Spasticity & Neuroregression - CP-Like but Progressive
- HEREDITARY SPASTIC PARAPLEGIA (HSP) is a genetically HETEROGENEOUS group of inherited neurodegenerative disorders of the CORTICOSPINAL TRACTS (and dorsal columns) causing PROGRESSIVE LOWER-LIMB SPASTICITY, hyperreflexia and a SPASTIC GAIT; it occurs in 'pure' (predominantly spastic) and 'complex' (with additional neurological features) forms.
- METACHROMATIC LEUKODYSTROPHY (MLD) is an AUTOSOMAL-RECESSIVE LYSOSOMAL storage LEUKODYSTROPHY (deficiency of arylsulfatase A, with sulfatide accumulation and central/peripheral demyelination) causing progressive NEUROREGRESSION - loss of motor and cognitive skills with evolving tone abnormalities (spasticity, sometimes preceded by hypotonia) and contractures.
- The ORTHOPAEDIC SEQUELAE of both follow from the SPASTICITY/upper-motor-neuron picture and resemble those of CEREBRAL PALSY: lower-limb spasticity produces EQUINUS and PES PLANOVALGUS feet, a FLEXED-KNEE 'CROUCH' gait, hip FLEXION/ADDUCTION deformity with HIP DISPLACEMENT/subluxation, and progressive CONTRACTURES - and children with HSP develop pes planovalgus and a flexed-knee gait managed with foot orthoses to control plantar pressure and improve gait.
- THE COMMONEST PLACE HSP IS MET IS A CEREBRAL-PALSY CLINIC, UNDER THE WRONG LABEL. In an Alberta HSP registry, 14 of the families whose children presented with spasticity had first been diagnosed with CEREBRAL PALSY - 70 PERCENT of those presenting under 3 YEARS of age - and the correct diagnosis was only made when SYMPTOMS PROGRESSED and prompted neurogenetic assessment. The red flag is spastic diplegia WITHOUT a clear history of prematurity, intrauterine growth restriction, infection or vascular insult. The orthopaedic surgeon reviewing a 'static' diplegia serially is often the first person positioned to notice that it is not static.
- NEUROMUSCULAR SCOLIOSIS and other spinal deformity can occur (more so in the more severely affected/MLD), and overall the orthopaedic management borrows the principles used in CEREBRAL PALSY - tone management, orthoses, physiotherapy and selective soft-tissue/bony surgery.
- The CRUCIAL DIFFERENCE from cerebral palsy is that HSP and MLD are PROGRESSIVE (not static) disorders - the neurological deficit and deformity worsen over time (MLD often relentlessly) - so management goals, the timing/extent of surgery and surveillance must be TAILORED to the disease trajectory and prognosis rather than assuming a stable baseline.
- BE HONEST THAT THE MANAGEMENT IS BORROWED, NOT EVIDENCED. There is essentially NO condition-specific orthopaedic outcome literature for HSP or MLD - no series of hip surveillance, no comparative results for soft-tissue or bony surgery, no scoliosis cohort, and no validated migration-percentage programme. Every threshold and protocol used is imported from CEREBRAL PALSY, where the disease is static, so applying it to a progressive disorder is a reasoned extrapolation rather than an evidence-based standard. Say so when asked, and let the trajectory rather than a borrowed number drive the decision.
- MANAGEMENT is MULTIDISCIPLINARY and largely the same toolkit as spastic CP: SPASTICITY/TONE management (physiotherapy, oral agents, botulinum toxin, in selected cases baclofen), ORTHOSES (e.g. AFOs, custom insoles for pes planovalgus/foot pressure), and SELECTIVE SURGERY (soft-tissue releases/lengthenings, foot reconstruction, hip surveillance/reconstruction, scoliosis correction) - all framed by the progressive natural history and realistic functional goals.
- “HSP = inherited corticospinal-tract disorder -> PROGRESSIVE lower-limb spasticity + spastic gait. MLD = lysosomal leukodystrophy (arylsulfatase A) -> neuroregression with evolving tone/contractures.
