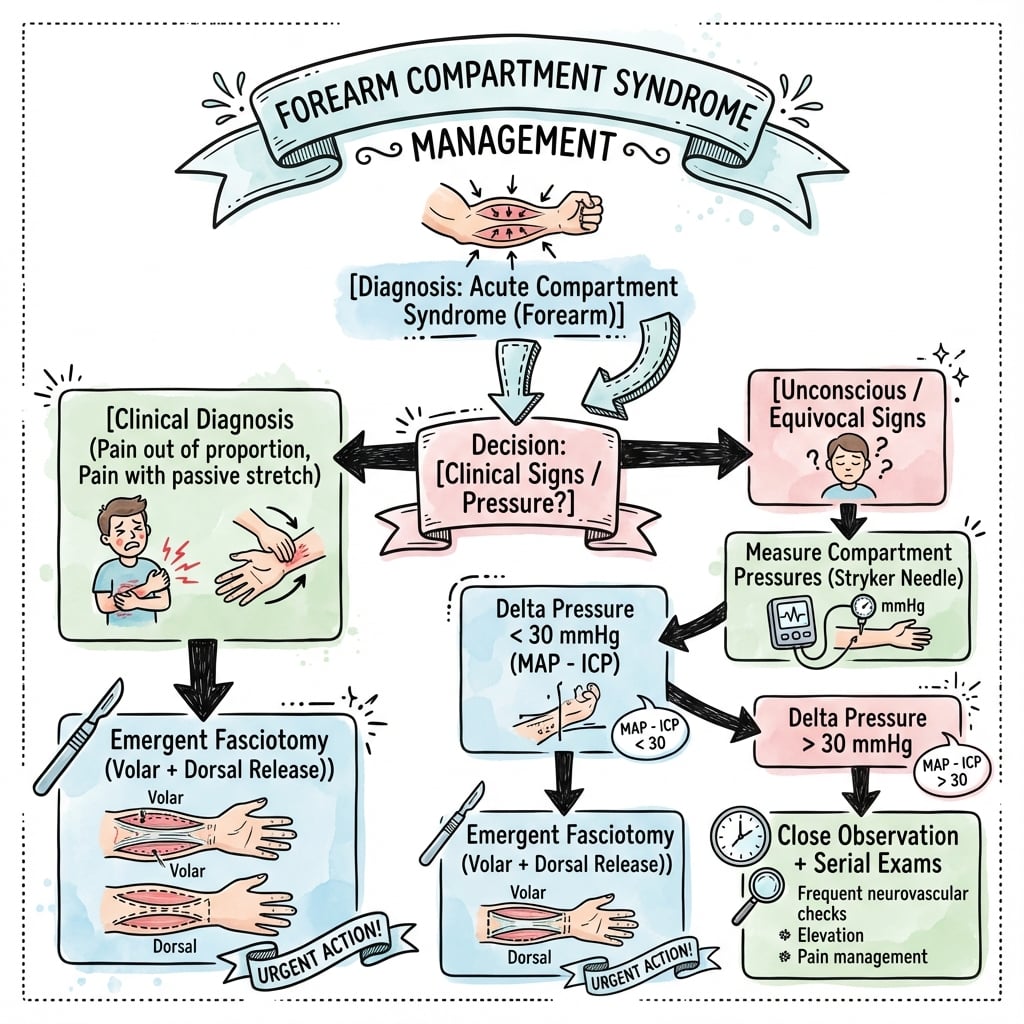
Pain Out of Proportion | Pressure Monitoring | Urgent Fasciotomy
- Pain on passive stretch is earliest reliable sign - pain with passive finger extension
- 5 Ps are LATE findings - Pulselessness and pallor indicate damage already occurring
- Pressure threshold: greater than 30mmHg absolute OR ΔP less than 30mmHg from diastolic
- Volar fasciotomy MUST include carpal tunnel release - edema extends distally
- Volkmann's ischemic contracture is the devastating end result of missed diagnosis
- “Clinical diagnosis sufficient - do NOT delay surgery for pressure measurement if high suspicion
- “Always release BOTH volar AND dorsal compartments if any doubt
- “Leave wounds completely open - never close primarily, DPC at 48-72 hours
- “High-risk fractures: supracondylar (children), both-bone forearm, floating elbow
EARLIEST and MOST RELIABLE sign. Pain with passive finger extension (volar) or flexion (dorsal) indicates rising compartment pressures. Do NOT wait for other signs.
Pain, Pressure, Pallor, Pulselessness, Paresthesia. Pallor and pulselessness are LATE signs - fasciotomy is needed BEFORE these appear or damage is irreversible.
Absolute greater than 30mmHg OR ΔP less than 30mmHg (diastolic BP minus compartment pressure = perfusion pressure). Either indicates need for urgent fasciotomy.
Volar fasciotomy MUST include carpal tunnel decompression - swelling extends distally. Add dorsal release if pressures elevated or any clinical doubt whatsoever.
