A Viral Fingertip Infection that Must NOT Be Incised
- Herpetic whitlow is a HERPES SIMPLEX VIRUS infection of the FINGERTIP (pulp/periungual skin), caused by HSV-1 or HSV-2; it characteristically produces a PRODROME of pain, tingling or burning followed by GROUPED VESICLES on an ERYTHEMATOUS base, with pain often OUT OF PROPORTION to the modest swelling.
- It classically affects YOUNG CHILDREN (autoinoculation from oral HSV - e.g. thumb-sucking/herpetic gingivostomatitis), HEALTHCARE WORKERS exposed to oral secretions (dentists, anaesthetists, respiratory staff - now much less common with universal glove use), and adults with genital HSV (HSV-2).
- THE KEY POINT: herpetic whitlow MUST NOT be treated like a felon - it must NOT be INCISED AND DRAINED. The fluid is viral (not pus), and incising it risks BACTERIAL SUPERINFECTION, delayed healing and potentially SYSTEMIC viral spread - a dangerous error, especially in the immunocompromised.
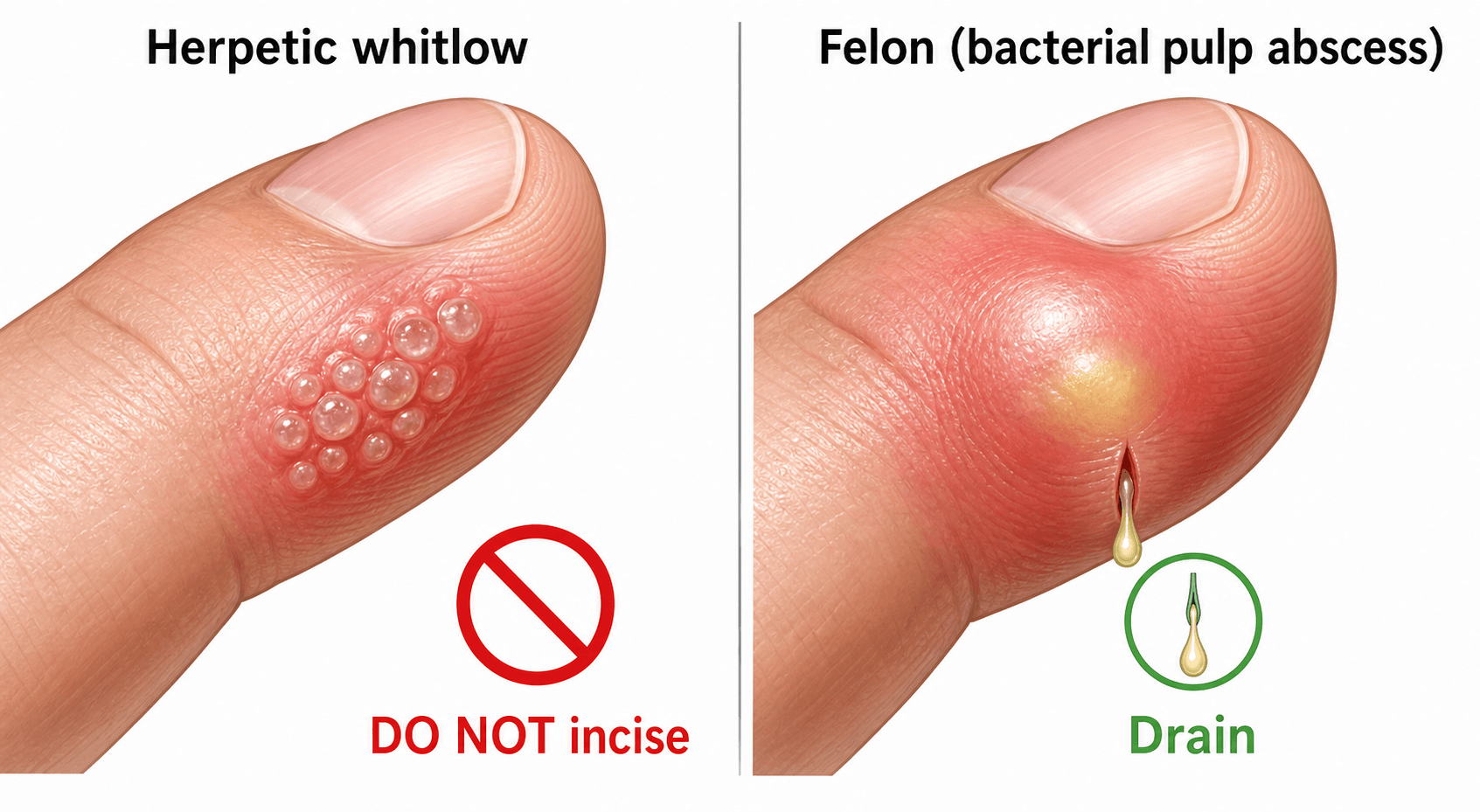
- It is therefore essential to DIFFERENTIATE it from a bacterial FELON (a purulent abscess of the closed pulp space that DOES need incision and drainage) and from acute paronychia: the grouped clear vesicles, the non-purulent vesicular fluid, the prodrome and the relatively soft (non-tense) pulp point to a viral whitlow.
