Benign Reactive Giant-Cell Lesion of Small Bones
- GIANT CELL REPARATIVE GRANULOMA (GCRG) is a BENIGN, REACTIVE giant-cell-rich lesion (not a true neoplasm) that most often arises in the SMALL BONES of the HANDS and FEET and in the JAWS (where it is termed central giant cell granuloma); it is now generally regarded as part of the spectrum of GIANT-CELL LESIONS OF THE SMALL BONES (overlapping with the 'solid' aneurysmal bone cyst).
- It presents as a LYTIC, often EXPANSILE lesion of a small tubular bone with cortical thinning and can look locally aggressive on imaging, but it is benign; pain, swelling and sometimes pathological fracture are typical.
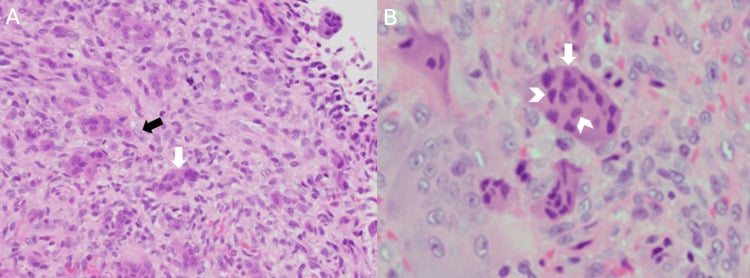
- HISTOLOGICALLY it shows a FIBROUS/cellular stroma containing osteoclast-type GIANT CELLS that are distributed UNEVENLY - clustered, often around foci of HAEMORRHAGE - together with REACTIVE woven BONE and haemosiderin; this UNEVEN, clustered giant-cell pattern (with reactive bone) helps distinguish it from giant cell tumour of bone, in which the giant cells are large and EVENLY distributed throughout a mononuclear stroma.
- The crucial DIFFERENTIAL is GIANT CELL TUMOUR (GCT) OF BONE, which is locally aggressive and - importantly - RARE in the small bones of the hand (it favours the meta-epiphysis of long bones around the knee); a giant-cell-rich lesion of the distal phalanx initially diagnosed as GCRG can recur - at 8 months in a reported case - and prove to be a giant cell tumour, so the diagnosis is genuinely challenging and warrants experienced pathological review.
- UNDERSTAND WHY THE DISTINCTION MATTERS BEYOND NOMENCLATURE. Giant cell tumour of bone metastasises to the LUNG in about 3 PERCENT of cases, and this has been reported from a GCT of the HAND - so labelling an aggressive hand giant-cell lesion a 'reparative granuloma' is not a harmless naming error. It changes the adequacy of the excision, the need for chest imaging, and the surveillance the patient receives.
- Other DIFFERENTIALS to consider for a giant-cell-rich lytic lesion of a small bone include the BROWN TUMOUR of hyperparathyroidism (check calcium/PTH), ANEURYSMAL BONE CYST, and (rarely) more aggressive lesions - so biochemistry and correlation of imaging with histology are part of the work-up.
- MANAGEMENT is CURETTAGE (with bone grafting) for most lesions, which is usually effective, but local RECURRENCE is well recognised and NO SERIES GIVES A RELIABLE RATE for the small bones - the published literature is case reports and small series, so counsel that recurrence happens without quoting a percentage you cannot support. Follow-up is needed and recurrent or aggressive lesions may require more extensive excision (occasionally amputation of a digit) and confirmation of the diagnosis - because a 'recurrent GCRG' may turn out to be a giant cell tumour.
- “Giant cell reparative granuloma = BENIGN, REACTIVE giant-cell lesion of the SMALL BONES of the hands/feet (and JAWS = central giant cell granuloma); part of the giant-cell-lesion-of-small-bones / solid ABC spectrum.
- “Histology: fibrous stroma + UNEVENLY/clustered giant cells around HAEMORRHAGE + reactive bone (vs GCT of bone = large, EVENLY distributed giant cells).
- “Key differential = giant cell tumour of bone (locally aggressive, RARE in the hand). Also brown tumour (check Ca/PTH), ABC. Treat by curettage +/- grafting and follow up - recurrence is recognised but no dependable rate is published for the small bones.
