Mechanical axis planning, temporary hemiepiphysiodesis and rebound surveillance
- Separate physiological genu varum or valgum from pathological deformity before planning treatment.
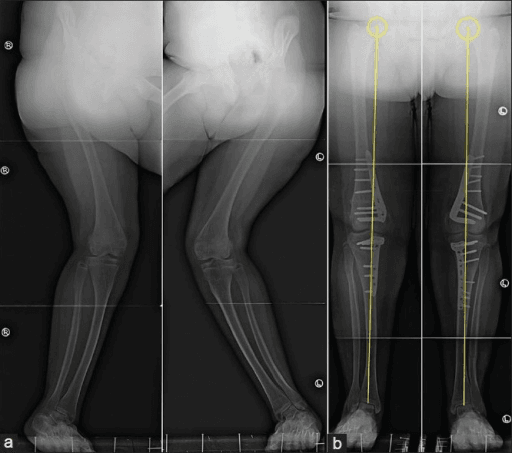
- Plan from standing hip-to-ankle radiographs, not cropped knee images.
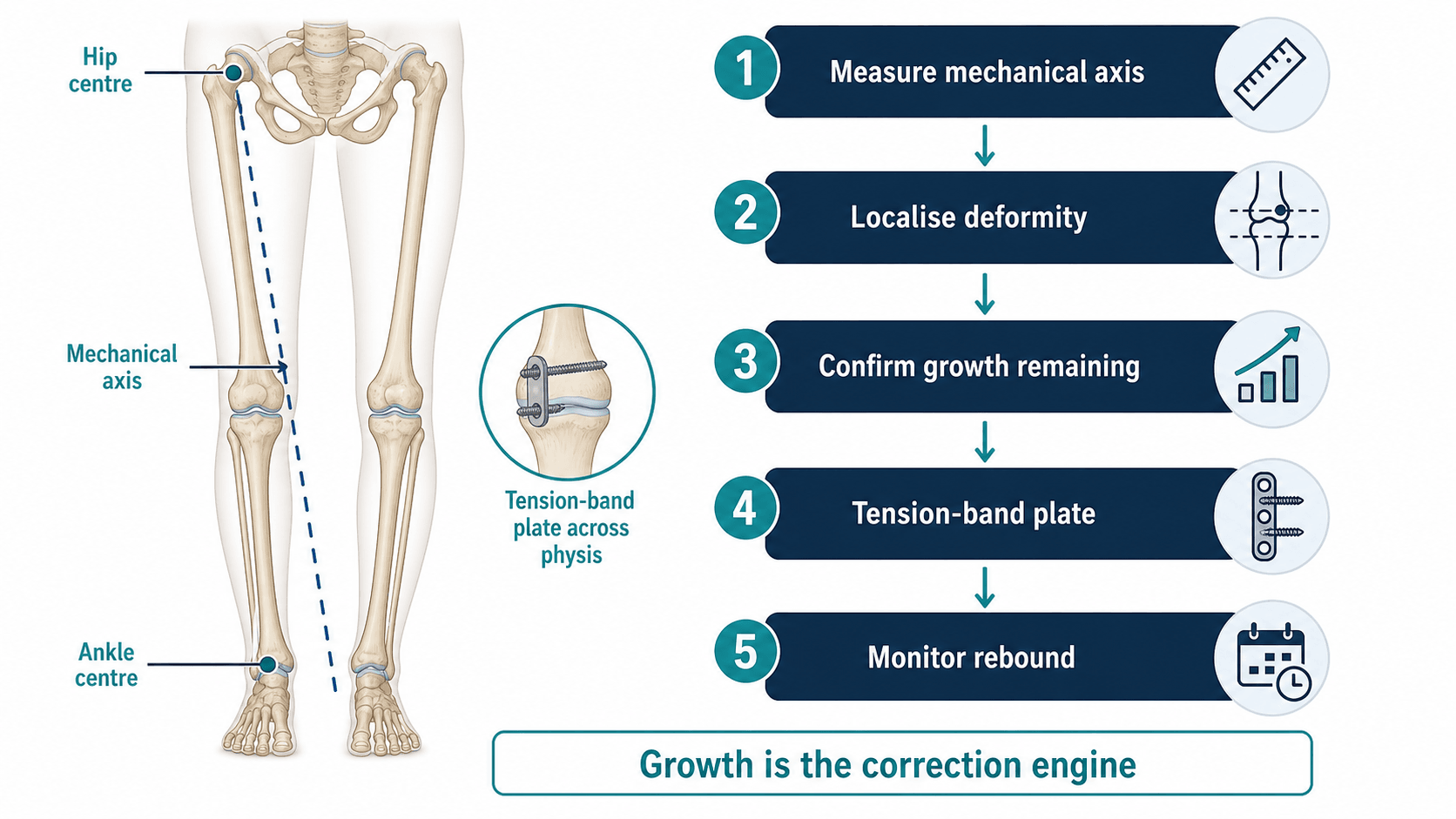
- Mechanical axis deviation tells you the effect; LDFA, MPTA and JLCA help identify the source.
- Guided growth requires open physes and enough growth remaining.
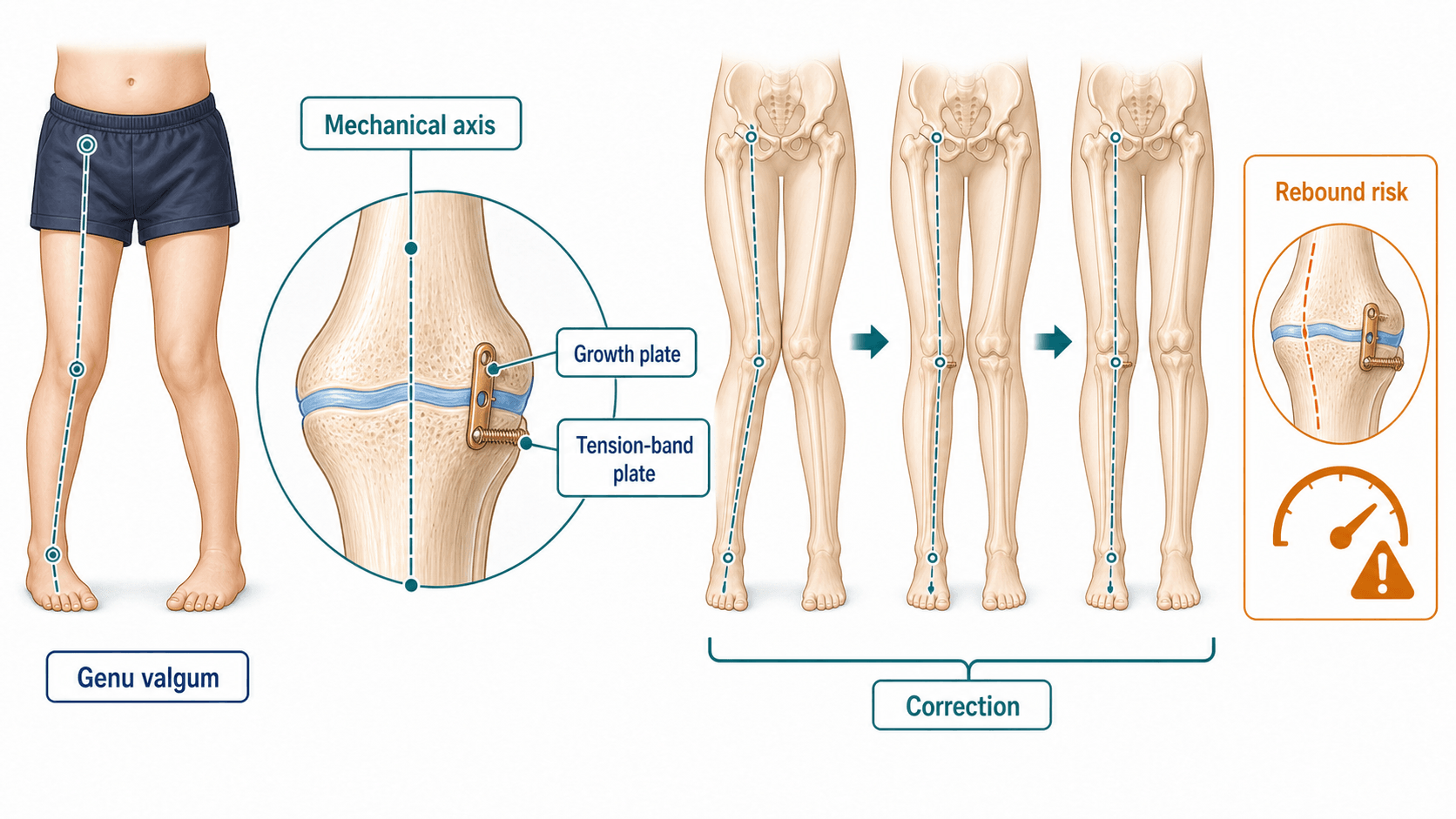
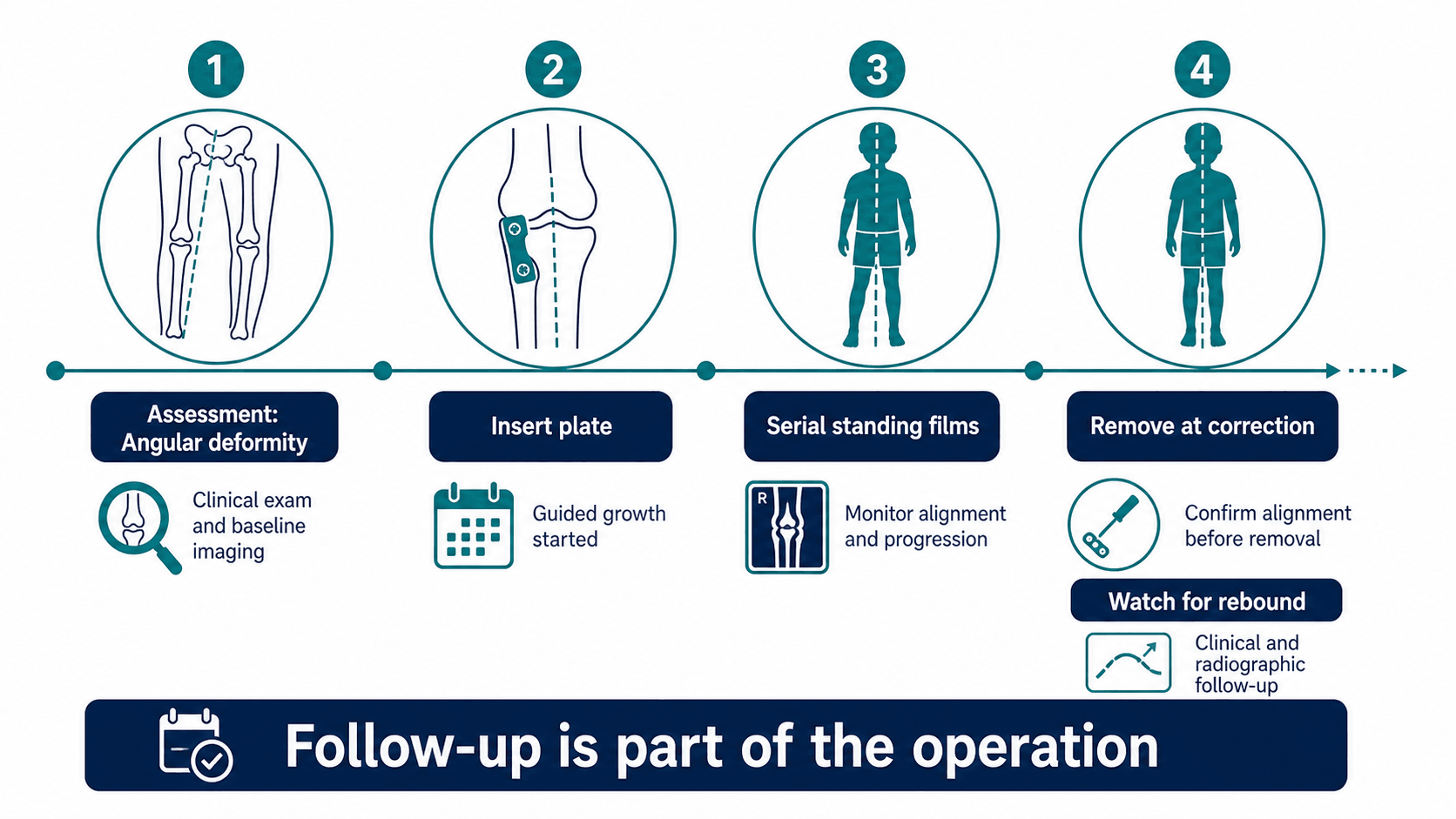
- Correction happens over months and follow-up continues after implant removal because rebound can occur.
- “The implant is small; the analysis is the operation.
- “The mechanical axis tells you where load passes, not why it got there.
