PIPJ Flexion Deformity
Lesser Toe Deformity Types
Critical Must-Knows
- Hammer Toe: PIPJ flexion with neutral DIPJ and MTPJ - most common lesser toe deformity.
- Claw Toe: MTPJ hyperextension with PIPJ AND DIPJ flexion - often neurological cause.
- Mallet Toe: Isolated DIPJ flexion only - least common, affects terminal tendon.
- Flexible vs Rigid: Correctable with ankle plantarflexed (FDL relaxed) = flexible.
- Flexibility Test: Critical - determines soft tissue vs bone surgery.
Clinical Pearls
- "Plantarflex ankle to test flexibility (relaxes FDL)
- "Always assess MTPJ stability - Drawer test
- "Flexible = FDL tenotomy/transfer
- "Rigid = PIPJ arthroplasty or arthrodesis
- "Address MTPJ if subluxed (Weil osteotomy)
Flexibility is the Key Exam Finding
The flexibility test determines your entire surgical approach.
- Flexible: Correct PIPJ with ankle PLANTARFLEXED (this relaxes FDL).
- If it corrects = Flexible → Soft tissue surgery (FDL tenotomy or transfer).
- If fixed = Rigid → Bone surgery (PIPJ arthroplasty or arthrodesis).
- Always check MTPJ - subluxation needs Weil osteotomy.
- Drawer test - anterior draw of proximal phalanx indicates MTPJ instability.
Hammer vs Claw vs Mallet Deformity
| Feature | Hammer Toe | Claw Toe | Mallet Toe |
|---|---|---|---|
| Neutral/Extended | HYPEREXTENDED | Neutral | |
| FLEXED | FLEXED | Neutral | |
| Neutral | FLEXED | FLEXED | |
| 80% of lesser toe | 15% of lesser toe | 5% of lesser toe | |
| Shoe wear, hallux valgus | Neurological (CMT, DM) | Trauma, long 2nd toe | |
| FDL/FDB overpull | Intrinsic weakness | FDP/terminal tendon |
Flexible Hammer
Rigid Hammer
MTPJ Subluxation
Crossover Toe
At a Glance
Hammer toe is the most common lesser toe deformity, characterized by PIPJ flexion with neutral DIPJ and MTPJ, affecting the 2nd toe in 80% of cases due to hallux valgus pressure and intrinsic muscle imbalance. The flexibility test (plantarflex ankle to relax FDL) is the critical examination determining surgical approach: flexible deformities respond to soft tissue procedures (FDL tenotomy, Girdlestone-Taylor transfer), while rigid deformities require bone surgery (PIPJ arthroplasty or arthrodesis). Always assess MTPJ stability with drawer test, as subluxation requires concurrent Weil osteotomy. Surgical correction achieves 80-90% good outcomes with proper deformity classification and procedure selection.
HCMDeformity Types - HCM
| H | Hammer PIPJ flexion (PIP joint only) |
| C | Claw MTP extension + PIP/DIP flexion (all joints) |
| M | Mallet DIPJ flexion only (DIP joint only) |
| H | Hammer PIPJ flexion (PIP joint only) |
| C | Claw MTP extension + PIP/DIP flexion (all joints) |
| M | Mallet DIPJ flexion only (DIP joint only) |
Hook:HCM - Hammer at PIP, Claw everywhere (neurological), Mallet at DIP (terminal)
PLANTFlexibility Test - PLANT
| P | Plantarflex Plantarflex ankle |
| L | Lax Makes FDL lax |
| A | Assess Assess PIPJ correction |
| N | No Resistance No resistance = flexible |
| T | Treatment Guided Treatment determined by result |
| P | Plantarflex Plantarflex ankle | N | No Resistance No resistance = flexible |
| L | Lax Makes FDL lax | T | Treatment Guided Treatment determined by result |
| A | Assess Assess PIPJ correction |
Hook:PLANT the ankle down to test flexibility - if it corrects with FDL lax, it's flexible.