- “State the stakes: GCT of bone metastasises to the LUNG in about 3%, reported even from a HAND lesion - so a mislabelled aggressive giant-cell lesion changes the adequacy of excision, whether the chest is imaged, and the surveillance. Treat a recurrence as a DIAGNOSTIC event: fresh tissue, H3.3 G34W immunostain (positive in GCT only), and calcium/PTH.
Small bones of hands/feet (and jaws); fibrous stroma with unevenly clustered giant cells around haemorrhage + reactive bone. Curettage (can recur).
Rare in the hand; locally aggressive; large, evenly distributed giant cells in a mononuclear stroma. A 'recurrent GCRG' may prove to be a GCT - review carefully.
What Is Actually at Stake in the GCRG-versus-GCT Call
The two lesions are usually contrasted on histology and site, which makes the distinction sound academic. It is not. Giant cell tumour of bone metastasises to the lung in roughly 3 percent of cases, and this has been reported from a giant cell tumour arising in a hand, where the tumour is supposedly rare. So calling an aggressive giant-cell lesion of a phalanx a reparative granuloma is not a naming error - it changes whether the excision is adequate, whether the chest is imaged, and how the patient is followed. The reported phalangeal case that recurred at 8 months and proved to be a giant cell tumour ended in amputation of the fingertip.
Recurrence after curettage is real and repeatedly described, but the literature on giant-cell lesions of the small bones is case reports and small series, and no cohort supplies a dependable recurrence rate. The right counselling is that these lesions can come back and need follow-up - not a percentage. If a number is quoted in an exam it should be attributed to the series it came from.
Treat a recurrence as a diagnostic event, not just a surgical one. Send fresh tissue, ask specifically for H3.3 G34W immunohistochemistry - positive in giant cell tumour, negative in reparative granuloma, brown tumour and aneurysmal bone cyst - and check calcium and PTH if that was not done initially. A lesion that behaves aggressively is telling you something the first report may have missed.
Features, Histology & Differential
GCRG is a benign, reactive giant-cell-rich lesion (not a true neoplasm), most often of the small bones of the hands/feet and the jaws (central giant cell granuloma), within the giant-cell-lesion-of-small-bones / solid ABC spectrum. It is lytic and expansile with cortical thinning and can look aggressive but is benign. Histology shows a fibrous stroma with unevenly distributed/clustered osteoclast-type giant cells (often around haemorrhage) plus reactive woven bone and haemosiderin - distinguishing it from giant cell tumour of bone (large, evenly distributed giant cells; locally aggressive; rare in the hand). Also consider the brown tumour of hyperparathyroidism (check calcium/PTH) and aneurysmal bone cyst.
- Giant cell reparative granuloma
- Benign, reactive
- Giant cell tumour of bone
- Benign but locally aggressive neoplasm
- Giant cell reparative granuloma
- Small bones of hands/feet; jaws
- Giant cell tumour of bone
- Meta-epiphysis of long bones (around knee); rare in hand
- Giant cell reparative granuloma
- Uneven/clustered (around haemorrhage)
- Giant cell tumour of bone
- Large, evenly distributed throughout stroma
- Giant cell reparative granuloma
- Fibrous stroma, reactive woven bone, haemosiderin
- Giant cell tumour of bone
- Mononuclear stromal cells (the neoplastic component)
- Giant cell reparative granuloma
- Curettage (+/- grafting); can recur
- Giant cell tumour of bone
- Extended curettage +/- adjuvants; denosumab; recurrence

Molecular Discriminators of the Giant-Cell-Rich Differential
- The molecular discriminators. When giant-cell-rich lesions overlap, markers help: giant cell tumour of bone carries the H3F3A (H3.3) G34W mutation - an H3.3 G34W immunostain is positive in GCT and negative in GCRG/brown tumour/ABC/chondroblastoma - the single most useful marker when GCRG-versus-GCT is in doubt. Primary aneurysmal bone cyst carries a USP6 rearrangement (FISH-positive), whereas the histologically-overlapping GCRG/central-giant-cell-granuloma is USP6-negative. Chondroblastoma carries a different mutation (H3F3B K36M, H3K36M-positive).
- The fuller giant-cell-rich differential. Beyond GCT, brown tumour and ABC, consider chondroblastoma (epiphyseal, child, chondroid matrix, H3K36M-positive), non-ossifying fibroma (metaphyseal, cortical, sclerotic rim, self-limiting), and - the one not to miss - a giant-cell-rich osteosarcoma (atypical stroma with malignant osteoid).