- “Treat rickets, Blount disease and physeal bars as specific diagnoses, not as simple knock-knee or bow-leg.
- “Guided growth does not correct rotation, severe joint incongruity or a child who is too close to maturity.
A knee that looks valgus or varus is not enough. Confirm mechanical axis, localise the bone and physis causing deformity, assess growth remaining and identify pathological causes before implanting a plate.
Images and Diagrams

| Question | Answer | Clinical use |
|---|---|---|
| First imaging? | Standing hip-to-ankle radiograph. | Shows global load axis and both limbs. |
| What does MAD show? | How far the mechanical axis is from knee centre. | Quantifies the effect on load transfer. |
| What localises deformity? | LDFA, MPTA and JLCA. | Separates femur, tibia, joint or combined source. |
| What can go wrong after removal? | Rebound, undercorrection or overcorrection. | Follow-up continues after implant removal. |
AXISPlanning Sequence
Hook:AXIS keeps planning grounded in full-length alignment.
PLATEGuided Growth Mechanics
Hook:PLATE links the implant to timing and follow-up.
REBOUNDAfter Removal
Hook:REBOUND makes follow-up after removal explicit.
Overview/Epidemiology
Coronal lower-limb alignment changes normally during childhood. Infants often have genu varum, toddlers pass into genu valgum, and older children gradually settle toward adult alignment. Guided growth is for the child whose alignment is not following that expected pathway or whose deformity is symptomatic, asymmetric, progressive or pathological.
The common clinical problem is genu valgum or genu varum around the knee. The important clinical question is not just whether the knees touch or the ankles separate. The important question is where the mechanical axis passes, what bone creates the deformity, whether the physis is open, how much growth remains, and whether the underlying biology is normal.
Typical indications include persistent genu valgum, pathological genu varum, Blount disease in selected stages, post-traumatic physeal disturbance, skeletal dysplasia and metabolic bone disease after medical optimisation. Guided growth is smaller than osteotomy, but it is not casual. It requires reliable follow-up, timely implant removal and continued surveillance for rebound.
Pathophysiology
Angular deformity develops when growth is asymmetric across a physis or when a bone or joint segment has abnormal orientation. The mechanical axis is the functional consequence: it shows where load passes from the hip to the ankle across the knee. A medial mechanical axis overloads the medial side; a lateral mechanical axis overloads the lateral side.