FRASurgical Options - FRA
| F | Flexible = FDL Flexible: FDL tenotomy or transfer |
| R | Rigid = Resection Rigid: PIPJ resection arthroplasty |
| A | Arthrodesis Alternative Or PIPJ fusion for stability |
| F | Flexible = FDL Flexible: FDL tenotomy or transfer |
| R | Rigid = Resection Rigid: PIPJ resection arthroplasty |
| A | Arthrodesis Alternative Or PIPJ fusion for stability |
Hook:FRA - Flexible gets FDL surgery, Rigid needs Arthroplasty/Arthrodesis.
FIRSComplications - FIRS
| F | Floating Floating toe (floppy, no purchase) |
| I | Infection K-wire infection |
| R | Recurrence Recurrent deformity |
| S | Stiffness PIPJ stiffness post-arthrodesis |
| F | Floating Floating toe (floppy, no purchase) | R | Recurrence Recurrent deformity |
| I | Infection K-wire infection | S | Stiffness PIPJ stiffness post-arthrodesis |
Hook:FIRS - Floating toe is the most common complaint post hammer toe surgery.
Overview and Epidemiology
Hammer Toe is the most common lesser toe deformity, accounting for approximately 80% of all lesser toe pathology. It predominantly affects the 2nd toe due to its length (often longest ray) and relationship with hallux valgus.
Epidemiology
- Prevalence: 2-20% of adult population
- Gender: Women affected 4-5x more than men (footwear)
- Age: Peak 40-60 years
- Location: 2nd toe in 80% of cases
- Bilateral: 40% have bilateral involvement
Pathophysiology and Anatomy
Anatomy
- PIPJ: Proximal interphalangeal joint - site of primary deformity
- Flexors: FDL (flexor digitorum longus), FDB (flexor digitorum brevis)
- Extensors: EDL (extensor digitorum longus), EDB (extensor digitorum brevis)
- Intrinsics: Interossei, lumbricals - flex MTPJ, extend IPJs
Pathophysiology
- Muscle Imbalance: FDL/FDB overpull relative to extensors
- Intrinsic Weakness: Loss of intrinsic function → PIPJ flexion
- Shoe Wear: Tight toe box → toe flexion adaptation
- Hallux Valgus: 2nd toe crowded, forced to flex
- Inflammatory Arthritis: Joint destruction, subluxation
Aetiology
- Footwear: High heels, narrow toe box - most common
- Hallux Valgus: Associated in 50-75% of cases
- Long 2nd Metatarsal: Increased pressure
- Inflammatory Arthritis: RA, psoriatic
- Neurological: Diabetic neuropathy, CMT, CVA (usually claw)
- Trauma: Compartment syndrome, crush injury
Clinical Assessment