Overview
Forearm compartment syndrome is a surgical emergency characterized by elevated pressure within the closed fascial compartments of the forearm, leading to compromised tissue perfusion and progressive ischemic injury to muscles and nerves.
- Forearm contains 3-4 distinct osteofascial compartments with limited compliance
- Elevated compartment pressure reduces capillary perfusion (normal compartment pressure: 0-8 mmHg)
- Muscle necrosis begins at 30 minutes of complete ischemia; irreversible after 6-8 hours
- Volkmann's ischemic contracture is the devastating sequela of missed or delayed diagnosis
- High medicolegal risk - one of the most common causes of orthopaedic litigation
Compartment syndrome occurs when pressure within a closed osteofascial space rises sufficiently to compromise tissue perfusion, leading to:
- Muscle ischemia progressing to necrosis
- Nerve ischemia causing sensory then motor deficits
- If untreated: Volkmann's ischemic contracture
Arteriovenous (AV) gradient theory: Tissue perfusion depends on the pressure gradient between arterioles and venules. When compartment pressure rises, venous outflow is first compromised, increasing venous pressure and reducing the AV gradient. This leads to decreased capillary perfusion even when arterial inflow remains present (pulse is preserved until late).
Etiology and Risk Factors
Common Causes
- Examples
- Both-bone forearm, supracondylar, distal radius
- Mechanism
- Bleeding, soft tissue injury
- Risk Level
- HIGH
- Examples
- Motor vehicle, industrial accidents
- Mechanism
- Direct muscle damage, edema
- Risk Level
- HIGH
- Examples
- Tight casts, circumferential dressings
- Mechanism
- External compression
- Risk Level
- HIGH
- Examples
- Arterial injury with revascularization
- Mechanism
- Reperfusion injury
- Risk Level
- HIGH
- Examples
- Anticoagulation, hemophilia
- Mechanism
- Compartment hemorrhage
- Risk Level
- MODERATE
- Examples
- Circumferential full-thickness
- Mechanism
- Eschar constriction + edema
- Risk Level
- MODERATE
- Examples
- IV infiltration, drug injection
- Mechanism
- Fluid accumulation
- Risk Level
- MODERATE
- Examples
- Necrotizing fasciitis
- Mechanism
- Edema, tissue destruction
- Risk Level
- MODERATE
High-Risk Fracture Patterns
- Supracondylar fractures in children - highest risk, especially displaced type III
- Both-bone forearm fractures - significant soft tissue injury
- Floating elbow - combined supracondylar + forearm fracture
- Monteggia and Galeazzi fractures - high-energy injury pattern
- Distal radius fractures with severe swelling/displacement
Patient Risk Factors
- Male gender (2:1)
- Age less than 35 years
- Anticoagulation
- Coagulopathy
- High-energy trauma
- Diabetes mellitus
- Peripheral vascular disease
- Drug/alcohol intoxication
- Unable to communicate
- Circumferential casts
- Tight bandages
- Positioning in surgery
- Infiltrated IV lines
- Prolonged surgery
Anatomy and Pathophysiology
Forearm Compartments
The forearm contains three to four distinct compartments depending on classification. Understanding anatomy is critical for complete fasciotomy.
- Pronator teres (PT)
- Flexor carpi radialis (FCR)
- Palmaris longus (PL)
- Flexor digitorum superficialis (FDS)
- Flexor carpi ulnaris (FCU)
Median nerve, Ulnar nerve
Most commonly affected in compartment syndrome
- Flexor digitorum profundus (FDP)
- Flexor pollicis longus (FPL)
- Pronator quadratus (PQ)
Anterior interosseous nerve (AIN) - motor branch of median
Contains AIN - FPL/FDP index weakness is early sign
- Extensor digitorum communis (EDC)
- Extensor digiti minimi (EDM)
- Extensor indicis proprius (EIP)
- Extensor carpi ulnaris (ECU)
- Abductor pollicis longus (APL)
- Extensor pollicis brevis (EPB)
- Extensor pollicis longus (EPL)
- Supinator
Posterior interosseous nerve (PIN)
Less commonly affected but must check pressures
- Brachioradialis (BR)
- Extensor carpi radialis longus (ECRL)
- Extensor carpi radialis brevis (ECRB)
Some consider part of dorsal compartment; released with dorsal approach
Pathophysiology
Ischemia-Reperfusion Cascade:
- Increased compartment pressure (from bleeding, edema, external compression)
- Venous outflow obstruction - first to be affected
- Decreased arteriovenous gradient - reduced capillary perfusion
- Tissue ischemia - muscle more sensitive than nerve initially
- Cellular swelling - further increases pressure (positive feedback)
- Muscle necrosis - begins within 30 minutes of complete ischemia
- Nerve damage - reversible initially, irreversible after 6-8 hours
- Volkmann's contracture - fibrotic replacement of necrotic muscle
Critical Time Windows
- Tissue Effects
- Muscle injury begins
- Tissue Effects
- Reversible muscle injury
- Tissue Effects
- Nerve dysfunction (initially reversible)
- Tissue Effects
- Irreversible muscle necrosis begins
- Tissue Effects
- Permanent nerve damage, Volkmann's contracture
Fasciotomy performed within 6 hours of symptom onset has significantly better outcomes than delayed decompression. After 8 hours, irreversible damage is highly likely.