Guided growth works by temporary hemiepiphysiodesis. A plate, screw construct or other tether slows one side of an open physis. The other side continues to grow, gradually changing the joint orientation and mechanical axis. The correction rate depends on age, remaining growth, which physis is used, the underlying diagnosis and distance from the knee.
Pathological physes behave differently. Blount disease has disordered medial proximal tibial growth and may recur or fail to correct if severe. Rickets and metabolic disease need medical correction before mechanical correction. Post-traumatic physeal bars can create focal angular growth disturbance and may require bar resection, epiphysiodesis or osteotomy rather than a simple plate.
Classification
- Physiological alignment: symmetric, painless, age-appropriate and improving.
- Pathological valgum or varum: persistent, progressive, asymmetric, painful or outside expected developmental range.
- High-risk pattern: lateral thrust, severe obesity, short stature, rickets signs, skeletal dysplasia or prior physeal injury.
- Functional problem: pain, fatigue, patellar symptoms, gait difficulty or sport limitation.
Clinical Presentation
History
Ask about age at onset, progression, symmetry and function. Pain, lateral thrust, fatigue, patellofemoral symptoms and unilateral progression are more concerning than cosmetic concern alone. Ask about previous physeal injury, infection, fracture, metabolic disease, vitamin D risk, renal disease, skeletal dysplasia features, family history and obesity.
Ask the family whether follow-up is practical. Guided growth is a commitment to serial imaging and planned hardware removal.
Examination
Observe the child standing and walking. Look for varus thrust, patellar tracking, foot progression, limb length difference, pelvic level and rotational profile. Measure intercondylar or intermalleolar distance as a clinical baseline, but do not use it as a substitute for full-length alignment.
Assess:
- Hip, knee and ankle range of motion.
- Coronal alignment and patella direction.
- Ligament laxity and joint line opening.
- Lateral thrust in varus knees.
- Rotational profile so torsion is not mistaken for coronal deformity.
- Signs of rickets, skeletal dysplasia or systemic disease.
- Skin, BMI and soft-tissue envelope for implant planning.
A guided-growth plan starts with a standing alignment film and source analysis, not with choosing a plate size.
Investigations
The key investigation is a standing hip-to-ankle radiograph with patellae facing forward where possible. This allows mechanical axis deviation, LDFA, MPTA and joint line convergence to be assessed. A cropped knee film can miss femoral, tibial, limb-length or global alignment contribution.
| Question | Investigation | Decision it informs |
|---|---|---|
| What is the global load axis? | Standing hip-to-ankle radiograph | Measures mechanical axis deviation and bilateral alignment. |
| Where is the deformity? | LDFA, MPTA and JLCA | Localises femur, tibia, joint or combined source. |
| Is enough growth left? | Bone age and maturity assessment | Determines guided-growth feasibility and timing. |
| Is there abnormal biology? | Vitamin D, calcium, phosphate, ALP, renal/endocrine tests when indicated | Optimises metabolic disease before mechanical correction. |
| Is the problem multiplanar? | Sagittal and rotational assessment, CT only when needed | Prevents using coronal guided growth for the wrong problem. |
Differential Diagnosis
- Physiological genu varum or genu valgum.
- Infantile or adolescent Blount disease.
- Nutritional rickets or hypophosphataemic rickets.
- Renal osteodystrophy or endocrine bone disease.
- Post-traumatic physeal bar.
- Skeletal dysplasia.
- Ligamentous laxity or joint line convergence.
- Rotational profile creating apparent coronal malalignment.
- Limb-length difference with pelvic compensation.
