Radial Head Fracture + IOM Disruption + DRUJ Instability | Longitudinal Forearm Instability | Do NOT Excise Radial Head
INJURY TRIAD
Critical Must-Knows
- Never excise radial head without replacement in Essex-Lopresti injury
- DRUJ must be assessed in ALL comminuted radial head fractures
- IOM central band is primary longitudinal stabilizer of forearm
- Proximal migration of radius indicates longitudinal instability
- Chronic cases extremely difficult to salvage - early diagnosis critical
Clinical Pearls
- "Mechanism: Axial load through extended wrist (FOOSH)
- "Missed diagnosis leads to irreversible proximal migration
- "Radial head replacement is essential - not optional
- "IOM reconstruction techniques are salvage procedures

Clinical Imaging
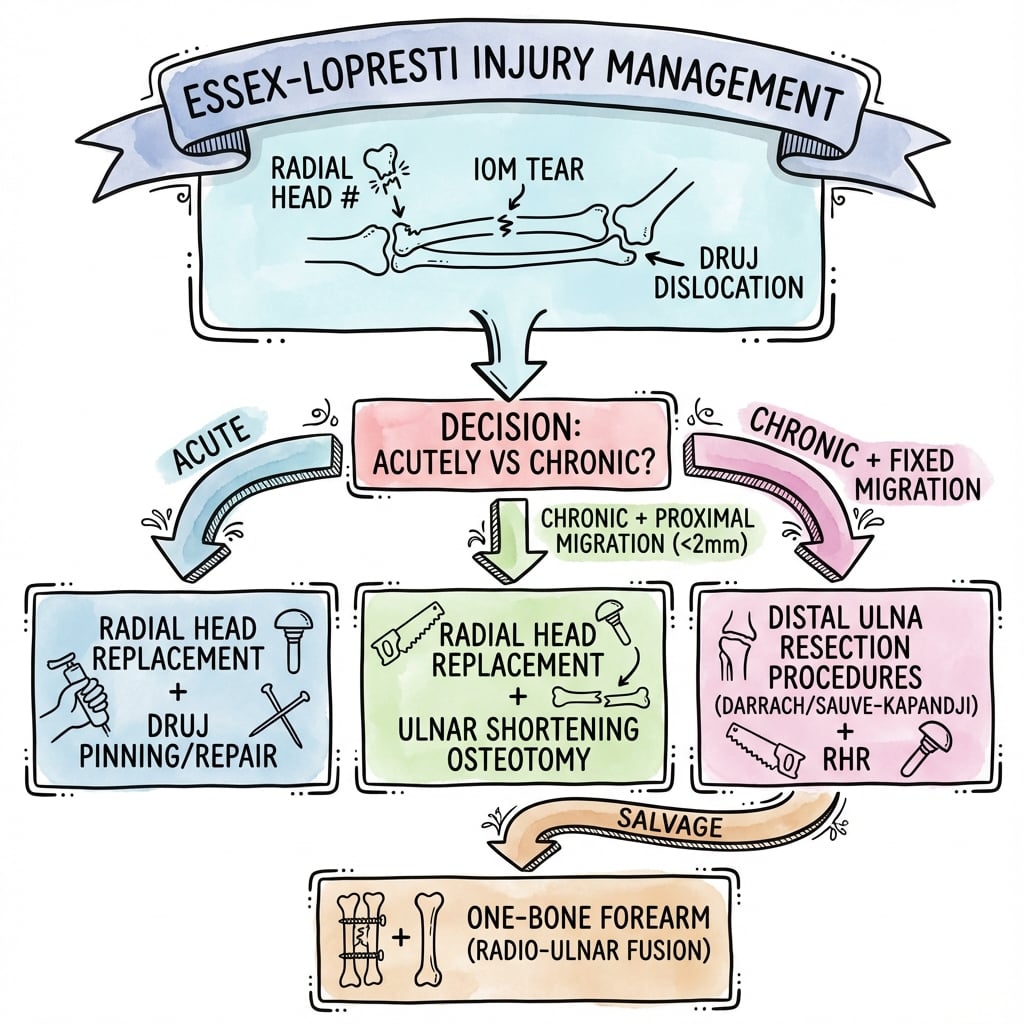
Complete Essex-Lopresti Treatment

IOM Reconstruction (Chronic Cases)

Critical Essex-Lopresti Exam Points
NEVER Excise Radial Head
Cardinal rule: In Essex-Lopresti injuries, the radial head is the ONLY remaining longitudinal stabilizer. Excision without replacement leads to inevitable proximal radial migration, ulnar impaction, and progressive pain.
