Orthopaedic Features of an Insensate Patient
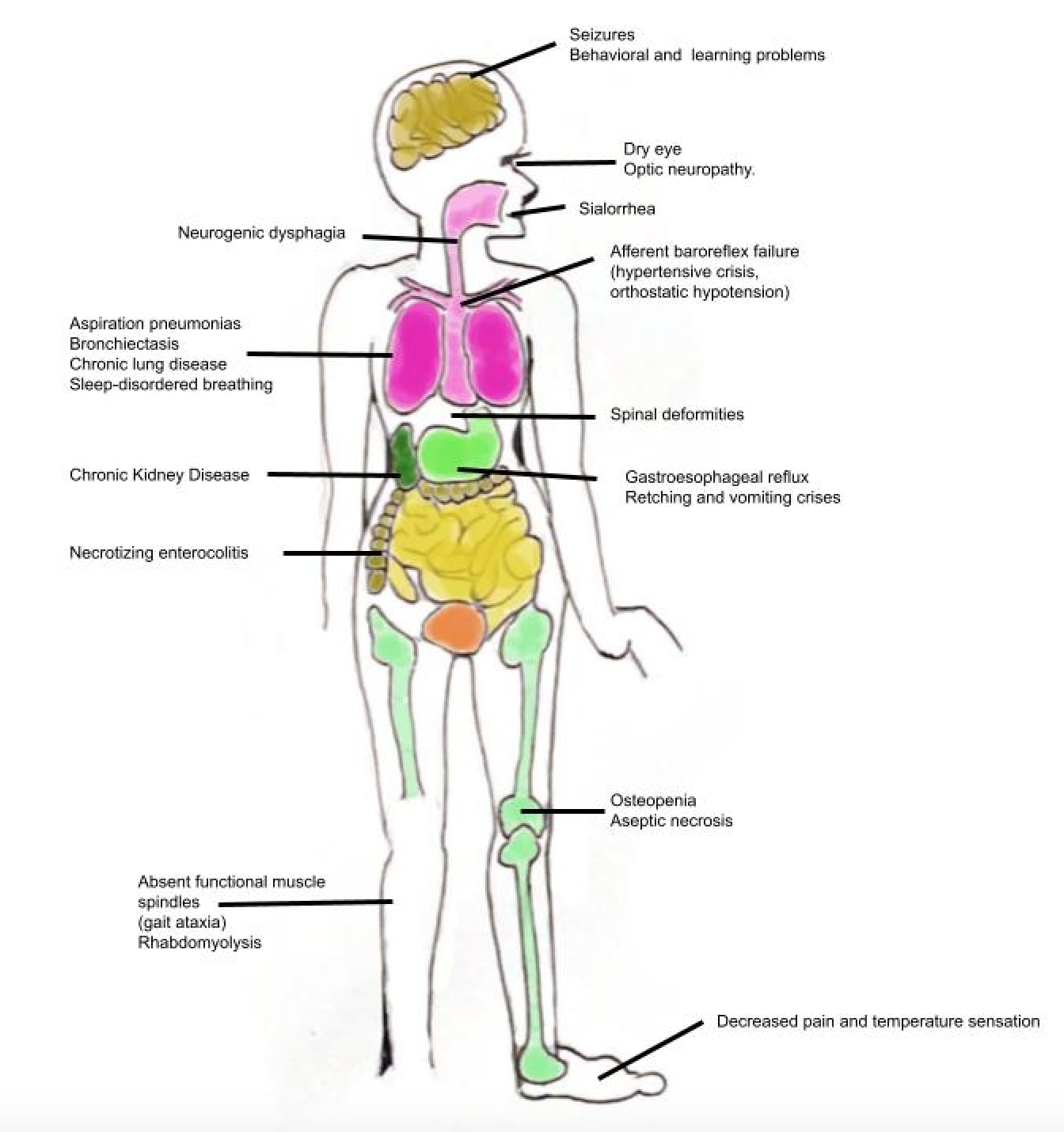
- FAMILIAL DYSAUTONOMIA (Riley-Day syndrome; hereditary sensory and autonomic neuropathy type III, HSAN III) is an AUTOSOMAL-RECESSIVE disorder occurring predominantly in Ashkenazi Jewish individuals (ELP1/IKBKAP gene), causing AUTONOMIC dysfunction (labile blood pressure/temperature, dysautonomic crises, absent overflow tears and fungiform tongue papillae, swallowing/aspiration problems) together with markedly REDUCED PAIN and TEMPERATURE sensation.
