Hook vs Body | Sports Injury | Tendon Rupture Risk | Ulnar Nerve
ANATOMIC CLASSIFICATION
Critical Must-Knows
- Hook forms radial wall of Guyon's canal - ulnar motor branch at risk
- Sports mechanism - golf club, racquet, or bat handle impact to palm
- FDP to ring/small fingers passes over hook - rupture if nonunion
- CT scan required - hook NOT visible on standard radiographs
- Excision of hook nonunion gives excellent outcomes for grip sports
Clinical Pearls
- "Hook of hamate pull test: pain with resisted ring/small finger flexion
- "Carpal tunnel view and 45-degree supinated oblique can show hook
- "Body fractures often associated with 4th/5th CMC fracture-dislocations
- "Pisometacarpal ligament attaches to hook - avulsion mechanism

Critical Exam Points - Hamate Fractures
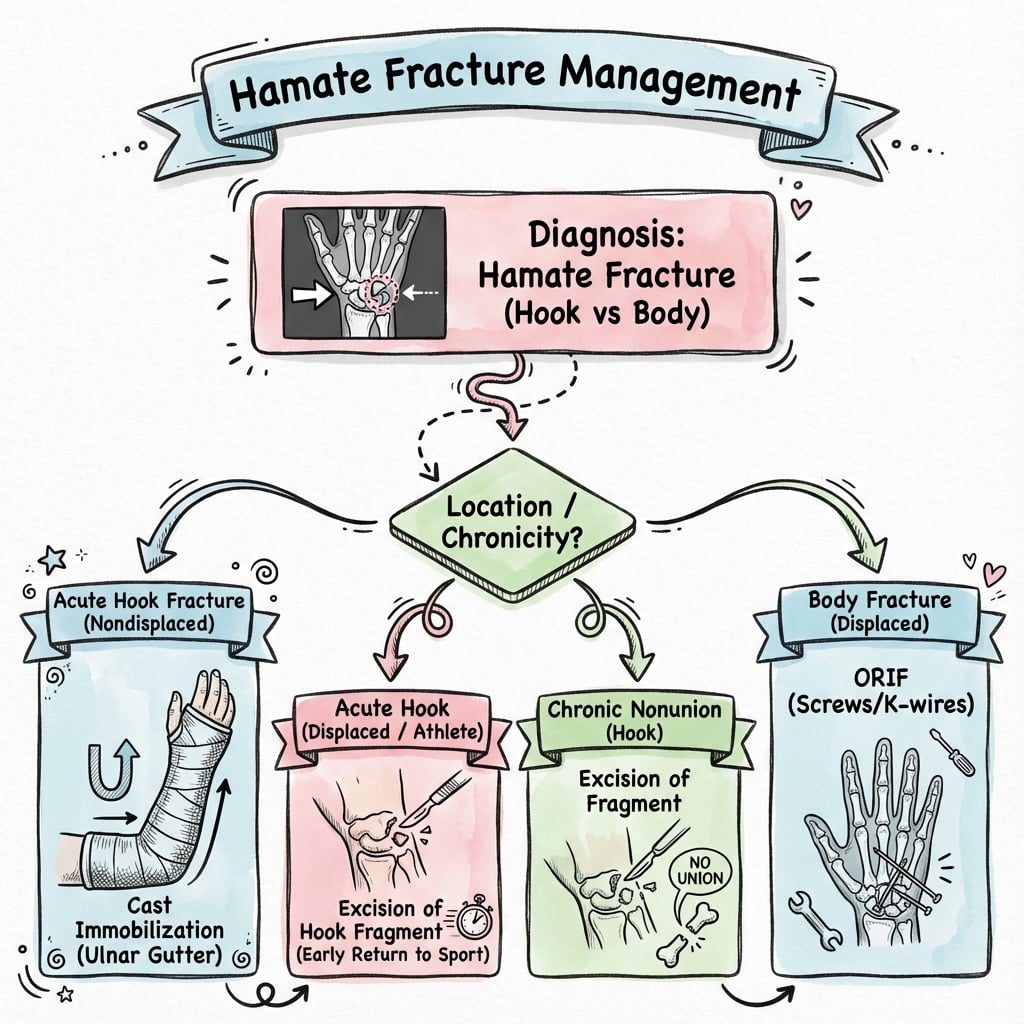
At a Glance - Quick Decision Guide
Acute Hook Fracture
Within 2 weeks of injury:
- CT to confirm diagnosis
- Consider ORIF if base fracture, large fragment
- OR early excision for athletes
- Conservative rarely successful (50% nonunion)
Delayed/Nonunion
Beyond 6 weeks / established nonunion:
- Hook excision is gold standard
- Check FDP integrity pre-op
- Ulnar nerve decompression if symptomatic
- 85-95% return to sport
Body Fracture + CMC
High-energy injury:
- CT for surgical planning
- ORIF via dorsal approach
- Address CMC joint stability
- K-wires or mini screws
Hook vs Body Fracture Comparison
| Feature | Hook Fracture | Body Fracture |
|---|---|---|
| Frequency | 80-90% of hamate fractures | 10-20% of hamate fractures |
| Mechanism | Direct blow from sports equipment handle | High-energy axial load, punch |
| Patient population | Athletes: golf, tennis, baseball | Trauma, altercation (boxer) |
| Key risk | FDP tendon rupture (20%) | CMC joint arthrosis |
| Imaging | CT gold standard (X-ray misses 50%) | Usually visible on X-ray |
| Treatment | Excision for nonunion; ORIF for acute | ORIF with K-wires/screws |
| Return to activity | 6-8 weeks after excision | 8-12 weeks after ORIF |
Memory Aids and Mnemonics
H - A - B - SHamate Fracture Types - 'HABS'
| H | Hook fractures Base, waist, or tip (most common overall - 80%) |
| A | Articular body Coronal split affecting CMC joint |
| B | Body fractures Associated with 4th/5th CMC dislocation |
| S | Stress fractures Rare; repetitive microtrauma in athletes |
| H | Hook fractures Base, waist, or tip (most common overall - 80%) | B | Body fractures Associated with 4th/5th CMC dislocation |
| A | Articular body Coronal split affecting CMC joint | S | Stress fractures Rare; repetitive microtrauma in athletes |
Hook:Hook fractures Are By far the Sport-related injury
B - R - A - GHook of Hamate High-Risk Sports - 'BRAG'
