is renal osteodystrophy. Fixation of an impending or actual lesion follows the principles in pathologic fracture management.
The clinical key to dialysis-related amyloidosis is to recognise its pattern in a long-term dialysis patient: bilateral carpal tunnel syndrome, flexor tenosynovitis and trigger fingers, a chronic large-joint (especially shoulder) arthropathy, and subchondral bone cysts. Two complications carry particular risk. The amyloid bone cysts enlarge over time and predispose to pathological fracture (for example of the femoral neck), so enlarging cysts and impending fractures should be monitored and addressed prophylactically. The destructive spondyloarthropathy, especially in the cervical spine, can cause endplate/disc destruction and instability with the potential for neurological compromise, and it can closely mimic infective spondylodiscitis - which must be excluded - so a dialysis patient with destructive spinal changes needs careful evaluation and, where unstable, stabilisation. Surgery addresses these complications, and high-flux ultrapure dialysis is associated with roughly half the prevalence at ten years, though that comparison is observational and no randomised trial of dialysis modality has measured amyloidosis at all. Successful renal transplantation is the only treatment that removes the source, and it normalises beta-2 microglobulin and usually settles the joint symptoms - but it should not be described as clearing the disease. Deposits already laid down persist, they have been demonstrated histologically and caused fatal bleeding in the immediate post-transplant period in a patient with 27 years of dialysis, and the bone cysts and the fracture risk they carry do not resolve with the graft.
Confirming and Typing the Amyloid
- Confirming amyloid. On biopsy, amyloid stains congophilic (salmon-pink) with Congo red and shows the diagnostic apple-green birefringence under cross-polarised light - the hallmark of any amyloid.
- Typing it. Once amyloid is confirmed, the fibril protein is identified by immunohistochemistry (anti-beta-2-microglobulin antibodies) or mass spectrometry - confirming the Abeta2M type and distinguishing it from AL and AA amyloid; serum beta-2 microglobulin is high.
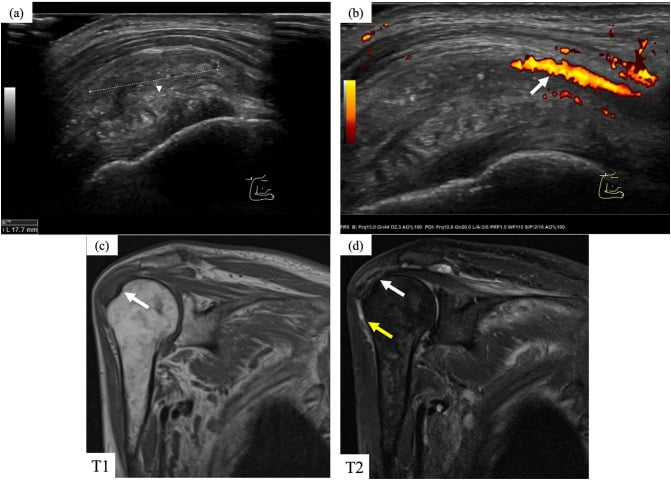
- The imaging clues. Radiographs show well-defined subchondral/periarticular lucent cysts with a thin rim, preserved joint space and no periosteal reaction; on MRI the amyloid is low signal on both T1 and T2 (unlike the T2-bright tumour, infection or inflammatory pannus), and ultrasound shows thickened synovium/cuff.
Q: How is dialysis-related amyloidosis confirmed and typed?
A: Biopsy → Congo red stain (congophilic/salmon) with apple-green birefringence under cross-polarised light = amyloid (any type); then immunohistochemistry (anti-beta-2-microglobulin) or mass spectrometry confirms the Abeta2M type (vs AL/AA); serum beta-2 microglobulin high. Imaging: well-defined subchondral cysts (thin rim, preserved joint space, no periosteal reaction); on MRI the amyloid is low signal on both T1 and T2 (unlike T2-bright tumour/infection/pannus).