History
- Pain: Dorsal PIPJ (shoe rubbing), tip of toe, under metatarsal head
- Callus/Corn: Dorsal PIPJ, tip of toe, interdigital
- Cosmesis: Crooked toe appearance
- Shoe Wear: Difficulty finding comfortable shoes
- Progression: Initially flexible → becomes rigid over time
- Hallux: Associated bunion symptoms
Physical Examination
Examination Technique
-
Standing Assessment
- Observe toe position weight-bearing
- Check for associated hallux valgus
- Assess arch, hindfoot alignment
-
Seated Examination
- Flexibility Test: Most critical exam finding
- Plantarflex ankle (relaxes FDL)
- Attempt to correct PIPJ deformity
- If corrects = Flexible
- If fixed = Rigid
- Flexibility Test: Most critical exam finding
-
MTPJ Assessment
- Drawer Test: Grasp toe, attempt to sublux proximally
- Positive = MTPJ instability (plantar plate injury)
- Assess MTPJ ROM
-
Callus/Skin
- Dorsal PIPJ: From shoe pressure
- Tip of toe: From ground contact
- Interdigital: From adjacent toe pressure
-
Neurovascular
- Capillary refill
- Sensation (diabetic neuropathy common)
Classification Systems
Coughlin Classification - Lesser Toe Deformities:
- Type I: Flexible deformity, reducible
- Type II: Semi-rigid, partially reducible
- Type III: Rigid, fixed deformity
- Type IV: Rigid with MTPJ subluxation/dislocation
Dhukaram Classification:
- Grade 1: Flexible, correctable
- Grade 2: Rigid PIPJ, flexible MTPJ
- Grade 3: Rigid PIPJ and MTPJ
- Grade 4: With MTPJ dislocation
Differential Diagnosis
Distinguishing the Painful Lesser Toe
| Condition | Key Deformity / Sign | Distinguishing Feature |
|---|---|---|
| Hammer toe | PIPJ flexion, neutral MTPJ/DIPJ | Flexibility test guides treatment; dorsal PIPJ corn |
| Claw toe | MTPJ extension + PIPJ/DIPJ flexion | Usually multiple toes; look for neurological cause (CMT, diabetes) |
| Mallet toe | Isolated DIPJ flexion | Tip-of-toe corn; terminal tendon pathology |
| Crossover 2nd toe | Medial/dorsal drift over hallux | Plantar plate tear, positive drawer; precedes fixed deformity |
| Plantar plate insufficiency | Dorsal MTPJ subluxation | Positive drawer/squeeze; pain at plantar MTPJ rather than PIPJ |
| Freiberg infraction | MTPJ pain, flattened metatarsal head | AVN of metatarsal head on X-ray; joint-line tenderness, not PIPJ |