- “Orthopaedic sequelae are SPASTICITY-driven and CP-like: equinus/pes planovalgus, flexed-knee CROUCH, hip flexion/adduction with HIP DISPLACEMENT, contractures, neuromuscular scoliosis.
- “Manage with the CP toolkit (tone management, orthoses/AFOs, selective surgery, hip + spine surveillance) - but remember these are PROGRESSIVE (unlike static CP), so tailor goals/surveillance/surgery to the trajectory.
- “The high-yield practical point: 70% of HSP children presenting under 3 years had first been diagnosed with CEREBRAL PALSY, corrected only when symptoms PROGRESSED. Suspect HSP in spastic diplegia WITHOUT prematurity, IUGR, infection or vascular insult. And note that every threshold used - including hip surveillance - is imported from CP; there is no condition-specific orthopaedic outcome evidence in either disease.
Spasticity-driven, like CP: equinus/pes planovalgus, flexed-knee crouch, hip flexion/adduction with hip displacement, contractures, neuromuscular scoliosis.
HSP and MLD are progressive (not static like CP) - MLD often relentlessly. Tailor goals, surgery timing and surveillance to the disease trajectory.
HSP Genetics and Classification
- The SPG nomenclature. HSP genetic types are designated SPG1 to SPG80+ (over 80 loci). The commonest is SPG4 (SPAST gene, spastin) - autosomal dominant, and the commonest cause of pure adult-onset HSP; other frequent types include SPG3A (atlastin, AD, childhood-onset), SPG11 (spatacsin, the commonest autosomal-recessive/complex form, with a thin corpus callosum) and SPG7 (paraplegin, AR). Inheritance may be autosomal dominant, autosomal recessive, X-linked or mitochondrial.
- Pure vs complex. Pure (uncomplicated) HSP is spastic paraparesis with, at most, dorsal-column sensory loss and urinary urgency; complex (complicated) HSP adds features such as ataxia, cognitive impairment, peripheral neuropathy, epilepsy, retinopathy or a thin corpus callosum.
- Why the lower limbs, with preserved power. HSP is a length-dependent, "dying-back" degeneration of the longest axons - the distal corticospinal tracts to the legs and the dorsal columns - so the lower limbs are affected first, the hands are spared, and power is relatively preserved (spasticity out of proportion to weakness), which shapes the orthopaedic (foot/knee/hip) pattern.
Q: How is HSP classified genetically, and why does it affect the lower limbs with preserved power?
A: HSP genetic types are designated SPG1-SPG80+. The commonest is SPG4 (SPAST/spastin, autosomal dominant); others include SPG3A (atlastin), SPG11 (spatacsin - commonest AR/complex, thin corpus callosum) and SPG7 (paraplegin); inheritance AD/AR/X-linked/mitochondrial. Pure = spastic paraparesis +/- dorsal-column loss/urinary urgency; complex adds ataxia/cognitive/neuropathy/thin-corpus-callosum. It is a length-dependent "dying-back" degeneration of the longest axons (distal corticospinal + dorsal columns), so the lower limbs go first, hands are spared, and power is relatively preserved (spasticity greater than weakness).
The Disorders, Sequelae & Management
HSP is a heterogeneous group of inherited corticospinal-tract disorders causing progressive lower-limb spasticity and a spastic gait; MLD is an autosomal-recessive lysosomal leukodystrophy (arylsulfatase A) causing progressive neuroregression with evolving tone and contractures. The orthopaedic sequelae of both are spasticity-driven and resemble cerebral palsy: equinus/pes planovalgus, a flexed-knee crouch, hip flexion/adduction with hip displacement, progressive contractures, and neuromuscular scoliosis. Management uses the CP toolkit - tone management (physiotherapy, botulinum toxin, baclofen in selected cases), orthoses (AFOs/insoles), and selective surgery (releases/lengthenings, foot reconstruction, hip/spine surveillance and reconstruction) - but with the key difference that these are progressive disorders, so goals and surveillance are tailored to the trajectory.