- Diagnosis is usually CLINICAL; it can be confirmed by a TZANCK smear (multinucleated giant cells), HSV PCR (most sensitive/specific), viral culture or direct fluorescent antibody from vesicle fluid - useful when atypical or to avoid an inappropriate incision.
- Management is SUPPORTIVE - analgesia and keeping the lesion clean and COVERED (to prevent autoinoculation/transmission) - and the condition is SELF-LIMITING over about 2-4 weeks; ORAL ANTIVIRALS (aciclovir/valaciclovir) shorten and reduce symptoms, particularly when started EARLY, and are important in severe, recurrent or immunocompromised cases; antibiotics are reserved for proven SECONDARY bacterial infection.
- “Grouped CLEAR vesicles on an erythematous fingertip + pain out of proportion + prodrome = herpetic whitlow (HSV).
- “DO NOT incise & drain (it is viral, not pus) - incision risks superinfection/systemic spread. Felon (purulent pulp abscess) IS drained.
- “Self-limiting (~2-4 weeks); antivirals (aciclovir) help if early/severe/recurrent/immunocompromised; keep covered to prevent autoinoculation.
Grouped clear vesicles on an erythematous base, non-purulent, pain out of proportion, prodrome. Viral - supportive care +/- antivirals. Incising it is harmful.
Tense, throbbing, purulent abscess of the closed pulp space. Bacterial - needs incision & drainage + antibiotics.
Aetiology & Presentation
Herpetic whitlow is inoculation of herpes simplex virus into the skin of the fingertip through a breach. HSV-1 predominates in children (autoinoculation from oral herpes, e.g. thumb-sucking with herpetic gingivostomatitis) and in healthcare workers exposed to oral/respiratory secretions (dentists, anaesthetists, respiratory therapists - historically a classic occupational infection, now uncommon with glove use); HSV-2 affects adults via genital contact. After a prodrome of localised pain, tingling or burning, grouped vesicles appear on an erythematous, oedematous base; the vesicles contain initially clear then cloudy fluid and may coalesce, and the pain is often out of proportion to the swelling. Low-grade fever, lymphangitis and epitrochlear/axillary lymphadenopathy may occur. The virus then becomes latent in the sensory ganglion, so recurrence is possible.

The Natural History: Stages, Timeline and Infectivity
The whitlow is self-limiting over about 2-4 weeks and should be kept covered to prevent transmission, but the staged course and what it means for infectivity are the examinable points - especially as healthcare workers are a named at-risk group.
- Incubation: roughly 2 to 20 days (commonly 2 to 7) after inoculation.
- Prodrome: localised pain, tingling or burning before any rash - the window in which early antivirals are most effective.
- Vesicular stage: grouped vesicles on an erythematous base (clear then cloudy), which may coalesce and ulcerate; this is the most painful and most infectious phase.
- Crusting and healing: the vesicles dry, crust and re-epithelialise.