| Morton neuroma | Interdigital pain, Mulder click | No fixed osseous deformity; numbness in adjacent toes |
Investigations
Imaging
Weight-Bearing Radiographs:
- AP View: MTPJ alignment, subluxation, joint space
- Oblique View: PIPJ deformity, osteophytes
- Lateral View: Degree of flexion, PIPJ arthritis
Radiographic Assessment
- MTPJ subluxation (proximal phalanx displaced dorsally)
- PIPJ joint destruction/arthritis
- Associated hallux valgus angle
- Metatarsal length assessment
- Bone quality (inflammatory arthritis)
Special Investigations
- HbA1c: If diabetic neuropathy suspected
- Inflammatory Markers: ESR, CRP if inflammatory arthritis
- Nerve Conduction Studies: If neurological cause suspected (CMT)
Clinical Pearl
Weight-bearing X-rays are essential - non-weight-bearing images miss MTPJ subluxation and underestimate deformity severity.
Management Algorithm
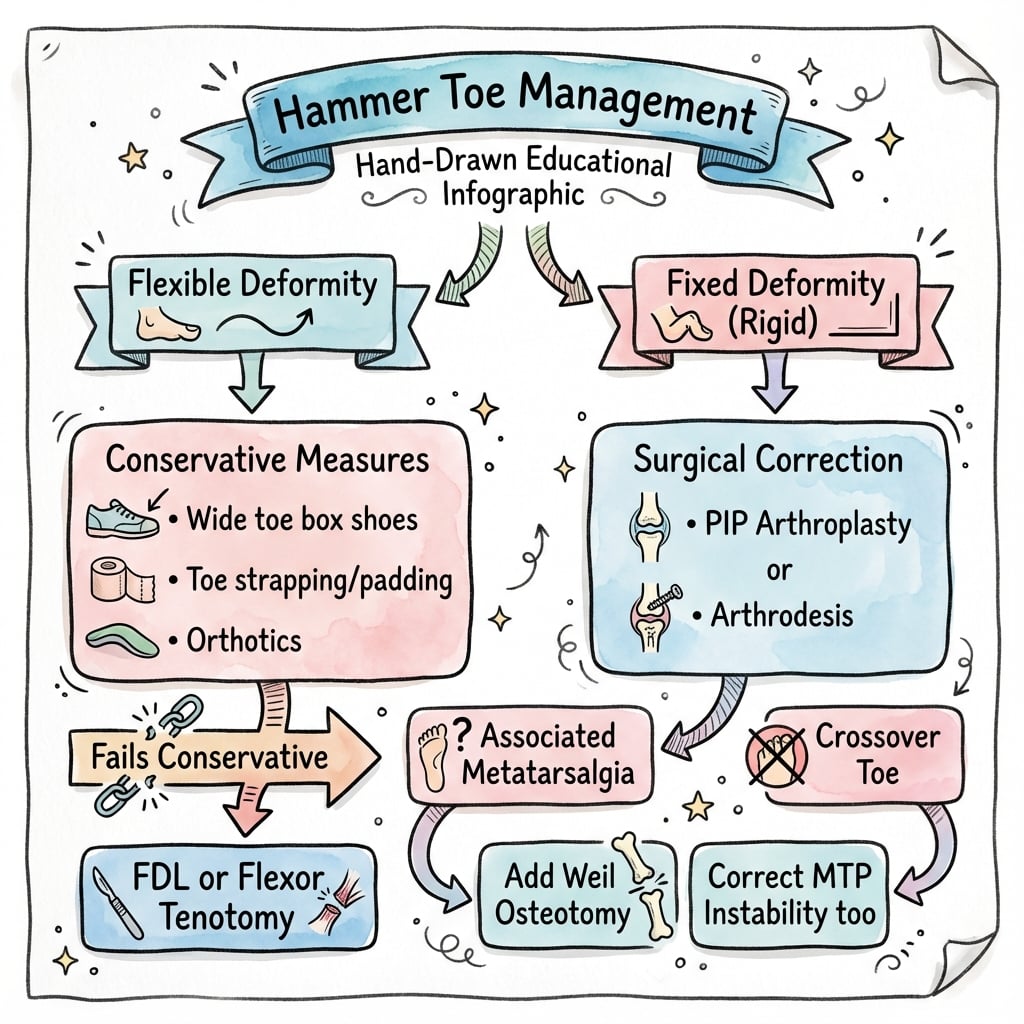
Floating Toe - Most Common Complaint
Floating toe is the most common post-operative complaint. The toe has no ground purchase and feels floppy. Prevention: avoid over-resection, use arthrodesis for stability, address MTPJ subluxation. Salvage is difficult.
Complications and Outcomes
Surgical Complications
Hammer Toe Surgery Complications
| Complication | Incidence | Risk Factors | Prevention/Management |
|---|---|---|---|
| Floating toe | 5-10% | Over-resection, tendon imbalance, MTPJ instability | Limit resection, arthrodesis, address MTPJ |
| Recurrence | 5-15% | Inadequate correction, not addressing MTPJ | Complete correction, treat all pathology |
| K-wire infection | 3-8% | Pin track contamination, diabetes | Pin care, early removal if infected |
| Stiffness | 5-10% | Excessive scarring, prolonged immobilization | Early mobilization, physiotherapy |
| Malalignment | 2-5% | Technical error, inadequate fixation | Careful intraoperative assessment |
| Transfer metatarsalgia | 5-10% | Shortening adjacent ray, overcorrection | Address all metatarsals, balanced correction |
Floating Toe - Most Common Complication
The toe has no ground purchase and feels floppy. Causes include over-resection at PIPJ, tendon imbalance, and unaddressed MTPJ subluxation. Prevention through conservative bone resection, arthrodesis for stability, and addressing MTPJ pathology is key. Salvage is difficult.