- The ORTHOPAEDIC consequences follow from the INSENSATE state: because the patient does not feel or normally avoid painful/damaging stimuli, injuries go UNRECOGNISED and untreated - the same mechanism that produces neuropathic orthopaedic problems across the congenitally insensate conditions (congenital insensitivity to pain, the HSANs, Lesch-Nyhan).
- The orthopaedic problems in congenitally insensate patients (including Riley-Day) comprise FRACTURE (often painless/unrecognised), SELF-MUTILATION, AUTO-AMPUTATION, OSTEOMYELITIS, SEPTIC ARTHRITIS, CHARCOT (neuropathic) JOINTS, SCOLIOSIS and DISLOCATION - a recognisable cluster driven by the abnormal pain response.
- PUT A NUMBER ON THE SPINE. About 90 PERCENT of surviving children with familial dysautonomia develop a spinal curvature, and it appears in the FIRST DECADE - so this is the expected course, not a complication to watch for. The curve is characteristically KYPHOTIC rather than lordotic: in an Israeli series of 51 patients seen at a scoliosis clinic, 37 had an increased thoracic kyphosis. CHARCOT (neuropathic) JOINTS and painless fractures result from repeated unperceived trauma to insensate joints and bones.
- MANAGEMENT is EARLY DIAGNOSIS and PATIENT/PARENT EDUCATION to PREVENT as many complications as possible (protective footwear/orthoses, joint protection, vigilance for unrecognised injury/infection); FRACTURES may be treated CONSERVATIVELY, while PROGRESSIVE SCOLIOSIS requires OPERATIVE intervention, and OSTEOMYELITIS, SEPTIC ARTHRITIS and CHARCOT joints require appropriate OPERATIVE treatment.
- PERIOPERATIVELY, the AUTONOMIC instability (blood-pressure/temperature lability, dysautonomic crises, aspiration risk) makes anaesthesia and surgery higher-risk, so any orthopaedic procedure is undertaken with careful multidisciplinary perioperative planning, and the orthopaedic surgeon must remember that the ABSENCE OF PAIN does not mean the absence of injury or infection.
- “Familial dysautonomia (Riley-Day, HSAN III) = autosomal recessive (Ashkenazi Jewish; ELP1/IKBKAP); autonomic dysfunction + reduced PAIN/TEMPERATURE sensation -> INSENSATE orthopaedic problems.
- “The insensate cluster (shared with CIPA/other HSANs): Charcot (neuropathic) joints, PAINLESS/unrecognised fractures, osteomyelitis/septic arthritis, self-mutilation/auto-amputation.
- “The spine is near-universal: ~90% of survivors develop a curve in the FIRST DECADE, characteristically KYPHOTIC. Bracing is minimally successful. Posterior fusion achieves only ~25% correction (friable osteoporotic bone), avoid anterior transthoracic approaches (pulmonary) - but pneumonia frequency fell and ataxia improved after surgery.
- “Management = early diagnosis + PROTECTION + patient/family EDUCATION to prevent complications; conservative fractures; OPERATE for progressive scoliosis, deep infection, Charcot instability. Beware autonomic instability perioperatively; absence of pain != absence of injury.
Reduced pain/temperature sensation means injuries go unrecognised -> Charcot joints, painless fractures, osteomyelitis/septic arthritis, self-injury, and progressive scoliosis.
Protect and educate - prevent complications (footwear/orthoses, joint protection, vigilance). Treat fractures conservatively; operate for progressive scoliosis/deep infection/Charcot instability.