- Resolution: heals over about 2 to 4 weeks, usually without scarring.
- Latency and recurrence: the virus retreats to the sensory ganglion; recurrences are usually milder and shorter.
Lesions are infectious until fully crusted and healed, so an affected healthcare worker should avoid direct patient contact or keep the lesion securely covered (a glove over an occlusive dressing) until healed - the same covering that prevents the patient's own autoinoculation.
Because antivirals work best before the vesicles erupt, recognising the prodrome (and, in frequent recurrers, starting at the first tingle) is what makes antiviral therapy effective rather than cosmetic.
Diagnosis & Management
Diagnosis is usually clinical from the grouped vesicles, prodrome and non-purulent appearance. When atypical - or to avoid an inappropriate incision - confirm with a Tzanck smear (multinucleated giant cells), HSV PCR (most sensitive and specific), viral culture, or direct fluorescent antibody from vesicle fluid. Management:
- Supportive: analgesia, keep the lesion clean and covered with a dry dressing to limit autoinoculation (eye - herpetic keratitis - and genitals) and transmission to others; the condition is self-limiting over about 2-4 weeks.
- Antivirals: oral aciclovir/valaciclovir shorten the episode and symptoms, especially when started early, and are indicated in severe, recurrent or immunocompromised patients; suppressive antivirals may be used for frequent recurrences.
- Do NOT incise and drain - the cardinal rule.
- Antibiotics only for a proven secondary bacterial infection.
Prescribing the antiviral: dose, window and when it is pointless
"Antivirals help if started early" is only useful with the numbers attached, and this is the one prescribing decision the topic contains.
- The window is the point. Aciclovir inhibits viral replication, so it works while the virus is still replicating - within about 48 to 72 hours of symptom onset, and ideally in the prodrome, before the vesicles erupt. Started at day seven in a crusting lesion it does essentially nothing, and offering it then is treatment for the clinician rather than the patient.
- Regimens are the standard mucocutaneous HSV ones - aciclovir 400 mg orally five times daily for around 7 to 10 days is the commonly used course, with valaciclovir (twice daily) or famciclovir as better-absorbed, less frequent alternatives that suit adherence. Check the local formulary and adjust for renal impairment, since aciclovir is renally cleared.
- Topical aciclovir alone is not adequate for an established whitlow; it is the systemic drug that matters.
- Suppression rather than episodic treatment is the approach for frequent recurrences - continuous lower-dose aciclovir or valaciclovir, reviewed periodically.
- Escalate to intravenous aciclovir in the significantly immunocompromised patient, in extensive or systemic disease, or where there is any suggestion of dissemination - this group is the reason the no-incision rule is not merely a technicality.
How often does it come back?
Recurrence is not a footnote: a substantial minority of patients - reported across series in the region of a fifth to a half - will have at least one further episode, because the virus persists in the sensory ganglion of that digit. Recurrences are milder, shorter and in the same finger, often heralded by the same prodromal tingle, which is exactly what makes patient-initiated early treatment practical: the patient who knows the sensation can start treatment inside the effective window without waiting for an appointment. Counsel for this at the first episode rather than at the second.
Series report herpetic whitlow being misdiagnosed as a bacterial whitlow and incised, or even mistaken for non-accidental injury (cigarette burns) in children. Incising a herpetic whitlow can cause bacterial superinfection, delayed healing and a risk of systemic viral dissemination - dangerous in the immunocompromised. Always consider HSV in a vesicular fingertip lesion, keep it covered to prevent cross-infection and autoinoculation to the eye, and counsel about recurrence.
The Wider Differential of a Vesicular or Blistered Fingertip
The headline distinction is whitlow versus the bacterial pus mimics (felon, paronychia), but a vesicular or blistered fingertip has a wider differential worth knowing. The safe unifying rule is that a vesicular lesion should not be incised as if it were an abscess until HSV is excluded.