Prevention Strategies
- Conservative bone resection: Avoid over-resection at PIPJ
- Arthrodesis over arthroplasty: More stable correction for rigid deformities
- Address MTPJ: Weil osteotomy if subluxed
- K-wire care: Clean pin sites, adequate duration (3-4 weeks)
- Patient selection: Avoid surgery in poorly controlled diabetics
Postoperative Care
Immediate Postoperative Period (0-2 Weeks)
Day 0-1:
- Dressing: Bulky postoperative dressing maintaining toe alignment
- K-wire care: If used, wire exits dorsally - keep dry and protected
- Elevation: Essential - foot above heart level to minimize swelling
- Weight-bearing: Heel weight-bearing in stiff-soled postoperative shoe
Week 1-2:
- First follow-up: Wound check at 10-14 days
- Suture removal: Non-absorbable sutures at 2 weeks
- Swelling management: Expect significant toe swelling for 6-8 weeks
- Activity: Limited ambulation for essential activities only
Early Recovery Phase (2-6 Weeks)
Week 2-4:
- K-wire removal: If used, remove at 3-4 weeks in clinic
- Active ROM: Begin gentle active toe movements after wire removal
- Footwear: Continue stiff-soled shoe; transition to accommodative shoe with stiff sole
- Buddy taping: Tape corrected toe to adjacent toe for 4-6 weeks post-wire removal
Week 4-6:
- Progressive weight-bearing: Transition to supportive athletic shoe
- Physical therapy: If stiffness present - focus on PIPJ mobility
- Wound massage: Scar mobilization after complete healing
Late Recovery Phase (6-12 Weeks)
- Footwear transition: Gradual return to regular shoes (wide toe box initially)
- Swelling: Toe swelling may persist 3-6 months - normal finding
- Return to activities: Low-impact exercise at 6-8 weeks, sports at 10-12 weeks
- Final assessment: Evaluate alignment and ROM at 12 weeks
Clinical Pearl
Postoperative Swelling Timeline: Inform patients that toe swelling following hammer toe correction typically peaks at 2-3 weeks and may persist for 3-6 months. Prolonged swelling does not indicate failure if alignment is maintained.
Complications and Management
| Complication | Incidence | Prevention/Management |
|---|---|---|
| Recurrence | 5-15% | Proper patient selection; address MTPJ if subluxed |
| Floating toe | 2-5% | Avoid excessive plantar plate release |
| Mallet toe | 3-8% | Check DIPJ mobility preoperatively |
| Stiffness | 10-20% | Early ROM after fixation; consider arthroplasty in elderly |
| Infection | 1-3% | Standard wound care; K-wire pin site care |
| Transfer metatarsalgia | 5-10% | Address 1st ray pathology; consider Weil osteotomy |
Outcomes and Prognosis
Expected Outcomes
Conservative:
- Symptom relief in 50-70%
- Deformity NOT corrected
- Typically progress over time
- Average 2-3 years before surgery
Surgical:
- Overall Satisfaction: 80-90%
- Pain Relief: 85-95%
- Deformity Correction: 75-90%
- Recurrence: 5-10%
- Complications: 10-20%
Factors Affecting Outcome
- Positive: Flexible deformity, isolated PIPJ, no MTPJ involvement
- Negative: Rigid deformity, MTPJ subluxation, inflammatory arthritis, diabetic
Return to Activity
- Walking: 2-4 weeks post-op
- Driving: 4-6 weeks
- Dress Shoes: 6-8 weeks
- Sports: 8-12 weeks
- Final Result: 6-12 months
Controversies & Areas of Uncertainty
- Arthroplasty vs arthrodesis for rigid deformity — Arthrodesis offers a more stable, lower-recurrence construct but at the cost of a stiff toe and a non-union risk; resection arthroplasty preserves some motion but is more prone to recurrence and floating toe. No high-quality RCT directly settles the choice, so selection remains driven by patient age, activity and surgeon preference.
- Intramedullary implants vs K-wire — The single RCT favours implants for fusion rate and patient-reported scores, yet pooled reviews show higher hardware-failure rates and a 640-894x cost premium with no clear complication benefit. Whether the avoided pin-tract morbidity justifies the cost is unresolved.
