Massive Osteolysis / Vanishing Bone Disease
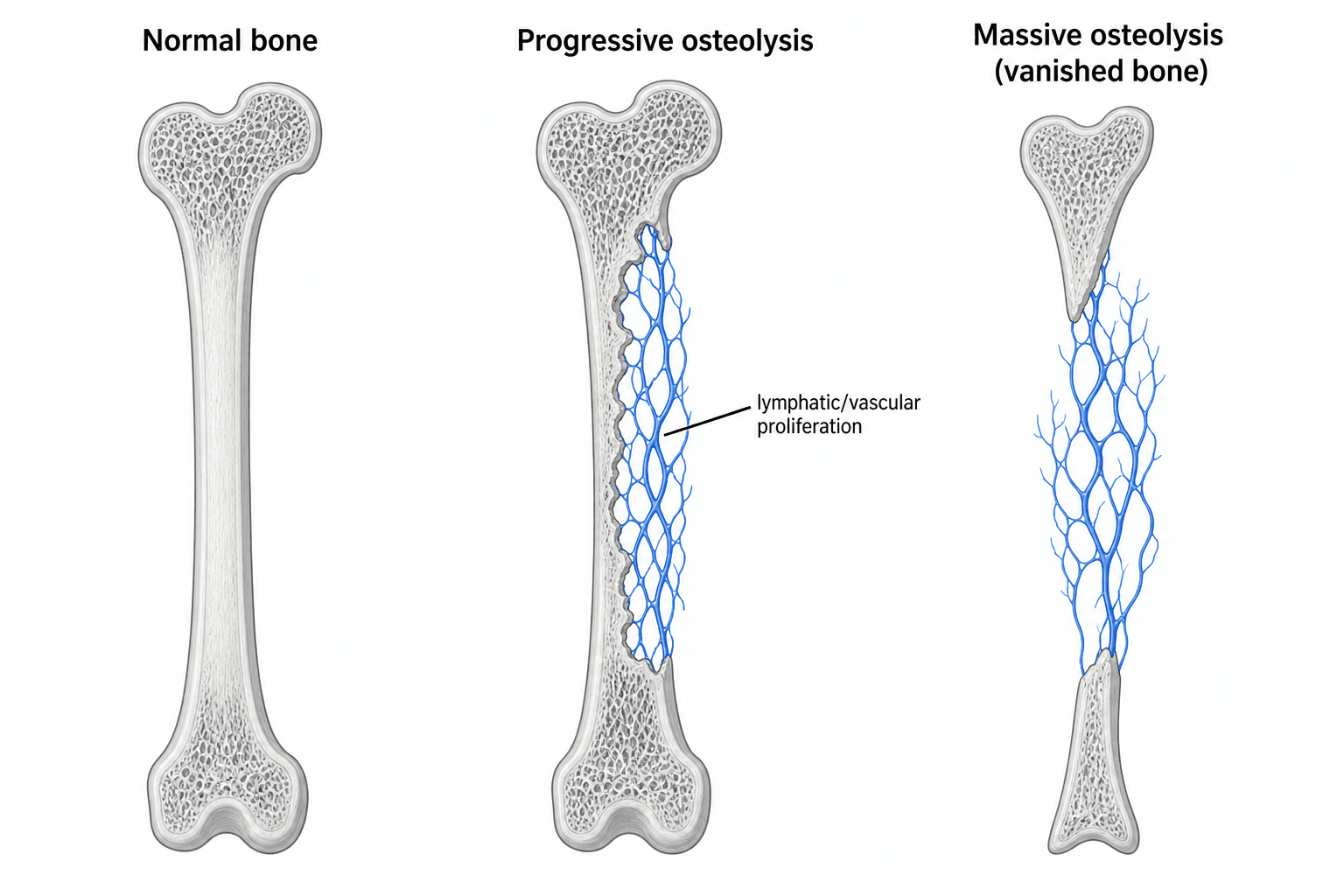
- Gorham-Stout disease (GSD) - massive osteolysis, 'vanishing bone' or 'phantom bone' disease - is a RARE disorder (only a few hundred cases reported) of PROGRESSIVE, SPONTANEOUS, idiopathic OSTEOLYSIS, in which an abnormal proliferation of LYMPHATIC and vascular channels within bone resorbs it and replaces it with fibrous/angiomatous tissue, so the bone literally 'disappears' on serial radiographs.