Classification Systems
Matsen Classification (By Clinical Stage):
- Clinical Findings
- Pain on passive stretch, no neurologic deficit
- Compartment Pressure
- Elevated (20-30 mmHg)
- Tissue Status
- Reversible ischemia
- Urgency
- High suspicion, serial monitoring
- Clinical Findings
- Pain, paresthesia, tense compartment
- Compartment Pressure
- Significantly elevated (greater than 30 mmHg or ΔP less than 30)
- Tissue Status
- Progressive muscle ischemia
- Urgency
- URGENT fasciotomy indicated
- Clinical Findings
- Pallor, paralysis, pulselessness
- Compartment Pressure
- Critically elevated (greater than 40 mmHg)
- Tissue Status
- Irreversible damage occurring
- Urgency
- EMERGENCY fasciotomy
- Clinical Findings
- Fixed contracture, tissue necrosis
- Compartment Pressure
- Variable (may normalize)
- Tissue Status
- Irreversible damage done
- Urgency
- Delayed reconstruction
The Matsen classification helps guide urgency of intervention based on clinical and pressure findings.
Clinical Presentation
Clinical Features by Stage
- Time Frame
- 0-2 hours
- Clinical Findings
- Pain out of proportion, pain on passive stretch
- Action Required
- HIGH SUSPICION - consider fasciotomy
- Time Frame
- 2-4 hours
- Clinical Findings
- Tense compartment, increasing analgesia needs, paresthesia
- Action Required
- URGENT fasciotomy
- Time Frame
- 4-8 hours
- Clinical Findings
- Pallor, paralysis, weak/absent pulses
- Action Required
- EMERGENCY fasciotomy - damage likely
- Time Frame
- More than 8 hours
- Clinical Findings
- Pulselessness, complete sensorimotor loss, cold limb
- Action Required
- Fasciotomy +/- amputation consideration
Key Clinical Signs
Pain on Passive Stretch - THE most reliable early sign:
- Volar compartment: Pain with passive finger EXTENSION
- Dorsal compartment: Pain with passive finger FLEXION
- Pain is disproportionate to the injury itself
- Increasing analgesic requirements despite adequate initial dosing
- First web space numbness (AIN - median nerve)
- Ulnar nerve distribution numbness (less common)
- PIN (posterior interosseous nerve) - motor only, no sensory
- AIN palsy: Weak FPL (thumb IP), FDP to index finger
- Weak finger flexion (FDS, FDP)
- Weak wrist flexion
A palpable pulse does NOT rule out compartment syndrome. Compartment syndrome affects the microcirculation while arterial inflow may be preserved until late. Waiting for pulse loss means irreversible damage has already occurred.
The topic stresses that the supracondylar fracture is the commonest cause in children and that "pain out of proportion" is the key adult sign - but a frightened, pre-verbal or distressed child cannot reliably report disproportionate pain or cooperate with passive-stretch testing. The paediatric-specific triad is the 3 A's:
- Analgesia - an increasing/escalating analgesic requirement (the child needs more and more opioid for a fracture that should be settling) is the most important and earliest objective red flag.
- Anxiety - rising distress and agitation in a child who was previously settling.
- Agitation - inconsolability and restlessness disproportionate to the injury.
The teaching is that in children you watch the trend in analgesia demand and behaviour, not a verbal pain-out-of-proportion report. An escalating opioid requirement after a supracondylar or both-bone forearm fracture is a compartment syndrome until proven otherwise, and the same low threshold for fasciotomy applies - children tolerate ischaemia no better than adults.
Exam point: in a child, the classic adult signs are unreliable - use the 3 A's (increasing Analgesia requirement, Anxiety, Agitation), with a rising analgesic demand after a high-risk fracture being the decisive trigger to act.
Investigations
Compartment Pressure Measurement
- Equivocal clinical examination
- Obtunded/uncooperative patient
- Unreliable examination (intoxication, head injury)
- Serial monitoring when clinical suspicion moderate
- Use calibrated device (Stryker STIC, arterial line transducer)
- Measure in zone of maximum injury/swelling
- Measure all compartments if any suspicion
- Position limb at level of heart
- Infiltrate 0.3ml saline to confirm placement
Pressure Thresholds for Fasciotomy
PRESSURE THRESHOLDS
ΔP (Delta P) = Diastolic BP - Compartment Pressure
This represents the perfusion pressure gradient. When ΔP is less than 30 mmHg, tissue perfusion is inadequate regardless of absolute compartment pressure.