Always Check DRUJ
DRUJ examination is mandatory in ALL comminuted radial head fractures. Ballottement test, piano key sign, and comparison to contralateral side. Miss this and you miss the diagnosis.
Mechanism Understanding
FOOSH with axial load transmits force through the carpus, radius, radial head, fracturing it, then continues through the IOM and DRUJ, disrupting the longitudinal stability of the forearm.
Chronic is Catastrophic
Early diagnosis is critical. Chronic Essex-Lopresti with established proximal migration is extremely difficult to treat. Results of salvage procedures are generally poor.
At a Glance - Management Decision
| Presentation | IOM Status | DRUJ | Treatment |
|---|---|---|---|
| Isolated radial head fracture | Intact | Stable | Standard radial head management |
| Acute Essex-Lopresti | Disrupted | Unstable | Radial head replacement + DRUJ stabilization |
| Chronic - minimal migration | Disrupted | Unstable | RH replacement + possible IOM reconstruction |
| Chronic - established migration | Disrupted | Unstable | Salvage: IOM reconstruction, ulnar shortening |
| End-stage with arthritis | Disrupted | Destroyed | Consider one-bone forearm or arthroplasty |
RIDEssex-Lopresti Triad
| R | Radial head fracture Usually comminuted Mason III type |
| I | Interosseous membrane Central band disruption |
| D | DRUJ disruption Distal radioulnar joint instability |
| R | Radial head fracture Usually comminuted Mason III type |
| I | Interosseous membrane Central band disruption |
| D | DRUJ disruption Distal radioulnar joint instability |
Hook:RID yourself of missing this diagnosis - always check all three components!
DRUJDRUJ Assessment
| D | Dorsal displacement Ulna prominent dorsally on exam |
| R | Radiographs Check ulnar variance and DRUJ alignment |
| U | Ulnar stress test Ballottement test in neutral rotation |
| J | Joint comparison Always compare to contralateral side |
| D | Dorsal displacement Ulna prominent dorsally on exam | U | Ulnar stress test Ballottement test in neutral rotation |
| R | Radiographs Check ulnar variance and DRUJ alignment | J | Joint comparison Always compare to contralateral side |
Hook:DRUJ tells you how to check the DRUJ!
REPLACETreatment Principles
| R | Replace radial head Metal prosthesis - never excise alone |
| E | Examine DRUJ Intraoperative stability testing |
| P | Pin DRUJ If unstable after RH replacement |
| L | Long-arm cast Protect DRUJ for 6 weeks |
| A | Assess IOM Consider reconstruction if chronic |
| C | Counsel patient Outcomes may be limited |
| E | Early motion When stable to prevent stiffness |
| R | Replace radial head Metal prosthesis - never excise alone | L | Long-arm cast Protect DRUJ for 6 weeks | E | Early motion When stable to prevent stiffness |
| E | Examine DRUJ Intraoperative stability testing | A | Assess IOM Consider reconstruction if chronic | ||
| P | Pin DRUJ If unstable after RH replacement | C | Counsel patient Outcomes may be limited |
Hook:REPLACE the radial head - it's the key to treatment!