- It can occur at any age but predominantly affects CHILDREN and young adults (with a slight male predominance), and although any bone may be involved it has a predilection for the AXIAL and girdle skeleton - the SPINE, RIBS, pelvis/hip, shoulder girdle, MANDIBLE and skull - frequently with MULTIPLE lesions that can cross joints.
- PAIN is the commonest symptom, with progressive swelling, deformity and PATHOLOGICAL FRACTURE; the hallmark is the documented PROGRESSIVE LOSS OF BONE on serial imaging, often with tapering/pointed bone ends ('sucked candy' appearance).
- The FEARED complication is CHYLOTHORAX / pleural effusion when the thoracic skeleton (ribs/spine) is involved: the proliferating lymphatics leak chyle into the pleural space, causing respiratory compromise - PLEURAL EFFUSION is a recognised RISK FACTOR FOR MORTALITY and demands close monitoring.
- Diagnosis is one of EXCLUSION: there are no agreed criteria, so it rests on demonstrating PROGRESSIVE osteolysis on serial imaging together with characteristic HISTOLOGY (proliferating thin-walled vascular/lymphatic channels with fibrosis, NO malignant cells and NO osteoblastic/reparative response), after EXCLUDING infection, malignancy (metastasis, myeloma), metabolic and other causes of osteolysis.
- There is NO consensus treatment: options include ANTIRESORPTIVES (bisphosphonates), the mTOR inhibitor SIROLIMUS (which targets the lymphatic proliferation and is increasingly used), interferon-alpha, RADIOTHERAPY, and SURGERY (resection, reconstruction/allograft, stabilisation, fracture management); chylothorax is managed with thoracic-duct ligation/embolisation, octreotide, a low-fat/MCT diet and pleurodesis. The course is unpredictable - some stabilise spontaneously.
- “Gorham-Stout = progressive spontaneous massive osteolysis ('vanishing bone') from intraosseous LYMPHATIC/vascular proliferation.
- “Axial/girdle predilection (spine, ribs, pelvis, shoulder, mandible); CHYLOTHORAX (thoracic involvement) is the feared, mortality-associated complication.
- “Diagnosis of EXCLUSION (progressive osteolysis + benign vascular/lymphatic histology, no malignancy). Treat with bisphosphonates / SIROLIMUS / radiotherapy / surgery; no consensus.
Progressive, spontaneous osteolysis on serial imaging - bone 'vanishes' and is replaced by lymphatic/vascular tissue. A diagnosis of exclusion.
Chylothorax when ribs/spine are involved (lymphatic leak into the pleura) - a recognised cause of mortality; monitor and treat aggressively.
Pathology & Presentation
In Gorham-Stout disease, an abnormal proliferation of lymphatic and vascular channels invades bone and drives its progressive resorption, replacing the bone with fibrous/angiomatous tissue - hence 'vanishing' or 'phantom' bone. It predominantly affects children and young adults, with a slight male predominance, and although any bone can be involved it favours the axial and girdle skeleton (spine, ribs, pelvis, shoulder, mandible, skull), often with multiple lesions that may cross joints. Patients present with pain (the commonest symptom), swelling, deformity and pathological fracture, and the diagnostic hallmark is documented progressive bone loss on serial radiographs, classically with tapered/pointed bone ends.
Diagnosis & Management
There are no universally agreed diagnostic criteria, so GSD is a diagnosis of exclusion requiring:
- Progressive osteolysis demonstrated on serial imaging (radiographs/CT/MRI; bone scintigraphy).
- Characteristic HISTOLOGY: proliferating thin-walled vascular/lymphatic channels with fibrous replacement, NO malignant cells and NO osteoblastic/reparative response.
- EXCLUSION of other causes of osteolysis - infection (osteomyelitis), malignancy (metastasis, myeloma, primary bone tumour), metabolic and endocrine disease, and other rare osteolyses.
- Assess for thoracic involvement and chylothorax (chest imaging) given its prognostic importance.
- Medical: bisphosphonates (antiresorptive), the mTOR inhibitor SIROLIMUS (targets the lymphatic proliferation - increasingly first-line), and interferon-alpha.
- Radiotherapy: can arrest progression in selected lesions.
- Surgery: resection of affected bone with reconstruction (allograft/prosthesis), stabilisation and management of pathological fractures - though osteolysis can recur in or around constructs.
- Chylothorax: thoracic-duct ligation/embolisation, octreotide, a low-fat/MCT diet, drainage and pleurodesis; multidisciplinary care.