Example: Patient with DBP 70 mmHg and compartment pressure 45 mmHg:
- ΔP = 70 - 45 = 25 mmHg (LESS THAN 30 = fasciotomy indicated)
Other Investigations
- CK (creatine kinase) - elevated with muscle necrosis
- Myoglobin - rhabdomyolysis marker
- Serum lactate - tissue ischemia
- Renal function - monitor for myoglobinuric AKI
- Coagulation studies - if bleeding diathesis suspected
- X-rays - identify underlying fracture, guide fracture management
- CT/MRI - NOT routine, may delay treatment
- Doppler ultrasound - assess arterial flow (pulse presence ≠ adequate perfusion)
Clinical diagnosis is sufficient. Do not delay fasciotomy for pressure measurement, imaging, or laboratory results if clinical suspicion is high. Time to fasciotomy is the critical factor.
Continuous Monitoring
Indications for continuous compartment pressure monitoring:
- Multiple trauma patient requiring sedation/ventilation
- Post-operative monitoring after high-risk surgery
- Burns with circumferential involvement
- Serial measurements impractical
The differential rightly flags compartment syndrome "masked by a nerve block", but this is a live controversy worth holding clearly, because the whole diagnosis rests on pain:
- The concern: a dense regional/peripheral nerve block, epidural, or opioid PCA abolishes the cardinal sign (pain out of proportion / pain on passive stretch) and can delay recognition of an evolving compartment syndrome in a high-risk limb.
- The modern, nuanced view: there is no high-level evidence that a block causes compartment syndrome or that it must always be withheld, and good analgesia is humane - but breakthrough pain "through" a working block, or escalating analgesic demand, is a major RED FLAG for compartment syndrome and must trigger urgent assessment, not a top-up.
- Practical rules: in a high-risk limb (both-bone forearm, supracondylar, crush, vascular repair) prefer shorter-acting, lower-concentration, single-shot or motor-sparing analgesia over a dense long-acting/continuous block, ensure the team knows the limb is at risk, and monitor the other signs and the analgesic trend (and compartment pressures if obtunded). Never let "the block is working" reassure you out of a diagnosis.
Exam point: regional blocks/PCA can mask compartment syndrome by removing the pain signal - do not necessarily withhold analgesia, but in a high-risk limb avoid dense long-acting blocks, treat breakthrough pain or rising analgesia demand as a red flag, and rely on serial signs/pressures rather than the absence of pain.

Management Algorithm
Initial Actions:
- Bivalve ALL casts
- Release ALL circumferential dressings
- Cut down to skin
- Position limb at heart level
- Do NOT elevate (reduces arterial perfusion)
- Maintain blood pressure (avoid hypotension)
- Correct hypovolemia
- Supplemental oxygen
- Maintain normothermia
- Correct coagulopathy
- Contact theatre immediately
- Consent for fasciotomy
- Plan for both volar AND dorsal release
- Warn patient wounds will be left open
- Plan for return to theatre 48-72h
Immediate removal of all constrictive elements is critical before definitive fasciotomy.
Surgical Technique
Preoperative Preparation
- Supine position, arm on radiolucent hand table
- Tourniquet applied but use judiciously (inflate only if bleeding obscures view)
- Consider avoiding tourniquet to assess tissue perfusion
- Explain wounds will be left open
- Risk of incomplete decompression
- Nerve and vessel injury risk
- Need for return to theatre at 48-72 hours
- Skin graft may be required
- Risk of ongoing muscle/nerve damage despite surgery
Volar Fasciotomy Technique
- Curvilinear/zigzag incision from medial epicondyle to palm
- Cross antecubital fossa obliquely (avoid linear scar contracture across flexion crease)
- Curve ulnar at wrist, then extend into palm for carpal tunnel release
- Total length: 15-20cm forearm + 3-4cm palm extension
- Skin Incision - Full-thickness skin incision, generous length
- Identify and protect superficial veins - ligate if necessary
- Release lacertus fibrosus (bicipital aponeurosis) at antecubital fossa
- Identify median nerve - runs between FDS and FDP
- Release superficial volar compartment:
- Incise fascia overlying PT, FCR, PL, FCU, FDS
- Full-length fascial release
- Palpate muscles - should decompress and bulge through fasciotomy
- Release deep volar compartment:
- Retract FDS muscles
- Incise deep fascia overlying FDP, FPL, PQ
- Protect AIN (runs on interosseous membrane)
- Carpal tunnel release (MANDATORY):
- Extend incision into palm
- Divide transverse carpal ligament under direct vision
- Protect median nerve and palmar cutaneous branch
- Inspect all muscles:
- Viable muscle: pink, contracts with stimulation, bleeds when cut
- Non-viable muscle: dark, does not contract, does not bleed
- Debride clearly necrotic tissue
A systematic approach to volar fasciotomy ensures complete decompression and protection of critical structures.