- When to address the MTPJ / plantar plate — There is debate over whether all crossover and instability-driven deformities need formal plantar plate repair, or whether a Weil osteotomy with soft-tissue balancing alone suffices. The Coughlin-Nery staging is increasingly used to guide this, but thresholds vary.
- Floating toe is partly unavoidable — Even with meticulous technique, floating toe occurs in a meaningful proportion after Weil osteotomy and plantar plate work; its true preventability and the best salvage remain uncertain.
- Role of percutaneous (minimally invasive) techniques — Percutaneous flexor tenotomy and minimally invasive osteotomies are expanding, but long-term comparative data against open correction are still limited.
Evidence Base
- Multicentre RCT, 91 patients randomised to K-wire (n=46) vs 2-piece intramedullary implant (n=45) for PIPJ fusion
- No statistically significant difference in complication rates between groups
- Intramedullary implant group had higher mean Bristol Foot Score, Foot Function Index and a higher fusion rate
- Mean age 58.7 years, confirming the typical older demographic
- Prospective series of 22 patients (40 lesser MTP joints) with instability treated by direct dorsal plantar plate repair plus Weil osteotomy
- Second MTP joint most commonly affected (63%); Grade III tears most frequent
- Defined the anatomical grading correlated with clinical staging for plantar plate dysfunction
- AOFAS score improved from a mean of 52 to 92 points postoperatively
- Retrospective series of 32 patients (47 feet) at mean 6-year follow-up
- Fixed hammer toes corrected by PIPJ arthrodesis with intramedullary Kirschner-wire fixation
- Dislocated lesser MTP joints reduced from 70% preoperatively to 7% postoperatively
- 23 feet excellent, 22 good, 2 fair; no poor results - a stable first ray protected lateral rays
- 24 toes with flexible PIPJ and/or MTPJ deformity treated by Girdlestone-Taylor FDL flexor-to-extensor transfer
- 92% (22 toes) achieved physiological alignment at 6 weeks
- 16% had recurrent or persistent MTPJ extension deformity at final follow-up
- No infections, overcorrection or transverse malalignment
- Review of 3878 PIPJ arthrodesis outcomes (3255 percutaneous K-wires, 347 SmartToe, 218 ToeGrip, 58 buried K-wire)
- Infection rates low across all methods (K-wire 0.3-7%, SmartToe 1.2-5%)
- SmartToe implant had the highest hardware failure rate (up to 20.7%); K-wire the lowest (0.1-4.3%)
- Implants cost 640-894x more than a K-wire with no clear superiority in union
- Reviews indications and technique of central (Weil) metatarsal osteotomy for forefoot pain and MTPJ instability
- Floating toe and joint stiffness identified as the characteristic complications
- Treating only the pain focus underserves the deformity - the high point must be addressed
- Emphasises managing patient expectations and proactive complication avoidance
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Flexible Hammer Toe
"A 55-year-old woman presents with a painful 2nd toe deformity. She has a callus over the dorsal aspect of the PIPJ. On examination, the deformity corrects manually when you plantarflex her ankle."
Diagnosis: This is a flexible hammer toe of the 2nd toe. The key finding is that the deformity corrects manually with the ankle plantarflexed, which relaxes the FDL and confirms flexibility.
Clinical Assessment:
- Confirm flexibility by plantarflexing ankle
- Assess MTPJ with Drawer test for instability
- Check for associated hallux valgus
- Examine other toes
- Weight-bearing X-rays
Management:
- Conservative first: Shoe modifications (wide toe box, soft upper), padding, toe sleeves
- If fails conservative: Surgical intervention
- Flexible deformity = soft tissue surgery:
- FDL tenotomy (percutaneous) - simple, effective for isolated PIPJ
- Girdlestone-Taylor transfer - better if MTPJ instability
Key Principle: Flexible deformity does NOT require bone resection. Soft tissue balancing is sufficient. Over-treatment with bone resection risks floating toe.