- The course is unpredictable - some lesions stabilise spontaneously while others progress relentlessly.
The single most important surgical principle: conventional bone graft is eaten by the disease. This is not a theoretical risk but the consistent experience since the condition was characterised - grafting has proved disappointing because the graft itself undergoes osteolysis, and there is no regeneration after the resorption to compensate. A cancellous or structural allograft placed into active disease is a further meal for the process, and the reconstruction fails. Four consequences follow, and together they are the answer to "how would you reconstruct this?":
- What it means in practice
- Avoid cancellous or structural allograft as the sole reconstruction in active disease
- Why
- The graft is resorbed by the same process; failure is the rule, not the exception
- What it means in practice
- Endoprosthesis, or a vascularised fibular transfer where biological reconstruction is wanted
- Why
- A vascularised graft carries its own blood supply and behaves as living bone rather than a scaffold to be resorbed; a prosthesis is not made of bone at all
- What it means in practice
- Long constructs; anchor points chosen outside the lytic segment and beyond it
- Why
- Fixation held by disease-bearing bone loosens as that bone disappears
- What it means in practice
- Control the disease medically first - and consider adjuvant radiotherapy or continued systemic therapy around surgery - reserving urgent surgery for instability, fracture or cord compression
- Why
- Reconstructing into a bone that is still dissolving is reconstructing into a moving target
Amputation retains a place in the rare limb rendered unreconstructable and painful by relentless progression, and saying so is not defeatism: it is the honest end of a spectrum in a disease with no reliable cure, and an examiner asking about the limits of reconstruction is asking whether the candidate knows it.
Because GSD favours the axial skeleton, thoracic (rib/spine) involvement can cause chylothorax, which is the leading cause of death in this disease through respiratory compromise and nutritional/immune depletion from chyle loss. Any patient with thoracic GSD and a pleural effusion needs urgent multidisciplinary management. Equally, because GSD is rare and mimics infection or malignancy, do NOT diagnose it without excluding those treatable/serious alternatives with biopsy and the appropriate workup.
The Criteria You Are Expected to Produce
No consensus criteria exist, which is not the same as no criteria at all. The set that is actually cited, and the one to have ready when an examiner asks how the diagnosis is made, is the eight criteria described by Heffez and colleagues in 1983:
- Criterion
- Biopsy showing angiomatous tissue - proliferating thin-walled vascular and lymphatic channels
- What it rules out
- Confirms the lesional tissue rather than inferring it from the radiograph
- Criterion
- Absence of cellular atypia
- What it rules out
- Angiosarcoma, epithelioid haemangioendothelioma, metastatic carcinoma
- Criterion
- Minimal or no osteoblastic response and absence of dystrophic calcification
- What it rules out
- Healing fracture, infection, tumour with reactive bone - anything that tries to rebuild
- Criterion
- Evidence of local progressive bony resorption
- What it rules out
- Static lytic lesions; this is the criterion that requires SERIAL imaging and therefore time
- Criterion
- Non-expansile, non-ulcerative lesion
- What it rules out
- Expansile tumours such as aneurysmal bone cyst or giant cell tumour
- Criterion
- Absence of visceral involvement
- What it rules out
- Generalised lymphatic anomaly and disseminated disease
- Criterion
- Osteolytic radiographic pattern
- What it rules out
- Sclerotic or mixed lesions
- Criterion
- Negative hereditary, metabolic, neoplastic, immunological and infectious aetiology
- What it rules out
- The whole differential below - this criterion is the diagnosis of exclusion in one line
Criterion 4 is the one that costs time. Progressive resorption can only be shown by comparing images separated by an interval, which is why the average interval from first symptom to diagnosis in a systematic review of 206 patients was 3.5 years. A single radiograph, however striking, cannot make this diagnosis.
The blood tests are normal, and that is a finding rather than an absence of one. Serum calcium, phosphate, alkaline phosphatase and parathyroid hormone are characteristically within normal limits despite dramatic bone destruction. Normal calcium and PTH exclude hyperparathyroidism and its brown tumours; a normal alkaline phosphatase is consistent with criterion 3, since there is no osteoblastic response to raise it; and the absence of a paraprotein and of anaemia or renal impairment argues against myeloma. Record them, because "the biochemistry was normal" is part of the positive case, not a gap in the work-up.