| B | Baseball/Bat sports Handle end impacts palm on swing |
| R | Racquet sports Tennis, squash, badminton racquet impact |
| A | And Golf Most common cause - club grip pressure point |
| G | Gym equipment Weightlifting bars and dumbbell handles |
| B | Baseball/Bat sports Handle end impacts palm on swing | A | And Golf Most common cause - club grip pressure point |
| R | Racquet sports Tennis, squash, badminton racquet impact | G | Gym equipment Weightlifting bars and dumbbell handles |
Hook:Athletes BRAG about their sports but can break their hamate hooks
G - R - I - PHook Examination - 'GRIP'
| G | Grip strength Weak and painful compared to opposite hand |
| R | Resisted flexion test Pain with resisted DIP flexion of ring/small fingers |
| I | Intrinsic muscle power Test first dorsal interosseous and thumb adduction (ulnar nerve) |
| P | Point tenderness 2cm distal and radial to pisiform (hook location) |
| G | Grip strength Weak and painful compared to opposite hand | I | Intrinsic muscle power Test first dorsal interosseous and thumb adduction (ulnar nerve) |
| R | Resisted flexion test Pain with resisted DIP flexion of ring/small fingers | P | Point tenderness 2cm distal and radial to pisiform (hook location) |
Hook:GRIP sports cause hook fractures - test GRIP function
B - L - O - O - DWhy Hook Nonunion is Common - 'BLOOD'
| B | Blood supply poor Tenuous single vessel to hook |
| L | Ligament tension Pisohamate ligament pulls on fragment |
| O | Out of cast Immobilization rarely successful |
| O | Often missed Delayed diagnosis means established nonunion |
| D | Dynamic tendons FDP motion prevents healing |
| B | Blood supply poor Tenuous single vessel to hook | O | Often missed Delayed diagnosis means established nonunion |
| L | Ligament tension Pisohamate ligament pulls on fragment | D | Dynamic tendons FDP motion prevents healing |
| O | Out of cast Immobilization rarely successful |
Hook:Poor BLOOD supply and motion cause nonunion
Overview
Hamate fractures represent 2-4% of all carpal fractures, with the hook of hamate being the most clinically significant injury pattern. The hamate is the most ulnar bone of the distal carpal row and has unique anatomical relationships with the ulnar nerve, flexor tendons, and grip mechanics. Hook fractures are classically associated with racquet sports and golf where the handle impacts the palm.
Key Exam Concept
The hamate hook forms the ulnar border of the carpal tunnel and the radial wall of Guyon's canal. This dual relationship explains why both median nerve (carpal tunnel compression) and ulnar nerve (motor branch palsy) symptoms can occur. The hook also lies adjacent to the FDP tendons to ring and small fingers - rupture occurs in 20% of missed hook fractures.