The ELP1 Biology, Diagnosis, and Why Surgery Is High-Risk
- The gene and mechanism. ELP1 (formerly IKBKAP) on chromosome 9 encodes a scaffold subunit of the Elongator complex (transcriptional elongation and tRNA modification). A near-universal founder splice-site mutation (IVS20+6T to C) causes tissue-specific skipping of exon 20 with reduced ELP1 especially in the nervous system, so sensory and autonomic neurons fail to develop and survive. About 99.5% of FD alleles carry this founder mutation and the Ashkenazi carrier frequency is roughly 1 in 30, so carrier screening and prenatal diagnosis are available.
- The diagnostic hallmarks. Classically: Ashkenazi ancestry, alacrima (absent overflow tears), absent fungiform papillae (smooth tongue), absent/depressed deep-tendon reflexes, and no axon-flare after intradermal histamine; genetic testing (ELP1) is now confirmatory.
- The systemic picture that raises perioperative risk. Dysautonomic crises (cyclical vomiting, hypertension, tachycardia, sweating - treated with benzodiazepines/clonidine), orthostatic hypotension with supine hypertension (baroreflex failure), impaired thermoregulation, and oropharyngeal incoordination causing recurrent aspiration and restrictive lung disease - the last being especially important before scoliosis surgery.
Q: What is the molecular basis and diagnostic picture of FD, and why is surgery high-risk?
A: ELP1 (IKBKAP) encodes an Elongator-complex subunit; a founder splice-site mutation (IVS20+6T to C) skips exon 20, reducing ELP1 in the nervous system so sensory/autonomic neurons fail (~99.5% of FD alleles; Ashkenazi carrier ~1/30 → carrier/prenatal screening). Diagnostic hallmarks: alacrima, absent fungiform papillae (smooth tongue), absent deep-tendon reflexes, no histamine axon-flare (+ genetic confirmation). Surgery is high-risk because of dysautonomic crises, orthostatic hypotension with supine hypertension, impaired thermoregulation, and aspiration/restrictive lung disease.
The Insensate Orthopaedic Footprint & Its Management
Familial dysautonomia (Riley-Day, HSAN III) is an autosomal-recessive disorder (Ashkenazi Jewish; ELP1/ IKBKAP) of autonomic dysfunction and markedly reduced pain/temperature sensation. The orthopaedic problems follow from the insensate state - injuries go unrecognised - and form the recognisable cluster seen across the congenitally insensate conditions: Charcot (neuropathic) joints, painless/unrecognised fractures, scoliosis (common and progressive), osteomyelitis/septic arthritis, dislocations and self-mutilation/auto-amputation. Management is early diagnosis, protection and patient/family education to prevent complications; conservative fracture care where possible; and operative treatment for progressive scoliosis, deep infection and Charcot instability - all mindful that the autonomic instability makes anaesthesia/surgery higher-risk.
The unifying principle in the orthopaedic care of familial dysautonomia (and the insensate patient in general) is that the protective function of pain is lost, so the clinician's vigilance must replace it. Patients do not feel or normally avoid damaging stimuli, so fractures occur and go unrecognised, joints are repeatedly traumatised into Charcot (neuropathic) degeneration, ulcers and deep infections (osteomyelitis, septic arthritis) develop without the usual pain warning, and self-injury occurs - and scoliosis is common and progressive. The cornerstone of management is therefore prevention: early diagnosis, protective footwear and orthoses, joint protection, and education of the patient and family to watch for unrecognised injury and infection, because the absence of pain does not mean the absence of damage. Fractures can often be treated conservatively, but progressive scoliosis, deep infection and Charcot instability require operative treatment. Finally, the autonomic dysfunction - labile blood pressure and temperature, dysautonomic crises and aspiration risk - makes anaesthesia and surgery higher-risk, so any procedure needs careful multidisciplinary perioperative planning.
FD-Specific Orthopaedic Management: Scoliosis and the Insensate Limb
- Scoliosis in FD. About 90 percent of surviving children develop a curvature, appearing in the first decade and characteristically kyphotic rather than lordotic, so a kyphoscoliosis is the expected pattern. Bracing is poorly tolerated and was minimally successful at best in the published series - the insensate skin breaks down under a brace and the restrictive lung disease worsens with chest compression. Posterior spinal fusion is indicated for progression; it is high-risk because of the restrictive and aspiration lung disease, intraoperative autonomic lability and poor nutrition and wound-healing, and only about 25 percent correction should be expected because friable osteoporotic bone will not accept the corrective force. Anterior transthoracic approaches are avoided despite the kyphosis, because of pulmonary complications.