Overview
The Essex-Lopresti injury is a rare but devastating pattern of forearm longitudinal instability characterized by radial head fracture, interosseous membrane (IOM) disruption, and distal radioulnar joint (DRUJ) instability. First described by Peter Essex-Lopresti in 1951, this injury represents complete disruption of the forearm's longitudinal stabilizing structures.
Epidemiology
Incidence:
- Less than 1% of all radial head fractures
- True incidence likely underestimated (frequently missed)
- Male predominance (high-energy mechanism)
- Most common in working-age adults (20-50 years)
Risk Factors:
- High-energy trauma
- Fall from height
- Motor vehicle accidents
- Industrial injuries
Mechanism of Injury
Primary Mechanism:
- Fall onto outstretched hand (FOOSH)
- Axial load through extended wrist
- Force transmission: Carpus to radius to radial head
Force Transmission:
- Radial head fractures under compressive load
- Force continues proximally through IOM
- Central band of IOM ruptures
- DRUJ disrupted as final stabilizer fails
Associated Injuries:
- Carpal fractures
- Capitellar injury
- Elbow dislocation
Anatomy and Pathophysiology
Forearm Longitudinal Stability
Understanding the longitudinal stabilizers of the forearm is essential for comprehending the Essex-Lopresti injury pattern.
Structure:
- Fibrous sheet connecting radius and ulna
- Fibers run obliquely (distal-ulnar to proximal-radial)
- Multiple distinct bands within the membrane
Central Band:
- Thickest and strongest portion
- Primary longitudinal stabilizer
- Located at junction of middle and proximal thirds
- Approximately 60% of longitudinal stability
Other Components:
- Proximal band (accessory band)
- Distal band
- Distal oblique bundle
Function:
- Transmits forces from radius to ulna
- Maintains radioulnar relationship
- Allows pronation and supination
The central band is the critical structure that ruptures in Essex-Lopresti injuries.
Clinical Pearl
The interosseous membrane central band provides approximately 60% of forearm longitudinal stability, while the radial head provides approximately 30%. When both are disrupted, catastrophic proximal radial migration occurs.
Classification
Classification
Essex-Lopresti Triad:
Component 1 - Radial Head Fracture:
- Usually Mason Type III (comminuted)
- May be Mason Type IV (with dislocation)
- Occasionally Type II with significant comminution
Component 2 - IOM Disruption:
- Central band rupture (primary)
- May extend to proximal band
- Diagnosed clinically and by longitudinal instability
Component 3 - DRUJ Disruption:
- TFCC tear
- Dorsal and/or palmar radioulnar ligament rupture
- Results in DRUJ instability
All three components must be present for the diagnosis.
Mason Classification with Essex-Lopresti Implications
| Mason Type | Fracture Pattern | Essex-Lopresti Risk | Management |
|---|---|---|---|
| Type I | Marginal, non-displaced | Low | Non-operative, check DRUJ |
| Type II | Marginal, displaced | Moderate | Fix or replace, check DRUJ |
| Type III | Comminuted, unreconstructable | HIGH | Replace, high index of suspicion |
| Type IV | With elbow dislocation | HIGH | Replace, very high suspicion |
Differential Diagnosis
The key discriminator is whether the forearm is longitudinally unstable (Essex-Lopresti) or stable. Isolated injuries at one end of the forearm and the other classic fracture-dislocations must be excluded.