Epidemiology
- 2-4% of carpal fractures
- Hook fractures: 80-90% of hamate fractures
- Peak incidence: 20-40 years
- Sports-related majority (golf, racquet, bat sports)
- Often delayed diagnosis (weeks to months)
Mechanism
- Hook: Direct blow from sporting equipment handle
- Hook: Avulsion via pisometacarpal ligament
- Body: High-energy axial load
- Body: Dorsal dislocation of 4th/5th CMC joints
- Stress fracture: Repetitive grip activities
Key Clinical Points
- Tenderness 2cm distal and radial to pisiform
- Pain with resisted ring/small finger flexion
- Ulnar nerve motor branch assessment essential
- CT scan is gold standard for hook fractures
- Symptomatic nonunion: hook excision is effective
Delayed Diagnosis - High Complication Rate
Hook of hamate fractures are missed in up to 50% of initial presentations because:
- Standard radiographs often fail to visualize the hook
- Symptoms attributed to "wrist sprain" or "tendinitis"
- Associated injuries distract from hook assessment
Missed fractures lead to:
- Flexor tendon rupture (FDP to ring/small fingers) in 20%
- Ulnar nerve motor branch injury
- Chronic pain and grip weakness
- Nonunion requiring surgical excision
Anatomy and Pathophysiology
Hamate Anatomy Key Points
The hamate is the most ulnar bone of the distal carpal row. It has two main components:
- Body - articulates with capitate (radially), triquetrum (proximally), and 4th/5th metacarpal bases (distally)
- Hook (hamulus) - projects 10-12mm from volar surface, forms important soft tissue attachments
The hook is a volar projection that serves as attachment for three key structures: flexor retinaculum (radial pillar), pisohamate ligament, and pisometacarpal ligament.
Hamate Articulations
Proximal Articulation
- Triquetrum - helicoid joint allowing dart-throwing motion
- Contributes to ulnar column of wrist
- Important for grip strength
Distal Articulations
- 4th metacarpal base - relatively immobile
- 5th metacarpal base - allows 20-30 degrees flexion
- CMC joint motion important for power grip
Neurovascular Relationships
Critical Structures at Risk
Ulnar nerve - motor branch curves around radial aspect of hook
- Injury causes weakness of intrinsic muscles
- Froment sign positive (FPL substitution for thumb adduction)
- First dorsal interosseous weakness impairs key pinch
Ulnar artery - passes superficial in Guyon's canal
- Hook fracture can cause thrombosis or pseudoaneurysm
- Hypothenar hammer syndrome with repetitive trauma
Flexor tendons - FDP to ring and small fingers
- Tendons pass directly over volar aspect of hook
- Sharp fracture edge causes attrition rupture
- 20% incidence of tendon rupture with missed hook fractures
Soft Tissue Attachments
Hook of Hamate Soft Tissue Attachments
| Structure | Attachment Site | Clinical Significance |
|---|---|---|
| Flexor retinaculum | Radial attachment to hook tip | Hook forms radial pillar of carpal tunnel |
| Pisohamate ligament | Proximal aspect of hook | Transmits FCU force; avulsion fracture mechanism |
| Pisometacarpal ligament | Base of hook | Force transmission to 5th metacarpal |
| Opponens digiti minimi | Hook tip and shaft | Origin of hypothenar muscle |
| Flexor digiti minimi | Hook tip | Origin of hypothenar muscle |
| Transverse carpal ligament | Entire hook | Maintains carpal arch |
Blood Supply
Vascularity
The hamate receives blood supply from multiple sources:
- Dorsal carpal arch (dorsal branches)
- Palmar carpal arch (volar branches)
- Direct branches from ulnar artery
The hook has tenuous blood supply - receives single or few nutrient vessels from ulnar artery. This explains the high nonunion rate (up to 50%) with conservative treatment of hook fractures.
Classification
Anatomic Classification
Hook Fractures (80-90%)
- Most common hamate fracture pattern
- Sports-related mechanism (grip sports)
- Direct blow from equipment handle
- Avulsion via pisohamate ligament
- High nonunion rate with conservative Rx
Body Fractures (10-20%)
- High-energy mechanism
- Often with CMC fracture-dislocation
- Articular involvement common
- Require ORIF for joint stability
- Better healing potential than hook
Hamate Fracture Pattern Summary
| Pattern | Mechanism | Associated Injuries | Treatment |
|---|---|---|---|
| Hook - Tip | Flexor retinaculum avulsion | Carpal tunnel symptoms | Immobilization vs excision |
| Hook - Waist | Direct impact (most common) | FDP attrition risk | Excision usually needed |
| Hook - Base | High force impact | Larger fragment | ORIF possible vs excision |
| Body - Dorsal margin | CMC dislocation | 4th/5th CMC subluxation | ORIF + CMC stabilization |
| Body - Coronal split | Axial load | Articular incongruity | ORIF for joint surface |
| Stress fracture | Repetitive microtrauma | Subtle changes on MRI | Rest; excision if symptomatic |
Clinical Assessment
History
Hook Fracture History
- Sports: Golf (most common), tennis, baseball, squash
- Felt "pop" or sharp pain with swing
- Pain worse with gripping