- The benefit, not just the risk. In that series, fusion was followed by a marked fall in the frequency of pneumonia and an improvement in ataxia, with a clear gain in quality of life - so the operation should not be discussed with a family as a dangerous attempt to straighten a spine. The gain is respiratory and functional, and the radiographic correction is modest by design.
- The insensate fracture and Charcot joint. Because the patient feels no pain, they continue to load the injured limb, risking delayed/malunion and progression to Charcot collapse - so immobilisation must be prolonged and enforced (the patient will not self-limit), and casts/orthoses must be well-moulded with vigilant skin checks (pressure sores form silently on insensate skin). The surgical goal in a neuropathic joint is a stable, plantigrade, braceable limb (realignment/arthrodesis) rather than anatomical perfection, always excluding painless superimposed infection.
Both halves of the problem belong to larger families. The spinal deformity is managed on the principles of neuromuscular scoliosis, and because the curve appears in the first decade it also falls under early-onset scoliosis. The insensate joint is the same process described in Charcot neuroarthropathy, and the other hereditary neuropathy that reaches an orthopaedic clinic with a deformed foot is Charcot-Marie-Tooth disease.
Q: How does the insensate state change scoliosis and fracture/Charcot management in FD?
A: A curve develops in about 90 percent of survivors, in the first decade, and is characteristically kyphotic; bracing is minimally successful (insensate-skin breakdown + restrictive lung disease). Posterior spinal fusion is high-risk (aspiration/restrictive lung disease, autonomic lability, wound/nutrition), gives only about 25 percent correction because the bone is friable and osteoporotic, and anterior transthoracic approaches are avoided - yet pneumonia frequency fell and ataxia improved after fusion, so the benefit is respiratory and functional rather than radiographic. For fractures/Charcot: because there is no pain the patient keeps loading the limb → delayed/malunion/Charcot collapse, so immobilisation must be prolonged and enforced, casts vigilantly skin-checked (silent pressure sores), and the surgical goal is a stable, plantigrade, braceable limb - always excluding painless infection.
What the Spine Series Actually Showed
Spinal deformity in familial dysautonomia is the rule rather than a complication: about 90 percent of surviving children develop a curvature, appearing in the first decade of life, and it is characteristically kyphotic rather than lordotic. In an Israeli series, 51 of the 90 reported national cases attended a scoliosis clinic and 37 had an increased thoracic kyphosis alongside the scoliosis. Orthotic treatment and physiotherapy were minimally successful at best - which is worth stating plainly, because in an insensate child a brace is also the thing that ulcerates skin silently and compresses an already restrictive chest. The practical consequence is that a child with this diagnosis should be under spinal surveillance from early childhood rather than referred when a curve is noticed.
Thirteen of those 51 patients underwent posterior spinal fusion, the indication being curve progression. Only about 25 percent correction was obtained in the majority, partly because friable, osteoporotic bone would not tolerate the corrective force. Anterior transthoracic procedures were avoided despite the kyphosis, because of the frequency of pulmonary complications, and bank bone alone was used to spare the patient the trauma of graft harvest. Complications exceeded those of ordinary paediatric deformity surgery.
After fusion the series reported a marked decrease in the frequency of pneumonia and an improvement in ataxia - the latter for reasons the authors could not explain - with an obvious gain in quality of life. So the operation should not be presented to a family purely as a high-risk correction of a deformity: modest radiographic correction coexisted with a real respiratory and functional benefit, which is the honest way to frame the consent conversation.
Mnemonics & Memory Aids
INSENSATE
Hook:INSENSATE: Insensate (Riley-Day), Neuropathic joints, Scoliosis, Educate/Early dx, No pain != no injury, Self-injury/Septic, Autonomic risk, Treat (conservative #/operate scoliosis).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child with familial dysautonomia presents with a swollen, deformed but painless ankle and a previously unrecognised fracture. How do you think about and manage this?”