Q: What molecular markers help distinguish GCRG from the other giant-cell-rich lesions?
A: Giant cell tumour of bone carries the H3F3A (H3.3) G34W mutation → H3.3 G34W IHC positive in GCT, negative in GCRG/brown tumour/ABC (the key GCRG-vs-GCT discriminator). Primary aneurysmal bone cyst carries a USP6 rearrangement (FISH-positive), whereas GCRG/central-giant-cell-granuloma is USP6-negative. Chondroblastoma carries a different mutation (H3F3B K36M, H3K36M-positive). The fuller differential also includes non-ossifying fibroma and the malignant giant-cell-rich osteosarcoma (not to miss).
The Jaw Form, Syndromic Associations, and Medical Treatment
- Central giant cell granuloma of the jaw. The intraosseous giant-cell lesion of the mandible/maxilla (commonest in the anterior mandible, in patients under 30, with a female predominance); it may be non-aggressive (slow, asymptomatic) or aggressive (pain, rapid growth, cortical perforation, root resorption, high recurrence). Distinguish it from the peripheral giant cell granuloma - a soft-tissue gingival lesion on the gum.
- The syndromic associations. Multiple or syndromic giant-cell lesions occur in Noonan syndrome, neurofibromatosis type 1, and cherubism (SH3BP2 gene; bilateral symmetric mandibular lesions in a child, self-limiting after puberty) - part of the RASopathy spectrum - so multiple lesions warrant a genetics work-up.
- The medical/adjuvant treatments. Beyond curettage, aggressive or jaw lesions can be treated with intralesional corticosteroid injections, calcitonin, interferon-alpha, or denosumab (anti-RANKL, shrinking the osteoclastic component of aggressive/unresectable lesions) - sparing more morbid resection.
Q: Describe the jaw form of GCRG, its syndromic associations, and the medical treatments.
A: Central giant cell granuloma is the intraosseous jaw lesion (commonest in the anterior mandible, under 30, female predominance), non-aggressive or aggressive (pain/perforation/root resorption/recurrence); the peripheral form is a soft-tissue gingival lesion. Multiple/syndromic giant-cell lesions occur in Noonan syndrome, NF1 and cherubism (SH3BP2, bilateral mandibular, self-limiting) - the RASopathy spectrum. Beyond curettage, medical options for aggressive/jaw lesions include intralesional corticosteroids, calcitonin, interferon-alpha, and denosumab (anti-RANKL).
Management
- Work-up: imaging (lytic/expansile small-bone lesion); biochemistry (calcium/PTH to exclude a brown tumour); biopsy/histology at a centre experienced in bone tumours.
- Treatment: curettage with bone grafting for most lesions - usually effective.
- Follow up: local recurrence is well recognised, though no series gives a dependable rate for the small bones - counsel that it can recur rather than quoting a percentage.
- Recurrent/aggressive disease: more extensive excision (occasionally digital amputation) and re-confirm the diagnosis - a 'recurrent GCRG' may prove to be a giant cell tumour of bone, which metastasises to the lung in around 3 percent of cases.
The lesions this must be separated from each have their own page, and the separation is what the work-up is for. The aggressive neoplasm at the other end is giant cell tumour of bone; the metabolic mimic is the brown tumour of hyperparathyroidism, which is why calcium and PTH are checked; and the lesion sharing both morphology and part of the spectrum is aneurysmal bone cyst. Two further giant-cell-rich lesions complete the differential - chondroblastoma, which is epiphyseal and H3K36M-positive, and non-ossifying fibroma.
The practical trap with giant cell reparative granuloma is diagnostic overlap with other giant-cell-rich lesions, especially giant cell tumour of bone. GCRG is a benign, reactive lesion of the small bones of the hands and feet (and jaws), with a fibrous stroma and unevenly clustered giant cells around haemorrhage and reactive bone, and it is treated by curettage and grafting. Giant cell tumour of bone, by contrast, is a locally aggressive neoplasm with large, evenly distributed giant cells, and it is rare in the hand - so a giant-cell-rich lesion of a phalanx diagnosed as GCRG that then recurs should prompt re-review of the histology, because it may in fact be a giant cell tumour requiring different, more aggressive management. The work-up should also exclude the brown tumour of hyperparathyroidism with calcium and PTH, and aneurysmal bone cyst is in the spectrum. Because GCRG has a notable recurrence rate, follow-up is needed, and recurrent or aggressive lesions warrant both more extensive surgery and a fresh, experienced pathological assessment of the diagnosis.