Differential Diagnosis of Essex-Lopresti Injury
| Condition | Distinguishing feature | Key test / finding |
|---|---|---|
| Essex-Lopresti injury | Radial head fracture + IOM (central band) tear + DRUJ disruption with longitudinal instability | Positive ulnar variance vs other side; positive radial pull test |
| Isolated comminuted radial head fracture | Elbow injury only; IOM and DRUJ intact, forearm longitudinally stable | Neutral ulnar variance; negative radial pull test; no wrist pain |
| Isolated DRUJ injury / TFCC tear | Wrist instability without radial head fracture or proximal migration | DRUJ ballottement positive; normal elbow and ulnar variance |
| Galeazzi fracture-dislocation | Distal-third radial shaft fracture with DRUJ disruption | Radial shaft fracture on radiograph; radial head intact |
| Monteggia fracture-dislocation | Proximal ulnar fracture with radial head dislocation | Ulnar shaft fracture; radiocapitellar line disrupted |
| Criss-cross / atypical forearm injury | Combined radial and ulnar shaft fracture with longitudinal instability (Artiaco group) | Both shafts fractured; dynamic instability on stressing |
History
Mechanism:
- Fall from height
- Motor vehicle accident
- Fall onto outstretched hand
- Axial loading injury
Symptoms:
- Elbow pain (from radial head fracture)
- Forearm pain (often overlooked)
- Wrist pain (DRUJ involvement)
- Weakness of grip
- Pain with forearm rotation
Red Flags:
- High-energy mechanism
- Pain at both elbow AND wrist
- Significant swelling along entire forearm
- Inability to supinate/pronate
Pain at both elbow and wrist after FOOSH should raise suspicion.
Elbow Examination
Inspection:
- Swelling over lateral elbow
- Ecchymosis
- Deformity may indicate dislocation
Palpation:
- Tenderness over radial head
- Crepitus with rotation
- Assess for associated injuries
Range of Motion:
- Flexion/extension limited by pain
- Pronation/supination painful
- Mechanical block suggests loose bodies
Stability:
- Valgus stress testing
- Posterolateral rotatory drawer
- Check for associated ligament injury
Thorough elbow examination identifies the radial head fracture.
DRUJ Examination
CRITICAL - Often Missed:
Inspection:
- Ulnar head prominence
- Swelling at wrist
- Comparison to contralateral side
Palpation:
- Tenderness over DRUJ
- Tenderness over TFCC
- Ulnar styloid tenderness
Stability Tests:
- Piano key sign (dorsal prominence with pressure)
- Ballottement test (AP translation in neutral)
- Radius pull test (longitudinal instability)
- Compare to contralateral side
Forearm Squeeze Test:
- Pain at DRUJ with mid-forearm squeeze
- Indicates IOM disruption
DRUJ examination is MANDATORY in all comminuted radial head fractures.
ALWAYS examine the DRUJ in patients with comminuted radial head fractures. The Essex-Lopresti injury is frequently missed because the wrist is not examined. Pain at both elbow AND wrist should raise immediate suspicion.
Investigations
Imaging Studies
Elbow Views:
- AP and lateral of elbow
- Radial head view (45° oblique)
- Assess fracture comminution
Forearm Views:
- Full-length forearm AP and lateral
- Include both wrist and elbow
- Look for radioulnar dissociation
Wrist Views:
- PA and lateral of wrist
- Measure ulnar variance
- Positive variance suggests proximal migration
- Compare to contralateral side
Key Findings:
- Comminuted radial head fracture
- Positive ulnar variance (proximal migration)
- DRUJ widening or subluxation
- Ulnar impaction changes if chronic
Full-length forearm films are essential to assess longitudinal instability.
Clinical Pearl
Positive ulnar variance on wrist radiographs indicates proximal radial migration. Always compare to the contralateral side and obtain full-length forearm films to assess longitudinal instability.
Management Algorithm
Treatment Decision Making
Surgical Treatment (Standard of Care):
Step 1 - Radial Head:
- ORIF if reconstructable (rare in Essex-Lopresti)
- Replacement with metal prosthesis if comminuted
- NEVER excise without replacement
Step 2 - Assess DRUJ Intraoperatively:
- After radial head addressed, test DRUJ stability
- Ballottement in neutral rotation
- Compare to contralateral side
Step 3 - DRUJ Stabilization:
- If stable: immobilize in supination 4-6 weeks
- If unstable: transfix with K-wires or suture repair
- Long-arm cast in supination
Post-operative:
- Long-arm cast 4-6 weeks
- Elbow motion can begin earlier
- Forearm rotation protected
Acute surgical treatment focuses on radial head replacement and DRUJ stabilization.