What You Exclude: The Family of Osteolyses
Because GSD is a diagnosis of exclusion, the diagnosis is only as good as the list of things excluded, so the other osteolyses have to be known by name. Think in two groups:
- Secondary (acquired) osteolysis - exclude first, because these are treatable/serious: infection (osteomyelitis), malignancy (metastasis, myeloma, primary bone tumour, primary bone lymphoma), hyperparathyroidism / brown tumours, neuropathic (Charcot) destruction, aggressive synovial disease (PVNS), and periprosthetic wear-particle osteolysis or distal-clavicular osteolysis in the relevant settings (each developed in Metastatic Bone Disease, Multiple Myeloma, Primary Bone Lymphoma, Hyperparathyroidism, THA Wear Osteolysis and Distal Clavicle Osteolysis). Biopsy and the appropriate work-up settle these.
- Primary / idiopathic ("essential") osteolyses: GSD is classically grouped as the massive (regional) osteolysis type within classifications of idiopathic osteolysis (e.g. the Hardegger grouping). It is distinguished from the hereditary multicentric osteolyses - which are typically carpal/tarsal, inherited, and may carry a nephropathy - and from acro-osteolysis syndromes (e.g. Hajdu-Cheney).
The features that mark out Gorham-Stout are: it is massive, progressive and regional (often crossing joints, ignoring the usual anatomical boundaries), driven by a lymphatic/vascular proliferation on histology, sporadic (non-hereditary), has no nephropathy, and shows no osteoblastic/reparative response - the bone simply disappears and is not rebuilt.
"Exclude other osteolyses" means two lists: the secondary ones (infection, metastasis/myeloma, brown tumours, periprosthetic wear) ruled out by biopsy/work-up, and the primary idiopathic ones - GSD is the massive, regional, lymphatic, non-hereditary, no-nephropathy, no-reparative-response form, versus the hereditary multicentric (carpal/tarsal, often with nephropathy) osteolyses.
The Spine: the Commonest Site and the Second Way This Disease Disables
The spine is involved in 46% of reported patients - more often than the ribs, the hip or the mandible - and it is the site at which the disease does harm by a mechanism entirely separate from the chylothorax.
What goes wrong. Vertebral body resorption removes anterior column support, so the segment collapses and kyphoses. Because there is no reparative response, the deformity does not stabilise the way a healed compression fracture does; the bone continues to disappear beneath any construct. Resorption of the posterior elements or extension of the angiomatous soft tissue into the canal adds direct compression. The result is progressive kyphotic deformity, instability and myelopathy or paraparesis, which in the reported literature sits alongside chylothorax as the reason patients die or are permanently disabled. Thoracic disease is particularly unforgiving because the canal is narrowest there and the cord's blood supply most tenuous.
What to do about it. Involvement of a vertebral body is an indication for baseline MRI of the whole spine - not a single level, because lesions are multiple in 77% of patients and a contiguous segment may be silently involved - and for serial neurological examination with a documented level rather than a global impression. Progressive deformity, instability or any neurological sign is an indication for stabilisation, and the operative principle is the same one that governs surgery anywhere in this disease: instrument beyond the affected segments into bone that is not involved, because fixation anchored in disease-bearing bone will loosen as that bone dissolves. Systemic therapy is started alongside, not instead of, stabilisation where the cord is threatened.
The chest and the spine are not separate problems here. Thoracic vertebral and rib disease frequently coexist, so a patient presenting with vertebral collapse needs the chest imaged for effusion, and a patient with a chylothorax needs the spine imaged for the lesion that will disable them later.
Imaging: What Each Modality Adds (and the Cold Bone Scan)
- Radiographs / CT: document the progressive resorption on serial films (the diagnostic hallmark), the cortical thinning and concentric "sucked-candy"/tapered pointed ends, and any pathological fracture; CT is best for cortical and calvarial detail and surgical planning.
- MRI: defines the marrow and soft-tissue extent of the abnormal lymphatic/angiomatous tissue (typically T2-hyperintense) - important for mapping disease beyond bone, for the mediastinum/chest, and for planning resection or radiotherapy.
- Bone scintigraphy - the discriminator: the vanished bone characteristically shows reduced or absent uptake because there is no osteoblastic/reparative response; this "cold" pattern helps separate GSD from the typically hot aggressive lytic processes (metastasis, osteomyelitis).
- Lymphatic imaging: lymphoscintigraphy / MR lymphangiography (and conventional/intranodal lymphangiography) demonstrate the abnormal lymphatics, the site of chyle leak and the thoracic-duct anatomy - directly guiding thoracic-duct embolisation when there is a chylothorax.