Mnemonics & Memory Aids
DIALYSIS
Hook:DIALYSIS: Duration risk, Impaired beta-2 clearance, Amyloid osteoarticular, Limb CTS, shoulder arthropathY, Subchondral cysts, Instability (spine), Solution = transplant.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient on haemodialysis for 15 years has bilateral carpal tunnel syndrome, chronic shoulder pain, and femoral-neck cysts on radiograph. What is the unifying diagnosis and how do you manage it?”
Evidence & Key Studies
Impact of advanced dialysis technology on the prevalence of dialysis-related amyloidosis
- Dialysis-related amyloidosis is a unique beta-2 microglobulin amyloidosis predominantly in end-stage renal disease, with deposition in osteoarticular tissue causing carpal tunnel syndrome and destructive arthropathy with cystic bone lesions.
- In long-term (at least 10 years) haemodialysis patients, the prevalence of DRA was 68% with conventional dialysis versus 28% with advanced high-flux, ultrapure dialysis, with carpal tunnel syndrome, bone cysts and arthropathies occurring significantly earlier in the conventional group.
- Duration of dialysis was the key risk factor; advanced dialysis technology reduces and delays DRA but does not abolish it.
Beta-2 microglobulin amyloid fibrils are cytotoxic to synovial cells
- In dialysis-related amyloidosis, beta-2 microglobulin amyloid fibrils deposit in osteoarticular tissue, leading to carpal tunnel syndrome and destructive arthropathy with cystic bone lesions.
- Beta-2 microglobulin amyloid fibrils (not monomers) were cytotoxic to synovial fibroblasts, inducing necrosis and apoptosis after endocytosis and disruption of endosomal/lysosomal membranes.
- This provides a mechanism by which the amyloid fibrils destroy bone and joint tissue in dialysis-related amyloidosis.
Haemodiafiltration, haemofiltration and haemodialysis for end-stage kidney disease
- 20 randomised trials and 657 patients comparing convective extracorporeal modalities - haemofiltration, haemodiafiltration and acetate-free biofiltration - against conventional haemodialysis in end-stage kidney disease.
- No included study assessed dialysis-related amyloidosis as an outcome, so the randomised literature does not establish that a convective or high-flux technique reduces it, however plausible the mechanism.
- The convective modalities also showed no significant advantage over haemodialysis for mortality or hospital admissions, and the trials were generally small and of suboptimal quality - the reduction in amyloidosis rests on observational comparisons instead.
Beta-2 microglobulin amyloidosis and gastrointestinal bleeding after renal transplantation
- A patient with 27 years of haemodialysis developed repeated rectal bleeding from a circumferential ulcer in the immediate post-transplant period, with a fatal outcome.
- Biopsy of the ulcer stained positive with Congo red and immunohistochemistry demonstrated beta-2 microglobulin in the wall of a rectal blood vessel - established amyloid persisting and causing harm after transplantation.
- The deposits also demonstrate that this amyloidosis, though osteoarticular in emphasis, involves extra-osteoarticular tissue. As a single case it establishes that the complication can occur, not how often it does.
The nature of dialysis-related amyloidosis (beta-2 microglobulin amyloid deposition in osteoarticular tissue causing carpal tunnel syndrome and destructive arthropathy with cystic bone lesions), the strong dependence on dialysis duration, and the reduction/delay (not abolition) with advanced high-flux/ultrapure dialysis come from the cited Schiffl study; the direct cytotoxicity of the amyloid fibrils to synovial cells from the cited Okoshi study. The hallmark shoulder arthropathy ('shoulder-pad' sign), flexor tenosynovitis/trigger fingers, the predisposition of amyloid bone cysts to pathological fracture and the destructive cervical spondyloarthropathy are standard, well-established teaching. The absence of any randomised assessment of amyloidosis as an outcome of dialysis modality comes from the Cochrane review; the persistence of established deposits after transplantation, and their occurrence outside the osteoarticular system, from the Van Audenhove case. No study gives the proportion of amyloid bone cysts that go on to fracture, no threshold cyst size triggers prophylactic fixation, and no surveillance interval after transplantation has been validated, so none is quoted here.