- May have delayed presentation weeks later
- Paresthesias in ring/small fingers (ulnar nerve)
Body Fracture History
- High-energy mechanism (fall, punch, MVC)
- Immediate swelling and deformity
- Often polytrauma setting
- May have associated metacarpal injuries
- Direct blow to dorsum of hand
Physical Examination
Special Tests
Clinical Tests for Hook of Hamate Fractures
| Test | Technique | Positive Finding | Sensitivity |
|---|---|---|---|
| Hook palpation | Press 2cm distal/radial to pisiform | Point tenderness over hook | High if done correctly |
| Pull test | Resist DIP flexion of ring/small fingers | Pain at hook location | ~80% |
| Push test | Patient pushes against table with palm | Pain in hypothenar region | Moderate |
| Grip dynamometry | Compare grip strength bilaterally | Decreased by 20-30% on affected side | Variable |
| Two-point discrimination | Test ring/small finger sensation | Decreased suggests ulnar nerve injury | Low (late finding) |
Ulnar Nerve Assessment is Mandatory
Assess the motor branch of ulnar nerve in all suspected hook fractures:
Motor testing:
- First dorsal interosseous: Index finger abduction against resistance
- Palmar interosseous: Finger adduction (paper grip test)
- Thumb adduction: Froment sign (FPL substitution = positive)
Sensory testing:
- Two-point discrimination of small finger
- Light touch over hypothenar eminence (palmar cutaneous branch)
Wartenberg sign - small finger abduction at rest suggests ulnar nerve palsy
Differential Diagnosis
Differential Diagnosis of Ulnar-Sided Wrist and Hypothenar Pain
| Diagnosis | Distinguishing Features | Key Investigation |
|---|---|---|
| Hook of hamate fracture | Grip-sport mechanism; tenderness 2cm distal/radial to pisiform; pain on resisted ring/small finger flexion | CT (gold standard); X-rays normal in many cases |
| Pisotriquetral arthritis | Tenderness over pisiform; pain on direct pisiform compression and shear | Supinated 30-degree oblique view; CT |
| Triangular fibrocartilage complex (TFCC) tear | Ulnar fovea tenderness; pain on ulnar deviation/loading; positive fovea sign | MR arthrography; wrist arthroscopy |
| Ulnar artery thrombosis (hypothenar hammer syndrome) | Cold intolerance, digital ischaemia; repetitive palmar trauma | Doppler ultrasound; CT/MR angiography; Allen test |
| Guyon canal ulnar neuropathy | Intrinsic weakness/clawing; sensory loss sparing dorsum; Froment sign | Nerve conduction studies; CT/MRI for mass or fracture |
| FCU tendinopathy/calcific tendinitis | Tenderness along FCU at pisiform insertion; pain on resisted flexion-ulnar deviation | Ultrasound; radiograph for calcification |
| Triquetral fracture | Dorsal ulnar tenderness; dorsal chip on lateral X-ray | Lateral and oblique radiographs; CT |
Tendon Assessment
FDP Tendon Integrity
Test FDP function to ring and small fingers at every visit for patients with hook fractures:
- Isolate DIP joint by stabilizing PIP
- Ask patient to flex DIP actively
- Compare strength to contralateral side
- Palpate for tendon continuity at wrist
Rupture of FDP (especially to small finger) is a late complication of missed hook fractures. If rupture occurs, tendon grafting or transfer may be required.
Investigations
Radiographic Views
Standard Views
- PA view: body visible, hook often obscured
- Lateral: limited hook visualization
- Miss rate up to 50% for hook fractures
- Obtain if suspected clinically
Specialized Views
- Carpal tunnel view: wrist dorsiflexed, beam parallel to palm
- 45° supinated oblique: hook profiled
- Lateral with supination: improves hook visibility
- More sensitive but still miss fractures
When to Get CT
- Clinical suspicion despite negative X-rays
- Preoperative planning for ORIF
- Evaluate union after conservative treatment
- Gold standard for hook fractures


CT Imaging Protocol
CT Scan Technique
CT is the gold standard for hook of hamate fractures:
- 1mm axial slices through carpus
- Sagittal and coronal reconstructions
- Compare to contralateral side if needed
CT findings:
- Fracture line through hook (any location)
- Displacement and fragment size
- Nonunion signs (sclerosis, gap, cyst formation)
- Associated body fractures



MRI Indications
Imaging Modality Comparison
| Modality | Sensitivity for Hook | Best Use | Limitations |
|---|---|---|---|
| Standard X-ray | 50% | Initial screening | Hook often not visible |
| Carpal tunnel view | 70% | Clinical suspicion | Positioning dependent |
| CT scan | 95-100% | Definitive diagnosis; surgical planning | Radiation; cost |
| MRI | 90% | Stress fractures; soft tissue | Cost; availability |
Imaging Approach
Clinical Algorithm:
- Suspicion based on history/exam → Standard X-rays first
- If negative but high clinical suspicion → CT scan (do not delay)
- MRI reserved for: occult stress fractures, soft tissue assessment, or tendon evaluation
- Ultrasound can identify tendon ruptures if concern
Do NOT rely on normal X-rays to exclude hook fractures in a patient with classic presentation!