- Discriminating clue
- Prodrome; grouped CLEAR vesicles on erythema; pain out of proportion; non-purulent
- What it means for management
- DO NOT INCISE - drainage risks bacterial superinfection and prolongs it. Oral aciclovir if within 48 hours, dressing, analgesia; it is self-limiting over 2-3 weeks
- Discriminating clue
- Tense PURULENT pulp abscess / pus in the nail fold
- What it means for management
- This one DOES need incision and drainage plus antibiotics - a felon left undrained can go on to pulp necrosis or osteomyelitis of the distal phalanx
- Discriminating clue
- Tense superficial blister with PUS over the volar pad, usually in children
- What it means for management
- (bacterial - drain + antibiotics)
- Discriminating clue
- Vesicles on hands AND feet plus oral ulcers; systemic, child
- What it means for management
- (viral - supportive)
- Discriminating clue
- Animal (sheep/cattle) contact; a single papulo-nodule
- What it means for management
- (viral - self-limiting)
- Discriminating clue
- ITCHY not painful, exposure/atopy; or a clear trauma/heat history
- What it means for management
- Neither infective nor surgical - emollients, topical steroid or removal of the irritant; the itch-rather-than-pain history is what redirects you
Mnemonics & Memory Aids
WHITLOW
Hook:Every letter of WHITLOW says: viral, don't cut it, cover it, antivirals.
CLEAR vs PUS
Hook:CLEAR vesicles = leave it (viral); PUS = drain it (felon).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient presents with a painful, blistered, red fingertip. How do you tell a herpetic whitlow from a felon, and why does it matter?”
“Who gets herpetic whitlow, how would you treat it, and what complications would you warn about?”
What it is
- HSV-1/HSV-2 infection of the fingertip (pulp/periungual)
- Prodrome (pain/tingling) -> grouped vesicles on erythema; pain out of proportion
- At risk: children (oral autoinoculation), healthcare workers, adults with genital HSV
Differentiation
- Whitlow: grouped CLEAR vesicles, non-purulent (viral)
- Felon: tense PURULENT closed-pulp abscess (bacterial) - needs I&D
- Confirm HSV if unsure: Tzanck, PCR, culture, DFA
Management
- DO NOT incise & drain (risks superinfection/systemic spread)
- Supportive: analgesia, keep covered (prevent autoinoculation); self-limiting ~2-4 weeks
- Oral aciclovir/valaciclovir if early/severe/recurrent/immunocompromised; antibiotics only for 2ndary infection
Complications
- Autoinoculation (eye - herpetic keratitis; genitals)
- Secondary bacterial infection; systemic spread (immunocompromised)
- Recurrence (latency in sensory ganglion)
Evidence & Key Studies
Paediatric recurrent herpetic whitlow
- A child's recurrent herpetic whitlow was initially mistaken for a bacterial whitlow and treated with incision and drainage, and later misattributed to cigarette burns prompting a child-protection referral.
- Correct diagnosis was made by scraping and viral culture, with recovery after topical and systemic aciclovir; recurrence occurred years later.
- Highlights the danger of incorrect diagnosis and inappropriate incision, the risk of cross-infection, and the importance of recognising HSV - especially to protect immunocompromised contacts.
Herpetic whitlow associated with an eating disorder: a case report
- Herpetic whitlow is a localised cutaneous HSV-1/HSV-2 infection of the fingers that can be recurrent, here linked to autoinoculation behaviour.
- It presented as an eroded group of vesicles on an erythematous base and was diagnosed clinically from history and examination.
- It resolved within a week of topical and systemic aciclovir, illustrating the supportive/antiviral (non-surgical) management.
The danger of misdiagnosis and inappropriate incision (and the diagnosis by viral culture, treatment with aciclovir and tendency to recur) comes from the cited Patel case report, and the HSV-1/HSV-2 aetiology, grouped-vesicle presentation, clinical diagnosis and aciclovir response from the cited Aljehani report. The no-incision rule and the felon/paronychia differentiation are standard hand-surgery teaching, as are the antiviral regimens and treatment window, the escalation to intravenous therapy in the immunocompromised, and the recurrence counselling. (See also Felon, Paronychia and Flexor Tenosynovitis.)