Mnemonics & Memory Aids
REPAIR
Hook:REPAIR: Reactive benign, Extremity small bones/jaws, Pattern (uneven/clustered + reactive bone), vs GCT (even/aggressive), Investigate Ca/PTH, Resect/curette + Recurrence (re-confirm).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A lytic, expansile lesion of a phalanx shows a giant-cell-rich histology. How do you approach the diagnosis and management?”
What it is
- Benign, reactive giant-cell-rich lesion (not a true neoplasm)
- Small bones of hands/feet and the jaws (central giant cell granuloma)
- Part of the giant-cell-lesion-of-small-bones / solid ABC spectrum
Histology
- Fibrous/cellular stroma; unevenly distributed/clustered giant cells
- Often around foci of haemorrhage; reactive woven bone + haemosiderin
- Contrast: GCT of bone = large, evenly distributed giant cells
Differential & work-up
- Giant cell tumour of bone (locally aggressive; rare in hand)
- Brown tumour (check calcium/PTH); aneurysmal bone cyst
- Imaging + biochemistry + experienced histology review
Management
- Curettage (+/- grafting) - usually effective
- Recurrence recognised but no dependable published rate for the small bones - follow up
- The stakes: GCT metastasises to lung in ~3 percent, reported even from a hand lesion
- Recurrent/aggressive: re-confirm diagnosis (may be GCT) + more extensive surgery
Evidence & Key Studies
Giant-cell lesion of the distal phalanx initially diagnosed as reparative granuloma, recurring as giant cell tumour
- Giant cell tumours of bone are locally aggressive neoplasms that typically occur in the distal femur or proximal tibia and infrequently in the bones of the hand, including the distal phalanx.
- A distal-phalanx lesion underwent curettage with a working diagnosis of giant cell reparative granuloma (with focal fracture callus), but recurred at 8 months and, on histopathology, was confirmed to be a giant cell tumour of bone (requiring amputation of the distal phalanx tip).
- In rare and difficult-to-diagnose giant-cell lesions, consultation with experienced pathologists improves diagnostic accuracy and prevents treatment delays - underscoring the GCRG/GCT diagnostic overlap.
Multiple pulmonary metastases from giant cell tumor of a hand
- Giant cell tumour of bone classically involves the epiphysis of long bones and only rarely the small bones of the hands and feet, but despite being benign it destroys bone, recurs locally and can metastasise.
- Approximately 3 percent of giant cell tumours metastasise to the lung. This report describes multiple pulmonary metastases from a giant cell tumour of the hand in a 54-year-old man, found incidentally as asymptomatic nodules on a routine chest radiograph.
- He achieved near-complete remission with adriamycin and cisplatin. As a single case report it establishes that the event can occur from a hand lesion, not how often - the 3 percent figure refers to giant cell tumours at all sites.
The diagnostic overlap and challenge between giant cell reparative granuloma and giant cell tumour of bone in the small bones of the hand (a phalangeal lesion diagnosed as GCRG recurring and proving to be a giant cell tumour), the rarity of giant cell tumour in the hand, and the value of experienced pathological review come from the cited DeFrancisis report. The benign reactive nature of GCRG, its location in the small bones of the hands/feet and jaws, the histological distinction (uneven/clustered giant cells with reactive bone vs even distribution in GCT), the brown-tumour/ABC differentials, and curettage-with-recurrence management are standard, well-established teaching. The roughly 3 percent pulmonary-metastasis figure for giant cell tumour of bone, and its occurrence from a hand lesion, come from the Moon report - a single case, which establishes that it can happen rather than how often. No cohort gives a dependable local-recurrence rate for giant-cell reparative granuloma of the small bones; the literature is case reports and small series, so no percentage is quoted here. Nor is there a validated follow-up interval, a size or site threshold that mandates wider excision, or a randomised comparison of curettage against any medical adjuvant in this lesion.