Management
Non-operative Treatment
Indications for Conservative
- Acute non-displaced hook tip fractures
- Very early presentation (within days)
- Patient preference for trial of immobilization
- Low-demand patients
- Stress fractures caught early
Protocol
- Short arm cast or thermoplastic splint
- 6-8 weeks immobilization minimum
- Avoid gripping activities
- Serial CT to assess union
- High failure rate: up to 50% nonunion
Conservative Treatment Reality
Conservative treatment for hook fractures has a high failure rate due to:
- Tenuous blood supply to hook
- Tensile forces from pisohamate ligament
- Motion from adjacent flexor tendons
- Delayed presentations are already nonunions
Most sports medicine surgeons recommend early excision for athletes who need to return to grip sports, citing predictable outcomes and faster recovery.
Surgical Technique
Hook of Hamate Excision
Patient Positioning:
- Supine with arm on hand table
- Tourniquet on upper arm
- Wrist in neutral, fingers slightly flexed
Surgical Approach:
- Incision: Curvilinear incision over hypothenar eminence
- Identify landmarks: Pisiform proximally, hook palpable distally
- Protect ulnar nerve: Motor branch courses radial to hook
- Expose hook: Incise hypothenar fascia, retract muscles
Excision Steps:
- Clear soft tissue from hook circumferentially
- Use curved osteotome at hook base
- Direct osteotome toward palm (away from tendons)
- Remove entire hook as single fragment
- Smooth residual base with rongeur/burr
- Inspect FDP tendons for damage
- Check ulnar nerve integrity
Closure:
- Repair hypothenar fascia
- Close skin with interrupted sutures
- Soft dressing, immediate finger motion allowed
Early finger motion is key to preventing stiffness and optimizing tendon gliding.
Surgical Pearls
Hook Excision Pearls
- Mark pisiform before incision (landmark)
- Stay ulnar to protect motor branch
- Remove ENTIRE hook to prevent symptoms
- Smooth base to prevent tendon irritation
- Check FDP tendons intraoperatively
Body ORIF Pearls
- True lateral view essential for CMC reduction
- Address all associated metacarpal fractures
- Stable fixation allows early motion
- K-wires removed at 6 weeks
- Watch for extensor lag post-op

Complications
Flexor Tendon Rupture
FDP rupture to ring or small finger is the most devastating complication of missed hook fractures:
- Occurs in 20% of untreated nonunions
- Sharp fracture edge causes attrition over weeks to months
- Small finger FDP most commonly affected
- Patient notices inability to flex DIP joint
Treatment of tendon rupture:
- If rupture is acute: tendon repair if ends can be approximated
- Most cases require: tendon grafting or FDS-to-FDP transfer
- Outcomes not as good as intact tendon
Early Complications
- Nonunion - up to 50% with conservative treatment
- Ulnar nerve injury - motor branch palsy
- Ulnar artery thrombosis
- Infection (if open injury)
- Complex regional pain syndrome
Late Complications
- FDP tendon rupture - 20% of nonunions
- Chronic pain and grip weakness
- Ulnar neuropathy (chronic compression)
- CMC arthrosis (body fractures)
- Hypothenar atrophy
Ulnar Nerve Complications
Ulnar Nerve Injury Patterns in Hamate Fractures
| Zone | Affected Structures | Clinical Finding | Prognosis |
|---|---|---|---|
| Zone I (proximal Guyon) | Superficial and deep branches | Sensory + motor loss | May need decompression |
| Zone II (around hook) | Deep motor branch only | Motor weakness, no sensory loss | Most common; usually recovers |
| Zone III (distal) | Superficial sensory only | Sensory loss only | Rare with hamate fractures |
| Compression by nonunion | Variable | Progressive weakness | Excision usually curative |
Differentiating Ulnar Nerve Zones
Zone II injury (deep motor branch around hook) is most common with hamate fractures:
- NO sensory loss - sensory branch takes separate course
- Weakness of interossei and hypothenar muscles
- Froment sign positive (FPL substitution for adductor pollicis weakness)
- First dorsal interosseous atrophy visible
- Usually improves after hook excision and decompression
Grip Strength Considerations
Post-Excision Grip Strength
Concern exists that hook excision will weaken grip. Evidence shows:
- Grip strength averages 80-90% of contralateral after excision
- No significant difference in hook excision vs ORIF for athletes
- Larger handle diameter compensates for any weakness
- Return to elite golf and racquet sports documented
- Patient satisfaction high despite measurable decrease
Bottom line: Grip strength reduction is minimal and well-tolerated, especially compared to ongoing pain or tendon rupture risk with nonunion.