Acute Principles
Goals:
- Replace radial head
- Restore length
- Stabilize DRUJ
- Protect healing
Timing:
- Surgery within 2 weeks ideal
- Earlier is better
- Delayed surgery associated with worse outcomes
Avoid These Errors
Critical Mistakes:
- Excising radial head without replacement
- Missing the DRUJ injury
- Inadequate immobilization
- Failing to assess longitudinal stability
Consequences:
- Irreversible proximal migration
- Ulnar impaction syndrome
- Chronic pain and disability
Surgical Technique
Operative Procedures
Patient Positioning:
- Supine with arm on hand table
- Tourniquet on upper arm
- Fluoroscopy available
Approach:
- Kocher approach (between anconeus and ECU)
- Protect lateral ulnar collateral ligament
- Identify and preserve annular ligament
Technique:
- Excise radial head fragments
- Preserve annular ligament remnants
- Ream medullary canal
- Trial implant sizing
- Confirm length with fluoroscopy
- Seat final implant
- Close annular ligament if possible
Intraoperative Assessment:
- Full ROM without impingement
- Stable tracking
- Test DRUJ stability
Radial head replacement technique is critical for successful outcome.
Clinical Pearl
When sizing the radial head prosthesis, the lateral ulnohumeral joint should be restored. Overlengthening causes capitellar wear and pain; underlengthening fails to prevent proximal migration.
Complications
Potential Complications
Most Common Problem:
- Failure to examine DRUJ
- Isolated radial head excision performed
- Progressive proximal migration
Consequences:
- Ulnar impaction syndrome
- Wrist pain
- Grip weakness
- Chronic forearm instability
Prevention:
- High index of suspicion
- Examine DRUJ in ALL comminuted RH fractures
- Full-length forearm radiographs
Missed diagnosis is the most common and devastating complication.
Radial head excision without replacement in Essex-Lopresti injury leads to inevitable proximal radial migration and chronic disability. This error is essentially irreversible - prevention through proper diagnosis is key.
Postoperative Care
Rehabilitation Protocol
Goals:
- Protect DRUJ stability
- Allow soft tissue healing
- Prevent proximal migration
Immobilization:
- Long-arm cast or splint
- Forearm in supination
- Elbow at 90 degrees
Motion:
- Elbow flexion/extension out of cast (if stable)
- No forearm rotation
- Shoulder and hand exercises
K-wire Removal:
- If DRUJ pinned, remove at 6 weeks
- Under local anesthesia
Protection phase prioritizes DRUJ healing.
Outcomes
Expected Results
Early Diagnosis and Treatment:
- Fair to good outcomes in 60-80%
- Better than chronic treatment
- Restoration of stability achievable
Functional Outcomes:
- ROM: Usually 80-90% of contralateral
- Grip strength: 70-80% of contralateral
- Return to work: Variable, often with restrictions
Complications:
- Migration despite treatment: 10-30%
- Revision surgery: 15-25%
- Chronic pain: 20-40%
Acute treatment provides best chance for acceptable outcome.