Rigid Hammer Toe with MTPJ Involvement
"A 62-year-old man has a painful, rigid 2nd toe deformity. The PIPJ does not correct even with the ankle plantarflexed. You also notice the toe is dorsally displaced at the MTPJ level with a positive Drawer test."
Diagnosis: This is a rigid hammer toe with MTPJ subluxation (Grade 3 or 4 by Dhukaram classification). The combination requires addressing both levels.
Clinical Assessment:
- Confirm rigidity - does not correct with ankle plantarflexed
- Positive Drawer test confirms MTPJ instability
- Assess degree of MTPJ subluxation/dislocation
- Check for associated hallux valgus
- Weight-bearing X-rays - assess joint destruction
Surgical Management:
- PIPJ level: PIPJ resection arthroplasty or arthrodesis
- Arthrodesis preferred for stability and lower recurrence
- MTPJ level: Weil osteotomy to shorten metatarsal
- Combined with plantar plate repair if torn
- May need extensor tenotomy and MTPJ capsulotomy
- Fixation: K-wire through toe or intramedullary device
Complications to Discuss:
- Floating toe (most common complaint)
- Recurrence if MTPJ not addressed
- Stiffness post-arthrodesis
- Transfer metatarsalgia
Floating Toe Post-Surgery
"A patient returns 3 months after hammer toe surgery complaining their 2nd toe feels floppy and doesn't touch the ground when standing. They are unhappy with the result."
Diagnosis: This is a floating toe - the most common complication and complaint after hammer toe surgery. The toe lacks ground purchase and feels unstable.
Causes of Floating Toe:
- Over-resection of proximal phalanx head
- Excessive soft tissue release
- Tendon imbalance (weak flexors)
- MTPJ instability not addressed
- Malunion/non-union of fusion
Assessment:
- Examine toe position and ground contact
- Check flexor strength (FDL intact?)
- Assess MTPJ stability
- X-ray to assess bone resection, alignment, fusion
Management Options:
- Conservative: Strapping, buddy taping, time
- Surgical salvage (difficult):
- Flexor tendon transfer if intact
- MTPJ stabilisation procedure
- Bone grafting if over-resected
- Syndactylization to adjacent toe (last resort)
- Prognosis: Salvage surgery unpredictable, manage expectations
Prevention:
- Avoid over-resection
- Use arthrodesis for stability
- Address MTPJ subluxation at index surgery
- Adequate K-wire duration
MCQ Practice Points
Classic MCQ: Lesser Toe Deformity Definitions
Q: What distinguishes a hammer toe from a claw toe?
A: Hammer toe = PIPJ flexion with neutral MTPJ and DIPJ Claw toe = MTPJ hyperextension + PIPJ/DIPJ flexion
Hammer toe is most commonly 2nd toe, associated with hallux valgus. Claw toe typically affects multiple toes and has neurological associations (Charcot-Marie-Tooth, diabetic neuropathy).
Key Surgical Decision: Flexibility Assessment
Q: A 55-year-old woman has a painful 2nd hammer toe. The PIPJ deformity corrects passively. What is the first-line surgical treatment?
A: Flexor-to-extensor transfer (Girdlestone-Taylor procedure) - indicated for flexible deformities. Preserves joint motion.
If the PIPJ is fixed/rigid → PIPJ arthrodesis is indicated.
Critical Anatomy: Push-up Test
Q: What does the push-up test assess in hammer toe evaluation?
A: Tests MTPJ stability. With examiner pressure under the metatarsal head, a positive test shows correction of PIPJ deformity → indicates the problem is plantar plate/MTPJ driven, not isolated PIPJ contracture. May need Weil osteotomy in addition to toe surgery.
Complication Recognition
Q: Following hammer toe correction, a patient develops progressive DIPJ hyperextension ("floppy toe"). What is the cause?