Postoperative Care
Post-Excision Protocol
- Soft bulky dressing, not cast
- Immediate finger ROM encouraged
- Elevation and edema control
- Wound check at 10-14 days
- Suture removal at 2 weeks
- Full active wrist ROM begins
- Light grip strengthening with putty
- Scar massage and desensitization
- Protective padding for sport activities
- Avoid heavy gripping
- Sport-specific grip exercises
- Gradual return to equipment use
- Modified grip diameter (larger handle)
- Progressive resistance training
- Monitor for tendon symptoms
- Full sport participation
- May use grip modification initially
- Protective padding optional
- Grip strength typically 80-90% of contralateral
- Follow up PRN
Rehabilitation Pearls
Hook Excision Rehab
- Early motion is key - no casting needed
- Grip strengthening begins at 2 weeks
- Sport-specific training at 4-6 weeks
- Larger grip handles compensate for weakness
- Full competition by 6-8 weeks
Body ORIF Rehab
- Protect fixation for 6 weeks
- CMC joint stability is priority
- Hand therapy essential for ROM
- Expect 3 months to full activity
- Monitor for CMC stiffness
Outcomes and Prognosis
Hook Fracture Outcomes
Hook Fracture Treatment Outcomes
| Treatment | Union Rate | Return to Sport | Grip Strength | Satisfaction |
|---|---|---|---|---|
| Conservative (casting) | 50% | Variable (if heals) | Variable | Low (frequent nonunion) |
| Hook excision | N/A (removed) | 6-8 weeks | 80-90% contralateral | High (85-95%) |
| Hook ORIF (acute) | 75-85% | 10-12 weeks | 90-95% if heals | Moderate (may need revision) |
Hook Excision - The Athlete's Choice
For athletes requiring reliable return to grip sports:
- Excision is preferred over conservative treatment or ORIF
- Predictable timeline (6-8 weeks to full sport)
- No risk of nonunion (hook is removed)
- Grip strength acceptably preserved (80-90%)
- Can return to elite level golf, tennis, baseball
ORIF considerations:
- May offer slightly better grip strength if union achieved
- But: 15-25% require excision anyway due to nonunion
- Longer rehabilitation period
- Reserved for select acute cases with large fragments
Body Fracture Outcomes
Good Prognostic Factors
- Anatomic reduction achieved
- Stable fixation obtained
- Early presentation
- Isolated injury (no CMC dislocation)
- Good patient compliance
Poor Prognostic Factors
- Articular comminution
- Associated CMC dislocation
- Delay to treatment
- Polytrauma patient
- Tobacco use
Long-term Considerations
Long-term Follow-up
After Hook Excision:
- Most patients have no long-term issues
- Grip strength stabilizes by 3-6 months
- Rare: hypothenar weakness if motor branch injured
- Very rare: recurrent symptoms (usually from incomplete excision)
After Body ORIF:
- CMC arthrosis may develop over 10-20 years
- More likely with comminution or residual incongruity
- Usually manageable with activity modification
- CMC arthrodesis rarely needed
Evidence Base
Return to Play After Hook of Hamate Fracture (Meta-analysis)
- PRISMA systematic review and meta-analysis of 20 studies (823 athletes). 94.5% (778/823) returned to play, and 91.2% returned at similar or improved performance. Mean time to return to play was 45 days (range 21-168). Surgical excision was used in 95.6% of patients, open reduction and internal fixation (ORIF) in 2.2%, and casting in 1.6%.
Surgical Management: ORIF versus Excision (Systematic Review)
- Systematic review of 27 studies (1954-2023) comparing excision (n=779) with ORIF (n=51). Excision gave a shorter return to sport (6 vs 7.8 weeks) and lower rates of persistent pain (6.1% vs 33.3%), but slightly higher rates of ulnar nerve sensory (4.2% vs 0%) and motor (1.5% vs 0%) dysfunction. Chronic fractures had a longer return to sport than acute injuries (7.2 vs 5.7 weeks).
CT versus Conventional Radiography for Hamate Fractures
- Cadaveric study (18 hands) with controlled hamate fractures imaged by all conventional projections (AP, lateral, oblique, carpal tunnel view) versus high-resolution CT. Combined radiographic sensitivity was only 72.2% (specificity 88.8%, accuracy 80.5%), whereas CT sensitivity was 100% (specificity 94.4%, accuracy 97.2%). Axial or sagittal CT planes were optimal.
Critical Evaluation of Therapeutic Procedures
- Series of 14 hook of hamate fractures. Five of six conservatively treated fractures progressed to symptomatic nonunion, whereas all eight patients treated by primary surgery (excision or screw fixation) were asymptomatic by three months. Primary surgical success (8/8) was significantly higher than conservative treatment (1/6); excision and ORIF gave comparable results.