Volar Fasciotomy MUST Include:
- Superficial compartment release (complete)
- Deep compartment release (complete)
- Carpal tunnel decompression (ALWAYS)
- Protection of median nerve throughout
- Assessment of muscle viability
Complications
Complications of Delayed/Missed Diagnosis
- Description
- Irreversible flexor muscle fibrosis and shortening
- Timing
- Weeks-months
- Treatment
- Tendon lengthening, muscle slide, free flap
- Description
- Median and/or ulnar nerve damage
- Timing
- Immediate
- Treatment
- Nerve exploration, possible grafting
- Description
- Dead muscle requiring debridement
- Timing
- Days
- Treatment
- Serial debridement, coverage
- Description
- Myoglobin release causing AKI
- Timing
- Hours-days
- Treatment
- Aggressive hydration, ?dialysis
- Description
- Neuropathic and ischemic pain
- Timing
- Months
- Treatment
- Multidisciplinary management
- Description
- Loss of grip strength, dexterity
- Timing
- Permanent
- Treatment
- Reconstructive surgery, therapy
Volkmann's Ischemic Contracture
Irreversible fibrotic contracture of forearm flexor muscles following untreated compartment syndrome.
- Wrist flexion
- MCP hyperextension
- IP joint flexion
- Thumb adduction
Passive wrist extension causes fingers to flex further (muscle shortening)
Classification (Tsuge):
- Muscle Involvement
- FDP to 2-3 fingers, FPL
- Features
- Limited contracture
- Treatment
- Muscle slide, tendon lengthening
- Muscle Involvement
- All flexors involved
- Features
- Significant deformity
- Treatment
- Muscle slide + tendon transfer
- Muscle Involvement
- Both flexors AND extensors
- Features
- Severe dysfunction
- Treatment
- Free functioning muscle transfer
Complications of Fasciotomy
- Wound infection
- Bleeding
- Nerve injury (iatrogenic)
- Vessel injury
- Skin edge necrosis
- Incomplete release
- Unsightly scars
- Skin graft contracture
- Chronic wound healing
- Tethering of tendons
- Altered sensation
- Need for secondary reconstruction
Postoperative Care and Rehabilitation
Immediate Post-operative Management
- Leave wounds completely OPEN - NEVER close primarily
- Apply loose non-adherent dressing (Jelonet, Adaptic)
- Consider negative pressure wound therapy (VAC) if:
- Significant edema persists
- Large wound with exposed structures
- Difficult to maintain dressing
- Position of function to prevent contracture:
- Wrist: 20-30° extension
- MCP joints: 70-90° flexion
- IP joints: Full extension
- Thumb: Abduction and opposition
- Avoid tight circumferential dressings
- Ensure splint does not compress compartments
- Neurovascular observations every 2 hours for first 24 hours
- Monitor for:
- Persistent pain (inadequate decompression)
- Worsening motor/sensory deficit
- Signs of bleeding
- Systemic complications (rhabdomyolysis)
Laboratory Monitoring
- CK (creatine kinase) - daily initially
- Myoglobin - serum and urine
- Renal function - creatinine, eGFR
- Urine output - maintain greater than 1ml/kg/h
- Lactate - marker of tissue ischemia
- Aggressive IV hydration - aim UOP greater than 1ml/kg/h
- Alkalinize urine - IV sodium bicarbonate
- Monitor potassium - hyperkalemia risk
- Consider dialysis if AKI develops
- Treat underlying cause
Return to Theatre (48-72 Hours)
- Muscle remains viable (pink, contractile)
- Edema has resolved
- No signs of infection
- Skin edges can be approximated without tension
- Thorough wound irrigation
- Reassess muscle viability - debride any necrotic tissue
- Approximate skin edges with interrupted sutures or staples
- Avoid tension on closure
- May need staged closure if significant gap
Delayed primary closure is ideal when edema resolves and skin edges can be approximated without tension.