A: FDL transection or excessive release during surgery. The FDL is the only active DIPJ flexor. If cut or transferred, unopposed EDL causes DIPJ hyperextension. Prevention: careful identification of FDL vs FDB.
Guidelines, Registries & Global Practice
Global Epidemiology
Lesser-toe deformities are among the most common forefoot complaints worldwide. Population studies report hammer/claw/mallet toes in a substantial minority of adults, rising steeply with age and strongly female-predominant (footwear and a longer second ray are the dominant drivers). Prevalence is higher in older, shod populations and lower in habitually barefoot communities, supporting footwear as a key modifiable factor. Hallux valgus coexists in the majority of symptomatic second-toe deformities.
Side-by-Side Guidance
| Body | Position on lesser-toe surgery |
|---|---|
| AOFAS / AAOS (US) | Flexible vs rigid distinction drives treatment; soft-tissue balancing for flexible, bony correction (arthroplasty/arthrodesis) for rigid; address MTPJ instability concurrently |
| BOA / BOFAS (UK) | Exhaust footwear and orthotic measures first; reserve surgery for failed conservative care; counsel explicitly on floating toe and recurrence |
| EFORT / European consensus | Endorses plantar plate staging (Coughlin-Nery) and combined Weil osteotomy plus plantar-plate repair for instability-driven deformity |
| IWGDF (diabetic foot) | In neuropathic feet, prioritise deformity offloading and ulcer prevention; weigh surgical correction against wound-healing and vascular risk |
There is no single international registry for lesser-toe surgery; comparative evidence comes from case series, the Jay/Malay fixation RCT, and large pooled fixation reviews rather than from arthroplasty-style joint registries.
High- vs Limited-Resource Practice Variation
- High-resource settings: Day-case surgery; growing use of intramedullary fusion implants despite cost and hardware-failure data favouring K-wires; frequent combined bunion + lesser-toe correction.
- Limited-resource settings: Percutaneous K-wire fixation and FDL tenotomy/transfer predominate (low cost, reliable); emphasis on footwear modification and offloading where surgical access is limited.
- Diabetic / neuropathic populations: Worldwide, the threshold for elective bony surgery is raised because of impaired healing; offloading, accommodative footwear and ulcer prevention take priority.
HAMMER TOES
Clinical summary
DEFINITION & TYPES
- •Hammer = PIPJ flexion, neutral MTPJ/DIPJ (80% of lesser toe)
- •Claw = MTPJ extension + PIPJ/DIPJ flexion (neurological)
- •Mallet = DIPJ flexion only (5%, terminal tendon)
- •2nd toe most common (80%) - length, hallux valgus
FLEXIBILITY TEST
- •Plantarflex ankle (relaxes FDL)
- •Attempt to correct PIPJ
- •Corrects = FLEXIBLE → soft tissue surgery
- •Fixed = RIGID → bone surgery
MTPJ ASSESSMENT
- •Drawer test - anterior subluxation
- •Positive = plantar plate rupture/MTPJ instability
- •Must address if subluxed (Weil osteotomy)
- •Missing MTPJ = recurrence
FLEXIBLE SURGERY
- •FDL tenotomy (percutaneous stab incision)
- •Girdlestone-Taylor (FDL split and transfer dorsally)
- •May need MTPJ capsulotomy
- •No bone resection needed
RIGID SURGERY
- •PIPJ resection arthroplasty (resect P1 head)
- •PIPJ arthrodesis (more stable, lower recurrence)
- •K-wire 3-4 weeks or intramedullary device
- •Weil osteotomy if MTPJ subluxed
COMPLICATIONS
- •Floating toe - MOST COMMON (floppy, no purchase)
- •Recurrence (5-10%)
- •K-wire infection (3-8%)
- •Stiffness, mallet toe, transfer lesions
OUTCOMES
- •80-90% satisfaction
- •Arthrodesis lower recurrence than arthroplasty
- •Conservative doesn't correct deformity
- •Full recovery 6-12 months