Excision in Competitive Golfers
- Seven competitive golfers with isolated hook of hamate fractures treated by excision. All had complete resolution of pain and all returned to their previous level of play, supporting an overuse/repetitive-motion mechanism in this group.
Viva Scenarios
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Acute Hook of Hamate in Golfer
"A 35-year-old right-hand dominant professional golfer presents with 2 weeks of ulnar-sided wrist pain after feeling a 'pop' during a swing. He has point tenderness 2cm distal to the pisiform and pain with gripping. X-rays are normal. What is your approach?"
Chronic Hook Nonunion with Tendon Concerns
"A 28-year-old tennis player presents with 4 months of hypothenar pain and now notices weakness flexing her small finger. She was previously told she had a 'wrist sprain.' CT shows hook of hamate nonunion with sclerotic margins. What are your concerns and how would you manage this?"
High-Energy Hamate Body Fracture
"A 40-year-old punches a wall and presents with dorsal hand swelling and unable to make a fist. X-rays show a fracture through the hamate body with dorsal subluxation of the 5th CMC joint. Describe the injury pattern and your management."
MCQ Practice Points
High-Yield MCQ Facts
- Hook forms radial wall of Guyon's canal (ulnar nerve at risk)
- Hook also forms ulnar border of carpal tunnel (median nerve)
- CT sensitivity 95-100% vs X-ray sensitivity 50%
- 50% nonunion rate with conservative treatment
- 20% FDP rupture rate with untreated nonunion
Common MCQ Traps
- Hook is radial to pisiform, not ulnar (2cm distal and radial)
- Motor branch of ulnar nerve at risk, NOT sensory
- X-rays are often normal with hook fractures
- Body fractures need ORIF, hook fractures often need excision
- Grip sports (golf, tennis) cause hook, not body fractures
Sample MCQ Concepts
Key Differentiators for MCQs
| Question Type | Key Point to Remember |
|---|---|
| Best imaging for hook fracture? | CT scan (gold standard) - X-rays miss 50% |
| Treatment for symptomatic nonunion? | Hook excision - not conservative, not ORIF |
| Which nerve branch at risk? | Motor branch of ulnar nerve (Zone II - around hook) |
| Return to sport timeline? | 6-8 weeks after excision |
| Most common mechanism? | Direct blow from sports equipment (golf club) |
| Tendon at risk for rupture? | FDP to ring and small fingers |
| Location of hook tenderness? | 2cm distal AND RADIAL to pisiform |
Imaging Question
Q: A golfer presents with hypothenar pain after hitting the ground during a swing. Plain radiographs are normal. What is the best next investigation?
A: CT scan of the wrist. Hook of hamate fractures are notoriously difficult to visualize on plain radiographs (50% sensitivity). CT has 95-100% sensitivity for hook fractures and is the gold standard imaging modality.
Anatomy Question
Q: Which neural structure passes through Guyon's canal and is most at risk with hook of hamate fractures?
A: The motor branch of the ulnar nerve (deep branch). The hook of hamate forms the radial wall of Guyon's canal. Injury causes weakness of intrinsic muscles (interossei, hypothenar muscles) without sensory loss in Zone II injuries.
Treatment Question
Q: A baseball player presents 6 weeks after injury with persistent hypothenar pain. CT confirms hook of hamate nonunion. What is the recommended treatment?
A: Hook excision. Hook of hamate nonunion has a 50% rate with conservative management. Excision reliably resolves symptoms with excellent outcomes, allows return to sport in 6-8 weeks, and eliminates the risk of FDP tendon rupture from the sharp nonunion fragment.
Complication Question
Q: What tendon is at risk of rupture with an untreated hook of hamate fracture, and what is the reported rupture rate?
A: The flexor digitorum profundus (FDP) tendons to the ring and small fingers are at risk due to their close proximity to the hook. Untreated nonunion has a 20% FDP rupture rate due to attrition from the sharp fracture fragment.
Classification Question
Q: What distinguishes hook of hamate fractures from body of hamate fractures in terms of mechanism and treatment?
A: Hook fractures result from direct impact during grip sports (golf, baseball) and are often treated with excision if symptomatic or nonunion develops. Body fractures result from high-energy trauma, often with associated CMC injuries, and require ORIF to restore carpometacarpal articulation.
Clinical Examination Question
Q: Where is the hook of hamate palpated on clinical examination?
A: The hook is palpated 2cm distal AND radial to the pisiform. It forms the ulnar border of the carpal tunnel and the radial wall of Guyon's canal. Point tenderness at this location with grip weakness is highly suggestive of hook fracture.