The orthopaedic care of hereditary spastic paraplegia and metachromatic leukodystrophy borrows heavily from the management of spastic cerebral palsy, because the spasticity/upper-motor-neuron picture produces the same lower-limb problems - equinus and pes planovalgus feet, a flexed-knee crouch gait, hip flexion/adduction with the risk of hip displacement, progressive contractures, and neuromuscular scoliosis - and the same toolkit applies: tone management, orthoses, physiotherapy, and selective soft-tissue and bony surgery, with hip and spine surveillance. The crucial difference, and the safety point, is that unlike cerebral palsy these are progressive disorders: HSP worsens over time and MLD is a relentlessly progressive leukodystrophy, so the clinician must not assume a stable baseline when planning surgery or setting goals. The natural history and prognosis should shape decisions - the timing and extent of surgery, the realistic functional aims, and the intensity of surveillance - within a multidisciplinary team that includes neurology/genetics, and with honest discussion of trajectory (especially in MLD).
The pages these principles are borrowed from are worth reading as the source of every threshold used here: cerebral palsy for the overall framework, cerebral palsy hip surveillance for the migration-percentage programme, cerebral palsy gait and single-event multilevel surgery for the crouch and lever-arm reasoning, spastic equinovarus foot for the foot, and neuromuscular scoliosis for the spine. The other inherited neuropathy that reaches a paediatric orthopaedic clinic with a progressive foot deformity is covered under hereditary motor and sensory neuropathies.
MLD: Subtypes, the Mixed Nerve Picture, and Therapy That Changes the Trajectory
- The subtypes (age of onset drives speed). Late-infantile (commonest, onset ~6 months to 2-3 years) - a previously-walking toddler regresses with rapid motor and cognitive decline, often fatal within a few years; juvenile (onset ~3-16 years) - cognitive/behavioural decline with gait problems, slower; adult (onset over 16 years) - psychiatric/cognitive presentation, slowest. The later the onset, the slower the course.
- A mixed upper- and lower-motor-neuron picture. Central demyelination gives UMN spasticity/hyperreflexia, but the peripheral demyelinating neuropathy gives LMN signs - weakness and, characteristically, absent or reduced reflexes - so a child may show spasticity with lost reflexes (a diagnostic clue), evolving to hypotonia/areflexia as the disease advances. Diagnosis rests on low arylsulfatase A activity, raised urinary sulfatides, ARSA gene testing, and MRI (symmetric periventricular demyelination in a "tigroid"/leopard-skin pattern) with nerve-conduction evidence of a demyelinating neuropathy.
- Disease-modifying therapy changes the orthopaedic trajectory. Haematopoietic stem-cell transplant (for pre-symptomatic later-onset disease) and gene therapy - atidarsagene autotemcel (arsa-cel, "Libmeldy"), an ex-vivo autologous ARSA gene therapy for pre-symptomatic late-infantile and early-juvenile MLD - can halt or slow the disease if given early. A treated, stabilised child has a more static (CP-like) trajectory, which shifts orthopaedic decision-making from purely palliative toward the standard surveillance/reconstruction used in cerebral palsy.
Q: What are the MLD subtypes, and why do the mixed nerve picture and modern therapy matter orthopaedically?
A: By onset: late-infantile (commonest, ~6 months-2 years, rapid regression of a walking toddler, often fatal in a few years), juvenile (~3-16 years), adult (over 16 years, psychiatric) - later onset = slower. Central demyelination gives UMN spasticity but the peripheral neuropathy gives LMN weakness and ABSENT REFLEXES (spasticity with lost reflexes is the clue); diagnosed by low arylsulfatase A, raised urinary sulfatides and a tigroid MRI. Crucially, HSCT and gene therapy (atidarsagene autotemcel / "Libmeldy") given pre-symptomatically can halt the disease - converting a relentless leukodystrophy into a more static, CP-like trajectory that shifts orthopaedic care from palliative toward standard surveillance/reconstruction.