Evidence Base
Key Studies
Essex-Lopresti - Original Description
- First description of the injury pattern (two cases)
- Comminuted radial head fracture with radial head excision followed by proximal radial migration
- Recognised the link between radial head loss, forearm length and distal radioulnar joint disruption
- Emphasised the need to recognise the whole forearm injury, not just the elbow
Hotchkiss et al. - IOM Biomechanics (landmark)
- Anatomic and mechanical cadaver study (12 specimens) of the interosseous membrane
- Central band identified in all specimens, approximately twice the thickness of adjacent membrane
- Central band provided 71% of forearm longitudinal stiffness after radial head excision; the TFCC contributed 8%
- Silicone radial head implants were far less stiff than the intact membrane - central band injury is key to proximal radial migration
Skahen et al. - Central Band Reconstruction (cadaver)
- Cadaver study (12 forearms) of central band strain and reconstruction
- Central band strain greatest in pronation and increased significantly after radial head excision
- Both central band and TFCC are important to axial forearm stability
- Flexor-carpi-radialis-based central band reconstruction prevented complete radial migration but did not fully restore longitudinal stability
Marcotte and Osterman - LRUD Treatment Algorithm
- Concepts in anatomy, biomechanics, diagnosis and treatment of longitudinal radioulnar dissociation
- Reports encouraging results for chronic injury treated by bone-ligament-bone (patellar tendon) central band reconstruction
- Provides a treatment algorithm for acute and chronic injury
- Frames the forearm as a single functional unit requiring length and stability restoration
Sheth et al. - Narrative Review
- Contemporary narrative review of Essex-Lopresti and longitudinal radioulnar instability
- Acute management centres on restoring radial length and temporary DRUJ stabilisation
- Radial head excision in the acute setting should be approached with caution - migration may develop over time
- Indications for acute IOM repair/reconstruction remain unclear; central band reconstruction can restore load transfer in chronic cases
Kooistra et al. - Definition Heterogeneity (systematic review)
- PRISMA systematic review: 47 clinical studies, 266 patients
- 39 of 47 studies did not even mention an IOM lesion as part of the injury
- Threshold for significant positive ulnar variance ranged from more than 1 mm to more than 12 mm across studies
- Only 9 studies used any dynamic intraoperative test of longitudinal stability
Meglic et al. - IOM Role and Radial Pull Test
- ESSKA instructional review of the interosseous membrane in post-traumatic forearm instability
- Describes the intraoperative radial pull test to improve detection of IOM injury
- Reframes the forearm as a functional unit and proposes the Artiaco classification of forearm fracture-dislocations
- Provides a management flowchart for acute and chronic forearm instability
Viva Scenarios
Viva Scenarios
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Acute Diagnosis
"A 35-year-old man falls from a ladder onto his outstretched hand. He has a comminuted radial head fracture. How would you assess for an Essex-Lopresti injury?"
Acute Management
"You have confirmed an Essex-Lopresti injury in the patient from the previous scenario. What is your surgical plan?"
Missed Injury (Chronic)
"A patient presents 6 months after a radial head excision for what was thought to be an isolated comminuted radial head fracture. He now has wrist pain and grip weakness. Radiographs show 8mm positive ulnar variance. What has happened and how would you manage this?"
Functional Anatomy
"Describe the anatomy of the interosseous membrane and its role in forearm stability."
MCQ Practice
High-Yield Exam Points
Key Point
Q: What is the most important examination to perform in a patient with a comminuted radial head fracture?
A: DRUJ stability assessment is CRITICAL in all comminuted radial head fractures to rule out Essex-Lopresti injury. Use ballottement test, piano key sign, and always compare to the contralateral side. Missing this examination leads to missed diagnosis with catastrophic consequences.
Key Point
Q: In an acute Essex-Lopresti injury, what is the most important surgical intervention and why?
A: Radial head replacement is essential. The radial head is the only remaining longitudinal stabilizer after IOM rupture. Excision without replacement leads to inevitable proximal radial migration, ulnar impaction, and chronic disability. This is a NEVER excise scenario.
Key Point
Q: What percentage of forearm longitudinal stability is provided by the IOM central band versus the radial head?
A: The IOM central band provides approximately 60-70% of forearm longitudinal stability, while the radial head provides approximately 30%. When both are disrupted, catastrophic instability results with proximal migration of the radius.
Key Point
Q: What is the most common reason Essex-Lopresti injuries are missed, and how can this be prevented?
A: Failure to examine the DRUJ is the most common reason these injuries are missed. The wrist is simply not examined in patients presenting with elbow injuries. Prevention: ALWAYS perform DRUJ examination in ALL comminuted radial head fractures and obtain full-length forearm radiographs.