Guidelines, Registries & Global Practice
Global Epidemiology
Incidence and Demographics
- Hamate fractures: 2-4% of carpal fractures (hook predominates)
- Strongly male, peak age 20-40 years
- Hook fractures cluster in grip/racquet sports: golf, baseball/softball, tennis, squash, hockey, and (regionally) underwater rugby
- Body fractures arise from high-energy axial load with 4th/5th CMC fracture-dislocation
- Diagnosis is frequently delayed, with many presentations as established nonunion
Evidence-Based Practice Signals
- Cadaveric study: combined radiographic sensitivity 72.2% vs CT 100% (Andresen 1999, PMID 9888053)
- Meta-analysis of 823 athletes: 94.5% return to play, mean 45 days, 95.6% treated by excision (Luxenburg 2024, PMID 38419427)
- Systematic review: excision gives faster return (6 vs 7.8 weeks) and less residual pain (6.1% vs 33.3%) than ORIF (Donohue 2023, PMID 38903831)
Guidance and Society Positions
No major orthopaedic body (AAOS, BOA/BSSH, NICE, AO Foundation, EFORT) publishes a disease-specific clinical practice guideline dedicated to hamate fractures; management is guided by hand-surgery consensus and the systematic-review evidence below. There is no carpal-fracture-specific national joint registry (the AOANJRR/NJR/AJRR cover arthroplasty, not carpal trauma), so registry-level outcome data are not available for this injury.
Where the Evidence and Practice Converge Internationally
| Domain | Consensus Position | Evidence Level |
|---|---|---|
| First-line imaging | CT is the modality of choice; radiographs (including carpal tunnel view) cannot exclude a hook fracture | Level II cadaveric (PMID 9888053) |
| Symptomatic nonunion | Surgical management (most commonly excision) is recommended over continued immobilisation | Level IV series (PMID 15692355) |
| Athlete, return-to-sport priority | Excision favoured for predictable, rapid return | Level III review/meta-analysis (PMID 38903831, 38419427) |
| Acute, large basal fragment | ORIF is a reasonable alternative with comparable outcomes in selected cases | Level III-IV (PMID 38903831, 15692355) |
| Displaced body fracture / CMC dislocation | ORIF to restore carpometacarpal congruity and stability | Level IV expert/series |
Practice Variation
Excision vs ORIF
- Worldwide literature is dominated by excision (over 95% of pooled surgical cases)
- ORIF remains operator- and region-dependent, used selectively for acute basal fragments
- No high-level trial establishes superiority of either - the main systematic review explicitly calls for a prospective cohort with standardised outcomes
Access and Recognition
- Outcomes hinge on timely CT access and clinician awareness, both of which vary by health system
- Delayed diagnosis (and thus nonunion and FDP rupture risk) is more frequent where advanced imaging is rationed or the diagnosis is unfamiliar
- High suspicion in grip-sport athletes with hypothenar pain is the key cross-system safeguard
Exam Framing
In any global fellowship exam, be ready to:
- Justify CT as first-line when suspicion is high despite normal radiographs
- Describe hook excision technique and ulnar motor branch protection
- Quote the return-to-sport evidence (around 94% RTP, mean 45 days, mostly after excision)
- Recognise the delayed-presentation/nonunion pattern and the 20% FDP rupture risk it carries
Hamate Fractures - Exam Day Essentials
Clinical summary
Anatomy Points
- •Hook = radial wall of Guyon's canal + ulnar pillar of carpal tunnel
- •Motor branch of ulnar nerve curves around hook - intrinsic weakness if injured
- •FDP to ring and small fingers pass over hook - rupture risk 20% if nonunion
- •Pisohamate ligament attaches proximally - transmits FCU force
Clinical Keys
- •Hook tenderness: 2cm distal and RADIAL to pisiform (not ulnar)
- •Pull test: resisted DIP flexion of ring/small fingers causes hook pain
- •Test FDP function at every visit - rupture is late complication
- •Ulnar motor testing: 1st dorsal interosseous and thumb adduction
Imaging
- •Standard X-rays miss 50% of hook fractures - carpal tunnel view better
- •CT is GOLD STANDARD - 100% sensitivity, get if clinical suspicion
- •MRI for stress fractures or occult injuries
- •Nonunion on CT: sclerotic margins, gap, cyst formation
Hook Treatment
- •Conservative: 50% nonunion rate - reserved for acute, non-displaced only
- •Excision: gold standard for symptomatic nonunion, 85-95% return to sport
- •ORIF: option for acute base fractures, 75-85% union rate
- •Return to grip sports: 6-8 weeks after excision
Body Treatment
- •ORIF required for displaced body fractures
- •Address CMC joint stability (often associated fracture-dislocation)
- •K-wires or mini screws depending on fragment size
- •Watch for long-term CMC arthrosis
Complications to Know
- •FDP rupture - 20% of nonunions, small finger most common
- •Ulnar motor branch injury - Zone II (around hook) most common
- •Nonunion - 50% with conservative treatment of hook fractures
- •Grip weakness after excision - 80-90% of contralateral (well tolerated)