Management
| Situation | Best fit | Reasoning |
|---|---|---|
| Symmetric age-appropriate alignment | Observation and explanation | Physiological varus and valgus usually improve without surgery. |
| Metabolic or endocrine bone disease | Medical optimisation first | A plate cannot correct abnormal growth biology if rickets or renal osteodystrophy remains untreated. |
| Open physis, localised coronal deformity, enough growth remaining | Temporary hemiepiphysiodesis | Gradual correction can avoid osteotomy when follow-up and timing are reliable. |
| Severe deformity, joint depression, multiplanar deformity or near maturity | Osteotomy or complex deformity correction | Growth modulation is too slow or too limited for the problem. |
| Post-traumatic physeal bar | MRI or CT mapping, bar resection or epiphysiodesis/osteotomy depending size and growth remaining | The growth arrest is focal and may not be solved by a simple tension-band plate. |
Observe physiological symmetric age-appropriate alignment. Explain natural history and review triggers. Treat metabolic disease before mechanical surgery. In obesity or Blount risk, address modifiable load and assess for lateral thrust, progression and joint depression.
| Step | What the surgeon does | Safety point |
|---|---|---|
| Plan | Mark the mechanical axis, identify the abnormal physis and choose medial or lateral tethering from LDFA, MPTA and JLCA. | Wrong-side or wrong-level tethering is a planning error, not a technical complication. |
| Position and imaging | Supine positioning with fluoroscopy; confirm true AP and lateral views of the target physis. | Poor intra-operative imaging risks screw placement across the physis or wrong plate position. |
| Approach | Small medial or lateral incision centred on the physis, protecting periosteum and soft tissues. | Avoid damaging the physis; the implant should act as a tether, not a physeal bar. |
| Implant | Place tension-band plate, staple or transphyseal screw according to surgeon preference and diagnosis. | Screws should hold epiphysis and metaphysis without crossing into the joint. |
| Follow-up | Serial standing alignment radiographs until target correction, then planned removal. | The operation fails if correction is not tracked or removal is missed. |
| After removal | Continue alignment surveillance for rebound, especially in young children and pathological physes. | Removal is not discharge. |
Complications
Early
- Wrong diagnosis: physiological alignment treated surgically.
- Wrong level or wrong side tethering.
- Infection, wound irritation or hardware prominence.
- No correction because growth remaining is inadequate.
- Family lost to follow-up before planned removal.
Late
- Overcorrection.
- Undercorrection.
- Rebound deformity after removal.
- Hardware breakage or migration.
- Physeal tethering or bar formation.
- Need for repeat guided growth or osteotomy.
Guided growth is not finished in theatre. The correction happens on serial alignment films, and the endpoint is missed if follow-up is missed.
Decision-Making in Practice
Guided growth is a timed growth-modulation operation. It is not an acute correction. The child must have enough growth remaining, the deformity source must be correctly identified, and the family must understand that overcorrection, undercorrection and rebound are surveillance problems.
| Decision | How to decide | Management consequence |
|---|---|---|
| Physiological or pathological | Age, symmetry, progression, pain, height, metabolic disease and family pattern | Physiological alignment is observed; pathological deformity is measured |
| Deformity source | Standing hip-to-ankle film with MAD, LDFA, MPTA and JLCA | Implant the correct side of the correct physis |
| Growth remaining | Bone age, chronological age, pubertal stage and growth velocity | Too little growth means osteotomy may be required |
| Implant choice | Diagnosis, size, physis, surgeon preference and recurrence risk | Tension-band plates, staples or screws have different behaviour |
| Removal timing | Serial axis correction and target overcorrection when appropriate | Prevents overshoot and manages rebound risk |
For genu valgum or varum, treatment begins with the full-length standing film, not a knee-only radiograph. The question is whether deformity arises from distal femur, proximal tibia, both, joint-line obliquity, ligament laxity or extra-articular deformity. Guided growth works poorly if the wrong physis is tethered or if the deformity is mainly intra-articular.
Osteotomy is preferred when correction is urgent, growth remaining is insufficient, deformity is severe and rigid, there is joint depression, or the child is near maturity. Guided growth is preferred when gradual correction is safe, there is enough growth remaining, and the joint surface is acceptable.