Serial radiographs/CT show the progressive resorption with tapered pointed ends; MRI maps the lymphatic/angiomatous soft-tissue extent; the bone scan is characteristically COLD (no reparative osteoblastic response - unlike hot metastasis/infection); and lymphangiography/lymphoscintigraphy localise the chyle leak to guide duct embolisation.
Mnemonics & Memory Aids
VANISH
Hook:The bone VANISHes - lymphatic-driven osteolysis; watch for chylothorax.
EXCLUDE
Hook:GSD is a diagnosis you EXCLUDE others to reach.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A young patient has progressive, spontaneous disappearance of bone on serial radiographs. What is the diagnosis, and how is it confirmed?”
“How is Gorham-Stout disease treated, and why is the chest important?”
What it is
- Rare progressive spontaneous massive osteolysis ('vanishing/phantom bone')
- Intraosseous lymphatic/vascular proliferation -> bone resorbed, replaced by fibrous/angiomatous tissue
- Children/young adults; slight male predominance; axial/girdle predilection
Presentation
- Pain (commonest), swelling, deformity, pathological fracture
- Progressive bone loss on serial imaging (tapered ends)
- Chylothorax with thoracic (rib/spine) involvement - mortality risk
Diagnosis (exclusion)
- Progressive osteolysis on serial imaging
- Histology: thin-walled vascular/lymphatic channels, no malignancy, no osteoblastic response
- Exclude infection, malignancy (metastasis/myeloma), metabolic causes
Treatment (no consensus)
- Bisphosphonates, sirolimus (mTOR inhibitor), interferon-alpha
- Radiotherapy; surgery (resection/reconstruction/stabilisation)
- Chylothorax: duct ligation/embolisation, octreotide, low-fat/MCT diet, pleurodesis
Evidence & Key Studies
Clinical features and current management of Gorham-Stout disease: a systematic review
- Gorham-Stout disease is a rare complex lymphatic malformation (~400 cases reported); among 206 reviewed patients it most often presented in childhood with a slight male predominance.
- Osteolysis predominantly affected the axial skeleton (spine 46%, ribs 29%, hip 23%, femur 18%, mandible 16%), usually with multiple lesions, and pain was the commonest symptom.
- Surgery (67%) and bisphosphonates (57%) remained mainstream with sirolimus in 18%; PLEURAL EFFUSION was a significant risk factor for mortality.
Management of refractory chylothorax in Gorham-Stout disease: a case report
- GSD is a rare lymphatic-origin disease with progressive osteolysis that commonly causes chylothorax from leakage of lymph from dissolved bone.
- Refractory chylothorax was managed with thoracic-duct embolisation, octreotide, a low-fat diet and surgery, and disease progression was halted after introducing SIROLIMUS.
- Illustrates the chylothorax complication and the role of sirolimus and multidisciplinary care.
Perspectives on massive osteolysis - the source of the eight diagnostic criteria
- Set out the eight criteria still used to make the diagnosis, combining angiomatous histology without atypia, absent osteoblastic response, documented progressive resorption and exclusion of all other aetiologies.
- Emphasised that there is NO regeneration following the osteolysis - the basis of the absent reparative response on imaging and histology.
- Recorded that bone grafting has proved disappointing because the graft itself undergoes osteolysis - the origin of the modern preference for vascularised or prosthetic reconstruction.
- Noted that attempts to arrest the process with chemotherapy or radiotherapy were generally unsuccessful in the era described, which is the historical baseline against which sirolimus is now judged.
The lymphatic-malformation basis, the childhood/axial predominance, the treatment patterns (surgery, bisphosphonates, sirolimus) and pleural effusion as a mortality risk factor come from the cited Zhou systematic review, and the chylothorax complication and sirolimus/multidisciplinary management from the cited Yamaki case report. The 'vanishing bone' radiographic hallmark, the diagnosis-of-exclusion approach and the characteristic benign vascular histology are standard, well-established teaching. The eight diagnostic criteria, the absence of regeneration after resorption and the resorption of conventional bone graft come from the cited Heffez report. The 46% spinal involvement, the 77% rate of multiple lesions and the 3.5-year average interval from symptom onset to diagnosis are from the Zhou systematic review. (See also Metastatic Bone Disease, Multiple Myeloma, Osteomyelitis Pathophysiology and Primary Bone Lymphoma.)