Rehabilitation Protocol
- Wound healing priority
- Gentle passive ROM when wounds closed/stable
- Edema control - elevation, compression
- Hand therapy referral
- Active ROM exercises
- Scar massage and desensitization
- Gentle strengthening
- Functional activities
- Progressive strengthening
- Return to activities of daily living
- Monitor for contracture development
- Long-term follow-up
Monitor for signs of developing Volkmann's contracture:
- Progressive finger flexion posture
- Cascade sign (wrist extension worsens finger flexion)
- Grip weakness
- Prompt referral to hand surgery if contracture develops
Outcomes and Prognosis
Factors Affecting Outcome
Timing of Fasciotomy:
- Expected Outcome
- Excellent - minimal muscle/nerve damage
- Functional Recovery
- 68% near-normal function
- Expected Outcome
- Good - some muscle fibrosis, nerve recovery
- Functional Recovery
- 40% near-normal function
- Expected Outcome
- Fair - significant muscle damage, incomplete nerve recovery
- Functional Recovery
- 20% near-normal function
- Expected Outcome
- Poor - established damage, Volkmann's likely
- Functional Recovery
- 8% near-normal function
Other Prognostic Factors:
- Severity of initial injury
- Associated fractures and soft tissue trauma
- Patient age (younger = better recovery potential)
- Rehabilitation compliance
- Presence of complications (infection, rhabdomyolysis)
Expected Recovery Timeline
Timeline:
- First sensation: 2-4 weeks
- Protective sensation: 6-12 weeks
- Discriminative touch: 3-6 months
- May remain incomplete in severe cases
Timeline:
- Muscle contraction: 4-8 weeks
- Functional strength: 3-6 months
- Maximal recovery: 12-18 months
- Depends on extent of muscle necrosis
Timeline:
- ADL independence: 3-6 months
- Return to work: 6-12 months
- Full recovery: 12-24 months
- May have persistent weakness
Volkmann's Contracture Outcomes
Prevention is Key:
- Incidence with early fasciotomy (less than 6h): less than 5%
- Incidence with delayed fasciotomy (greater than 12h): 20-40%
- Established contracture is IRREVERSIBLE - reconstructive surgery only
Reconstructive Surgery Outcomes:
- Surgery
- Muscle slide, tendon lengthening
- Expected Function
- Good - 70-80% normal
- Patient Satisfaction
- High
- Surgery
- Muscle slide + tendon transfers
- Expected Function
- Fair - 40-60% normal
- Patient Satisfaction
- Moderate
- Surgery
- Free functioning muscle transfer
- Expected Function
- Poor - 20-30% normal
- Patient Satisfaction
- Low to moderate
Long-term Complications Rates
- Incidence
- 10-20%
- Impact
- Cosmetic, possible functional limitation
- Management
- Scar revision, Z-plasty
- Incidence
- 15-25%
- Impact
- Neuropathic pain, impaired function
- Management
- Multidisciplinary pain management
- Incidence
- 30-50%
- Impact
- Reduced grip strength, endurance
- Management
- Ongoing therapy, adaptive strategies
- Incidence
- 20-35%
- Impact
- Protective sensation usually preserved
- Management
- Desensitization therapy
- Incidence
- 5-10% (early surgery), 20-40% (late surgery)
- Impact
- Severe functional impairment
- Management
- Reconstructive surgery
- Incidence
- 5-15%
- Impact
- Delayed healing, possible amputation
- Management
- Antibiotics, serial debridement
Medicolegal Outcomes
Missed or delayed compartment syndrome is one of the most common and costly sources of orthopaedic litigation internationally:
- Common allegations: delayed diagnosis, failure to monitor or document neurovascular status, and inadequate (incomplete) fasciotomy
- Claims are frequent and high-value in multiple jurisdictions (e.g. analyses of UK NHS Resolution and US closed-claims data), driven by the catastrophic, irreversible nature of the sequelae
- Prevention: meticulous time-stamped documentation, a low threshold for fasciotomy, and early senior/specialist involvement
Key Documentation for Medicolegal Protection:
- Time-stamped neurovascular examinations
- Compartment pressure measurements (if performed)
- Clinical decision-making rationale
- Patient/family discussions about risks
- Informed consent including Volkmann's contracture risk
- Time from symptom onset to surgical decompression
Guidelines, Registries & Global Practice
Differential Diagnosis
Compartment syndrome must be distinguished from other causes of a painful, swollen or neurologically compromised forearm. The two most dangerous mimics to exclude are arterial injury and an evolving compartment syndrome masked by a nerve block.
- Distinguishing Features
- Pain out of proportion, pain on passive stretch, tense compartment, escalating analgesia
- Key Test
- Clinical; compartment pressure / ΔP if equivocal
- Pitfall
- Pulse often preserved until late - do not wait for it
- Distinguishing Features
- Cold pale limb, absent pulse, hard signs of vascular injury, ABI reduced
- Key Test
- Doppler, CT angiography
- Pitfall
- Can coexist with compartment syndrome (e.g. supracondylar fracture)
- Distinguishing Features
- Focal sensorimotor deficit in single nerve territory, soft compartment, no disproportionate pain
- Key Test
- Clinical exam, nerve conduction (delayed)
- Pitfall
- Mislabelling early compartment ischaemia as primary nerve injury
- Distinguishing Features
- Erythema, warmth, fever, raised inflammatory markers, soft compartment
- Key Test
- Bloods (WCC, CRP), clinical
- Pitfall
- Necrotising fasciitis can mimic and coexist - look for crepitus, systemic toxicity
- Distinguishing Features
- Swelling, less severe pain, no pain on passive stretch
- Key Test
- Duplex ultrasound
- Pitfall
- Rare in upper limb; do not anticoagulate if compartment syndrome possible
- Distinguishing Features
- Pain proportionate to injury, settles with analgesia and splintage
- Key Test
- Clinical response to analgesia
- Pitfall
- Attributing escalating pain to 'just the fracture'
Global Epidemiology
According to PubMed, the largest population series (McQueen et al, J Bone Joint Surg Br 2000, PMID 10755426) of 164 consecutive acute compartment syndromes found an associated fracture in 69%, with forearm cases linked to distal radius fractures and occurring predominantly in young men under 35 years. The Lancet Emergency Surgery Series review (von Keudell et al 2015, PMID 26460664) confirms acute compartment syndrome affects upper and lower limbs in both adults and children and that there remains no internationally agreed diagnostic gold standard. Forearm compartment syndrome in children is most often associated with displaced supracondylar humeral fractures (Mubarak & Carroll, PMID 479251).