Key Point
Q: A patient had radial head excision 6 months ago. Now has wrist pain and 7mm positive ulnar variance. What happened and what are the management options?
A: This is a missed Essex-Lopresti injury with established proximal migration. Management options include: 1) Radial head replacement + IOM reconstruction (best salvage option), 2) Ulnar shortening osteotomy + DRUJ procedure, 3) One-bone forearm (extreme salvage). All have poor outcomes compared to acute treatment - this emphasizes the critical importance of early diagnosis.
Key Point
Q: How do you assess DRUJ stability intraoperatively after radial head replacement?
A: Test DRUJ stability in neutral rotation using ballottement test. Compare to contralateral side. If stable, immobilize in supination for 6 weeks. If unstable, perform K-wire transfixion with 2 parallel wires from radius to ulna, forearm in supination, or consider direct TFCC repair.
Guidelines, Registries & Global Practice
Global Practice, Guidelines and Evidence
Essex-Lopresti injury (also termed longitudinal radioulnar dissociation) is a rare, globally relevant pattern. There is no internationally agreed definition and no high-level (RCT) guideline, so practice rests on cadaver biomechanics, case series and expert consensus reviews. The world standard of care is consistent: in a comminuted radial head fracture, actively exclude longitudinal instability, restore radial length, stabilise the DRUJ, and avoid radial head excision.
Epidemiology (global)
- Accounts for less than 1% of radial head fractures and is widely under-recognised; mechanism is axial load through an extended wrist (fall onto the outstretched hand, fall from height, motor-vehicle and industrial trauma).
- Typically affects working-age adults with a male predominance, reflecting the high-energy mechanism.
- A PRISMA systematic review found only 266 reported patients across 47 studies, and most studies did not document the interosseous-membrane component - the literature base is small and heterogeneous (Kooistra et al., EFORT Open Rev 2022).
Guidance and consensus, side by side
How major bodies frame longitudinal forearm instability
| Body / source | Position | Evidence level |
|---|---|---|
| AO Foundation / AO Surgery Reference | Reconstructable radial head: fix; comminuted with longitudinal instability: replace, never excise in isolation; assess and stabilise the DRUJ | Expert consensus |
| ESSKA instructional review (Meglic et al., Int Orthop 2021) | Use an intraoperative radial pull test to detect IOM injury; treat the forearm as one functional unit; classification-guided algorithm | Level V review |
| JBJS Reviews narrative review (Sheth et al., 2022) | Restore radial length plus temporary DRUJ stabilisation acutely; approach acute radial head excision with caution; acute IOM repair indications unclear | Level V review |
| EFORT Open Reviews systematic review (Kooistra et al., 2022) | No accepted definition; radial head fracture with wrist/forearm pain should trigger comparative imaging and a dynamic stability test | Level III systematic review |
| BOA / AAOS dedicated guideline | No condition-specific guideline exists - this injury is too rare for a formal guideline | Not addressed |
Registry evidence
Joint and trauma registries (NJR, AJRR, AOANJRR, SHAR, Norwegian and NZJR) do not separately capture Essex-Lopresti injury or radial head arthroplasty for it, so there is no registry-level implant-survival or revision data to quote. Outcome evidence is therefore limited to single-centre case series and biomechanical studies, which is itself an examinable point about the quality of the evidence base.
Practice variation
- High-resource settings: ready access to modular radial head prostheses, intraoperative fluoroscopy and CT, and to bone-ligament-bone central band reconstruction for chronic cases.
- Limited-resource settings: where modern prostheses are unavailable, surgeons may have to choose between accepting the consequences of radial head loss and improvised stabilisation; this drives the global teaching point to preserve or replace, never simply excise, the radial head.
- Worldwide, the dominant cause of poor outcome is the same - a missed acute diagnosis leading to fixed proximal migration - so the universal priority is recognition, not a particular implant or technique.
Essex-Lopresti Injuries - Exam Quick Reference
Clinical summary