Controversies and Areas of Uncertainty
Guided growth is established, but several questions remain genuinely contested and are favourite viva territory.
| Controversy | One view | Counter view |
|---|---|---|
| Deliberate overcorrection | Aim past neutral to offset expected rebound in young, fast correctors. | Overcorrection risks creating the opposite deformity and a second operation; aim for neutral and watch. |
| Implant choice | Tension band plates allow faster, growth-arrest-sparing correction than staples. | Percutaneous transphyseal screws are lower profile and cheaper; staples remain effective in some hands. |
| Leave plate in or remove early | Remove promptly at neutral to avoid overcorrection. | Some retain the plate as a guide during continued growth, accepting closer review. |
| Guided growth in Blount disease | Effective in selected early or mild cases and avoids osteotomy. | High implant breakage and undercorrection in late-onset, high-BMI, severe varus argue for osteotomy. |
| Lower age limit | Earlier intervention uses abundant growth and is gentle. | Very young children rebound more and may simply be physiological; observation may suffice. |
Guidelines, Registries and Global Practice
Guided growth is practised worldwide, but the supporting framework is principle-based and society reviews rather than randomised trials or implant registries, because these are paediatric soft-tissue-sparing procedures in growing bone.
Global epidemiology
- Physiological genu varum is usual in infancy and physiological genu valgum peaks around age 3 to 4 years, settling toward adult alignment (mild valgus) by about age 7, across populations.
- Idiopathic genu valgum needing intervention is uncommon; most referrals are physiological and resolve with observation.
- Blount disease prevalence varies by region and body habitus: infantile (early-onset) disease is more frequent where early walking and higher childhood BMI are common, while late-onset (adolescent) disease tracks adolescent obesity.
- Nutritional rickets remains a leading cause of pathological bowing in limited-resource settings, whereas X-linked hypophosphataemic rickets dominates where nutrition is adequate.
Side-by-side guidance
- Emphasis for paediatric angular deformity
- Distinguish physiological from pathological alignment; image with full-length standing radiographs before any intervention.
- Emphasis for paediatric angular deformity
- Reserve surgery for progressive, asymmetric or pathological deformity; observation and natural-history counselling for physiological alignment.
- Emphasis for paediatric angular deformity
- Deformity analysis (mechanical axis, joint orientation angles, CORA) drives the choice between growth modulation and osteotomy.
- Emphasis for paediatric angular deformity
- Endorse temporary hemiepiphysiodesis as first line for suitable coronal deformity with open physes, with planned removal and rebound surveillance.
The common thread across societies is that the analysis (full-length alignment, source localisation, growth remaining and underlying diagnosis) governs the decision, not the appearance of the knee.
Registry and evidence notes
- There is no dedicated international guided-growth implant registry comparable to arthroplasty registries (NJR, AJRR, AOANJRR); evidence comes from multicentre series such as the multinational tension band plating cohort of 967 physes.
- Best available data are cohort-level (Level III to IV), so counselling rests on pooled series rather than registry survivorship.
High- versus limited-resource practice
- Where full-length standing radiography and reliable follow-up are available, tension band plating with planned removal is standard.
- Where imaging or follow-up is limited, percutaneous transphyseal screws (lower cost, low profile) or single-stage osteotomy may be preferred, because guided growth fails without serial alignment review.
- In settings with high nutritional rickets burden, medical optimisation precedes any mechanical correction, and untreated metabolic disease is a frequent reason guided growth fails.
Evidence Signals
Guided growth principles and indications
- Temporary hemiepiphysiodesis tethers one side of an open physis to allow differential growth and correct coronal deformity around the knee.
- Staples, percutaneous transphyseal screws and tension band plates are all described constructs.
- Undercorrection and overcorrection are common; careful preoperative planning and follow-up minimise complications.
Multinational tension band plating series defines correction rate
- 967 physes in 537 patients across multiple centres; mean age at implantation 11.4 years.
- Calculated correction rate was 0.77 degrees per month for the femur and 0.79 degrees per month for the tibia.