Guideline & Registry Comparison
- Region
- UK
- Key Position
- Urgent senior decompression; clinical diagnosis paramount; document neurovascular status serially
- Evidence Level
- Consensus standard
- Region
- International
- Key Position
- Clinical suspicion drives early fasciotomy; continuous pressure monitoring for obtunded/unreliable patients
- Evidence Level
- Narrative review (Level V)
- Region
- USA
- Key Position
- Either absolute pressure greater than 30 mmHg OR ΔP less than 30 mmHg; fasciotomy if clinically suspected
- Evidence Level
- Expert consensus
- Region
- International
- Key Position
- Complete volar + dorsal release with mandatory carpal tunnel decompression; wounds left open
- Evidence Level
- Technique consensus
- Region
- Europe
- Key Position
- ΔP threshold (McQueen) favoured over absolute pressure; early decompression
- Evidence Level
- Based on Level II-III data
There is no orthopaedic registry that systematically captures forearm compartment syndrome in the way arthroplasty registries (AOANJRR, NJR, AJRR) capture joint replacement; incidence and outcome data derive from single-centre and national trauma series rather than registry datasets.
Practice Variation & Regional Considerations
The principal area of international practice variation is the diagnostic pathway: continuous intracompartmental pressure monitoring is favoured in some UK and European units for high-risk or obtunded patients, whereas a clinically-driven "decompress if suspected" approach predominates in many trauma centres internationally (von Keudell 2015, PMID 26460664). The ΔP less than 30 mmHg threshold (McQueen, PMID 8898137) is the most widely adopted pressure criterion worldwide.
In trauma centres internationally, standardised serial neurovascular observation is applied after high-risk fractures, and first-generation cephalosporin prophylaxis (e.g. cefazolin) is the standard at fasciotomy. In rural and remote settings where transfer time may exceed 4-6 hours, local surgeons should have a low threshold to perform fasciotomy before transfer rather than risk irreversible ischaemia in transit. VTE prophylaxis follows standard trauma protocols, with mechanical methods preferred initially given the bleeding risk into freshly decompressed compartments.
MnemonicCards
PRESSCompartment Syndrome Pathophysiology
Hook:PRESS-ure leads to tissue death - urgent decompression breaks the cycle
5 Ps5 Ps of Compartment Syndrome
Hook:Pain out of Proportion is the KEY - do NOT wait for the late Ps!
CURLSVolar Fasciotomy Steps
Hook:CURLS protects fingers - from contracture!
MCQ Practice Points
Q: What is the earliest and most reliable clinical sign of compartment syndrome?
A: Pain out of proportion to the injury, especially pain on passive stretch of the affected compartment. For volar forearm compartment, this is pain with passive finger extension.
Q: What are the compartment pressure thresholds indicating need for fasciotomy?
A: Either absolute pressure greater than 30mmHg OR Delta P less than 30mmHg (where Delta P = diastolic blood pressure minus compartment pressure). Delta P accounts for individual patient perfusion status.
Q: What MUST be included with volar forearm fasciotomy?
A: Carpal tunnel decompression - swelling extends distally into the carpal tunnel and must be released to prevent median nerve compression at the wrist.
Q: Which of the 5 Ps are considered LATE signs of compartment syndrome?
A: Pallor and pulselessness are late signs. Waiting for these findings means irreversible muscle and nerve damage has likely already occurred. Pain, pressure, and paresthesia are earlier findings.
Q: What is the pathological basis of Volkmann's ischemic contracture?
A: Ischemic necrosis of forearm flexor muscles leading to fibrotic replacement. The shortened, fibrotic muscles cause the characteristic posture: wrist flexion, MCP hyperextension, IP joint flexion.
Q: What is the critical time window for fasciotomy in compartment syndrome?
A: 6-8 hours from onset of ischemia. Fasciotomy within 6 hours has significantly better outcomes. After 8 hours, irreversible muscle necrosis and nerve damage are highly likely.
At a Glance Table
- Key Points
- Clinical - pain on passive stretch
- Critical Values
- Absolute pressure greater than 30mmHg OR ΔP less than 30mmHg
- Action
- Urgent fasciotomy
- Key Points
- Muscle necrosis starts at 30 mins
- Critical Values
- Irreversible damage after 6-8 hours
- Action
- Decompress within 6 hours
- Key Points
- Volar superficial, volar deep, dorsal, mobile wad
- Critical Values
- Release volar AND dorsal if any doubt
- Action
- Always include carpal tunnel
- Key Points
- Supracondylar, both-bone forearm, floating elbow
- Critical Values
- Maintain high index of suspicion
- Action
- Serial neurovascular exams
- Key Points
- Volkmann's contracture if untreated
- Critical Values
- Irreversible flexor muscle fibrosis
- Action
- Prevention is key
Key Takeaways
- Pain on passive stretch is the earliest reliable sign
- Clinical diagnosis is sufficient - don't delay for pressures
- Always release carpal tunnel with volar fasciotomy
- Time to fasciotomy determines outcome
- Leave wounds completely open
- Waiting for pulselessness (too late!)