What it is
- Familial dysautonomia (Riley-Day, HSAN III); autosomal recessive
- Predominantly Ashkenazi Jewish; ELP1/IKBKAP gene
- Autonomic dysfunction + reduced pain/temperature sensation
Orthopaedic cluster (insensate)
- Charcot (neuropathic) joints; painless/unrecognised fractures
- Spinal curvature in ~90 percent, first decade, kyphotic; bracing minimally successful
- Fusion: ~25 percent correction (friable bone), avoid anterior transthoracic - but pneumonia fell and ataxia improved
- Osteomyelitis/septic arthritis; dislocation; self-mutilation/auto-amputation
Management
- Early diagnosis + protection (footwear/orthoses/joint protection) + patient/family education
- Conservative fracture care where possible
- Operate for progressive scoliosis, deep infection, Charcot instability; beware autonomic instability perioperatively
Evidence & Key Studies
Orthopaedic manifestations in congenitally insensate patients (incl. Riley-Day syndrome)
- In congenitally insensate patients (including congenital insensitivity to pain, Riley-Day syndrome and Lesch-Nyhan syndrome), an abnormality of pain interpretation/avoidance leads to self-inflicted damage.
- The orthopaedic problems and complications included fracture, self-mutilation, auto-amputation, osteomyelitis, septic arthritis, Charcot joints, scoliosis and dislocation.
- Effective management consists of early diagnosis and patient/parent education to prevent complications; fractures may be treated conservatively, progressive scoliosis requires operative intervention, and osteomyelitis, septic arthritis and Charcot joints require appropriate operative treatment.
Aspects of spinal deformity in familial dysautonomia (Riley-Day syndrome)
- About 90 percent of surviving children with familial dysautonomia develop a spinal curvature, appearing in the first decade and usually kyphotic rather than lordotic. Of the 90 cases reported in Israel, 51 attended the scoliosis clinic; 37 had an increased thoracic kyphosis in addition to the scoliosis. Orthotic treatment and physiotherapy were minimally successful at best.
- Thirteen of the 51 underwent surgery, the indication being curve progression, with six years of follow-up. Only posterior fusions were performed - anterior transthoracic procedures were avoided despite the kyphosis because of the frequency of pulmonary complications - and bank bone alone was used to avoid the additional trauma of graft harvest.
- Only about 25 percent correction was achieved in the majority, partly because friable osteoporotic bone limited the corrective force that could be applied, and the complication rate exceeded that of ordinary paediatric deformity surgery. After surgery there was a marked decrease in the frequency of pneumonia and an improvement in ataxia, for reasons the authors could not explain. This is a small retrospective single-country series from the era of Harrington and sublaminar-wire instrumentation, so the technical findings do not transfer directly to modern pedicle-screw constructs.
The cluster of orthopaedic problems in congenitally insensate patients including Riley-Day syndrome (fracture, self-mutilation, auto-amputation, osteomyelitis, septic arthritis, Charcot joints, scoliosis, dislocation) and the management principles (early diagnosis and patient/parent education to prevent complications; conservative fracture treatment; operative treatment for progressive scoliosis and for osteomyelitis/septic arthritis/Charcot joints) come from the cited Guidera study. The nature of familial dysautonomia (HSAN III, autosomal recessive, Ashkenazi Jewish, ELP1/IKBKAP, autonomic dysfunction with reduced pain/temperature sensation) and the perioperative autonomic-instability risk are standard, well-established teaching. The spinal figures - the 90 percent curvature rate, the kyphotic pattern, the poor response to bracing, the roughly 25 percent correction achieved and the post-operative reduction in pneumonia - come from the Kaplan series, which is small, retrospective, and from the era of Harrington and sublaminar-wire instrumentation, so its technical findings should not be read across to modern constructs. No trial compares any treatment strategy in this disease, no curve threshold for surgery has been validated, and no screening interval for the spine or for neuropathic joints has been established, so none is quoted here.