- Infection rate 1.48 percent and screw breakage 0.55 percent; age at implantation and direction of deformity influenced correction.
Tension band plate corrects faster than stapling
- 34 patients with 65 deformities corrected to neutral at a mean of 11 months using a non-locking tension band plate.
- Correction was approximately 30 percent faster than reported with stapling, with no permanent growth arrest.
- Four idiopathic genu valgum patients rebounded and underwent repeat guided growth; two late-onset Blount cases undercorrected.
Clinical Reasoning Notes
Structured clinical approach
Use a structured sequence:
- Define physiological versus pathological alignment.
- Describe symptoms, progression and asymmetry.
- Obtain standing hip-to-ankle films.
- State mechanical axis deviation.
- Use LDFA, MPTA and JLCA to localise source.
- Check growth remaining and bone age.
- Look for metabolic disease, Blount disease or physeal bar.
- Choose observation, medical treatment, guided growth or osteotomy.
- Plan follow-up, removal timing and rebound surveillance.
Common pitfalls
- Planning from a knee-only X-ray.
- Operating on physiological alignment.
- Ignoring bone age.
- Forgetting rickets or renal bone disease.
- Confusing rotational deformity with coronal deformity.
- Using guided growth when osteotomy is required.
- Not removing implants on time.
- Discharging after removal without rebound surveillance.
Evidence Base
Rebound predictors after stapling for genu valgum
- 37 limbs with idiopathic genu valgum followed to maturity or beyond two years after staple removal.
- Rate of correction, BMI, age and initial valgus angle were independent predictors of rebound on multivariate analysis.
- Rapid correctors had a 79 percent rebound incidence (mean 4 degrees); slow correctors with low BMI had less rebound, and none when BMI was at or above 21.
Rebound is common and driven by young age and fast correction
- 100 patients (189 legs) with idiopathic genu valgum analysed on serial long-leg radiographs.
- 59 percent of legs showed rebound growth after plate removal, 30 percent stayed stable and 11 percent continued correcting.
- Sex, age, baseline mechanical axis deviation, mLDFA, mMPTA and the correction rate were significant, with correction rate carrying the highest odds ratio.
Implant breakage is far higher in Blount disease
- 246 tension band implant procedures in 113 patients with Blount disease across 8 centres.
- Overall implant breakage 12 percent (mean 1.6 years after implantation), mostly metaphyseal screws.
- Higher BMI and greater varus deformity raised breakage risk; solid 3.5 mm screws had a 50 percent breakage rate in late-onset Blount disease.
Femoral deformity contributes to malalignment in tibia vara
- 127 limbs with tibia vara reviewed; many had concurrent femoral varus contributing to overall malalignment.
- Femoral lateral tension band plating corrected mLDFA from 98 to 87 degrees, with 80 percent achieving full femoral correction.
- In early-onset tibia vara, 73 percent of femurs corrected with tibial plating alone, supporting observation of the femur in young children.
Physiological alignment and red flags
- Physiological varus and valgus follow a predictable age-related course in young children.
- Pathological features include asymmetry, progression, pain, short stature and systemic disease.
- Treatment depends on diagnosis and growth remaining.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A ten-year-old has progressive genu valgum. How do you plan guided growth?”
“A child with genu varum has lateral thrust and obesity. What are you worried about?”
“An eight-year-old corrected to neutral had her tension band plate removed six months ago. The latest standing film shows the valgus is returning. How do you explain and manage this?”
Measure
- Standing long-leg film
- MAD
- LDFA
- MPTA
- JLCA
- Bone age
Indications
- Progressive
- Asymmetric
- Symptomatic
- Outside age range
- Growth remaining
Treatment
- Observe physiological
- Correct metabolic disease
- Guided growth
- Osteotomy
- Monitor rebound
Pitfalls
- Wrong source
- No follow-up
- Overcorrection
- Rebound
- Rotation ignored