- Delaying surgery for pressure measurement
- Closing wounds primarily
- Attributing pain to fracture alone
- Incomplete fasciotomy
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“8-year-old boy, 6 hours post-supracondylar fracture ORIF. Nurses report severe forearm pain despite regular analgesia. Pain with passive finger extension. Cast has been bivalved.”
“25-year-old motorcyclist with closed both-bone forearm fracture. Moderate forearm pain, compartment feels somewhat tense but not rock-hard. Fingers move but patient reports altered sensation in thumb web space. You are uncertain about the diagnosis.”
“28-year-old presents 6 months after forearm fracture treated elsewhere. He has a fixed flexion deformity of fingers with wrist in flexed position. Extending wrist causes fingers to flex further. He has weak grip and altered sensation.”
Clinical Signs
- Pain OUT OF PROPORTION (earliest)
- Pain on PASSIVE STRETCH (most reliable)
- Tense, wooden compartment
- Paresthesia (nerve ischemia)
- Pallor and pulselessness = TOO LATE
Pressure Thresholds
- Absolute greater than 30 mmHg
- Delta P less than 30 (DBP - compartment pressure)
- Clinical diagnosis SUFFICIENT
- Do NOT delay for pressures if high suspicion
Volar Fasciotomy
- Curvilinear incision elbow to palm
- Release lacertus fibrosus
- Release superficial + deep volar
- ALWAYS add carpal tunnel release
- Protect median nerve throughout
Post-operative
- Leave wounds OPEN
- Loose dressings or VAC
- Splint in position of function
- DPC at 48-72 hours
- STSG if cannot close
High-Risk Fractures
- Supracondylar (children)
- Both-bone forearm
- Floating elbow
- Monteggia/Galeazzi
- High-energy distal radius
Volkmann's Contracture
- Irreversible flexor fibrosis
- Wrist flexed, MCP extended, IP flexed
- Cascade sign positive
- PREVENTION is key - early fasciotomy
Evidence Base
Delta P Threshold for Fasciotomy (Landmark)
- Prospective study of 116 tibial diaphyseal fractures with continuous anterior compartment monitoring for 24 hours; 3 (2.6%) developed acute compartment syndrome.
- Using a differential pressure (diastolic BP minus compartment pressure) threshold of less than 30 mmHg led to NO missed cases; no patient had compartment-syndrome sequelae at minimum six-month review.
- An absolute threshold of greater than 30 mmHg would have led to fasciotomy in 43% of patients, many unnecessary.
Timing of Fasciotomy and Outcomes (Landmark)
- 66 cases of acute compartment syndrome treated by fasciotomy in 46 extremities of 44 patients.
- Fasciotomy performed early (less than 12 hours after onset) gave normal function in 68% of extremities; only 8% of late fasciotomies achieved normal function.
- Complication rates were 4.5% (early) versus 54% (late).
Volkmann's Contracture, Supracondylar Fractures and Prevention (Landmark)
- Review of 55 children (58 limbs) with Volkmann's contracture treated in Toronto 1955-1975.
- Supracondylar fractures of the elbow that progressed to Volkmann's contracture frequently had BOTH an arterial injury and a compartment syndrome.
- Most children had not received early appropriate treatment, and the frequency of contracture had not declined over 21 years despite increased awareness.
Acute Compartment Syndrome of the Upper Extremity (Review)
- Comprehensive review of acute compartment syndrome of the hand, forearm and upper arm.
- Pain out of proportion to injury is the most reliable early symptom; diagnosis is particularly difficult in obtunded patients and young children.
- Early recognition and expeditious fasciotomy are essential to obtain good outcomes and prevent permanent disability and ischaemic contracture.
Acute Compartment Syndrome: Who Is at Risk? (Epidemiology)
- Analysis of 164 consecutive patients with acute compartment syndrome over eight years.
- An associated fracture was present in 69%; forearm compartment syndrome was associated with distal radius fractures and, like the cohort overall, occurred most commonly in young men (typically under 35 years).
- Soft-tissue injury without fracture was the second most common cause; one-tenth had a bleeding disorder or were anticoagulated.
Diagnosis and Treatment of Acute Extremity Compartment Syndrome (Lancet Series)
- Lancet Emergency Surgery Series review summarising upper- and lower-limb acute compartment syndrome in adults and children.
- There is no universally agreed diagnostic standard; some advocate continuous intracompartmental pressure monitoring in high-risk injuries while others favour aggressive fasciotomy when the syndrome is even suspected.
- Ineffective treatment risks permanent dysaesthesia, ischaemic contracture, muscle dysfunction, limb loss and death; fasciotomy itself carries long-term morbidity.