The Child in Front of You Is Probably Labelled Cerebral Palsy
This is not a rare academic distinction - it is the usual situation. In an Alberta registry of 90 HSP families, 29 had a paediatric presentation of spasticity and 20 presented under 3 years; 14 families had received an initial diagnosis of cerebral palsy, amounting to 70 percent of those presenting under 3. In every case the label was corrected only after the symptoms progressed and prompted neurogenetic assessment, with exome sequencing identifying a pathogenic variant in nine of the fourteen. The clinical rule the authors draw is worth memorising: in a young child with spastic diplegia and no clear history of prematurity, intrauterine growth restriction, infection or vascular insult, consider HSP. An orthopaedic surgeon following a "CP" diplegia through serial gait and hip assessments is often the first clinician in a position to see that the picture is progressing rather than growing out of proportion - and the diagnosis changes prognosis, surgical planning and the family's recurrence risk.
There is essentially no condition-specific orthopaedic outcome evidence in HSP or MLD - no hip-surveillance series, no comparative surgical results, no scoliosis cohort, no validated migration-percentage threshold. Everything is imported from cerebral palsy, a static encephalopathy. That extrapolation is reasonable but it is an extrapolation, and in a progressive disease a CP-derived threshold may act too late.
Follow the trajectory, not a single measurement: serial gait, serial migration percentage and serial spinal assessment tell you more than any borrowed cut-off. Set goals against the expected course - and in MLD ask whether the child has had stem-cell transplant or gene therapy, because a stabilised child behaves far more like the CP population the protocols were written for.
Mnemonics & Memory Aids
SPASTIC
Hook:SPASTIC: Spasticity/Storage, Progressive, Ankle (equinus/planovalgus), Stance (crouch), Tone management, (hip) Instability, Curve/Contractures (CP toolkit).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How do the orthopaedic problems of hereditary spastic paraplegia and metachromatic leukodystrophy compare with cerebral palsy, and how does that change management?”
The disorders
- HSP: inherited corticospinal-tract disorder -> progressive lower-limb spasticity + spastic gait
- MLD: autosomal-recessive lysosomal leukodystrophy (arylsulfatase A) -> neuroregression
- Both progressive (unlike static cerebral palsy)
- 70 percent of HSP presenting under 3 years was first diagnosed as CP - suspect it without a perinatal cause
Orthopaedic sequelae (spasticity-driven)
- Equinus / pes planovalgus; flexed-knee crouch gait
- Hip flexion/adduction with hip displacement/subluxation; contractures
- Neuromuscular scoliosis
Management
- CP toolkit: tone management (physio/botulinum toxin/baclofen), orthoses/AFOs
- Selective surgery (releases/lengthenings, foot, hip/spine reconstruction); hip + spine surveillance
- Tailor goals/surgery timing/surveillance to the progressive trajectory; MDT (neurology/genetics)
- Every threshold is borrowed from CP - no condition-specific orthopaedic outcome evidence exists; follow the trajectory, not a cut-off
Evidence & Key Studies
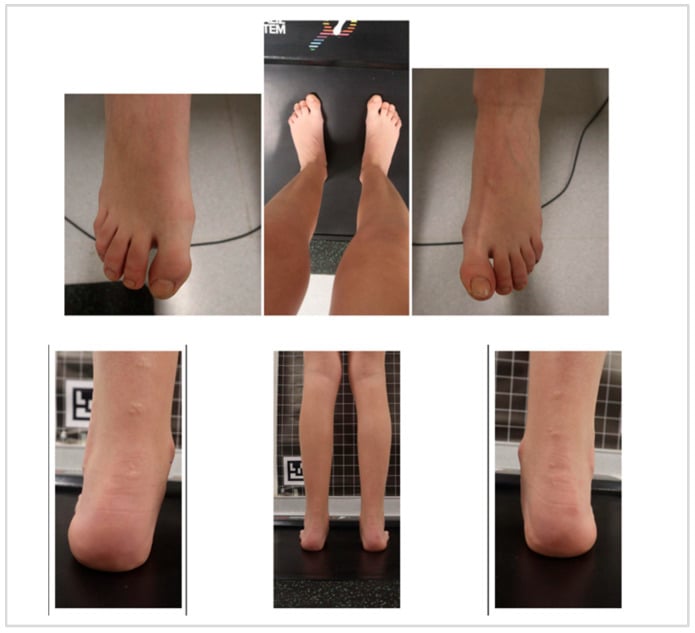
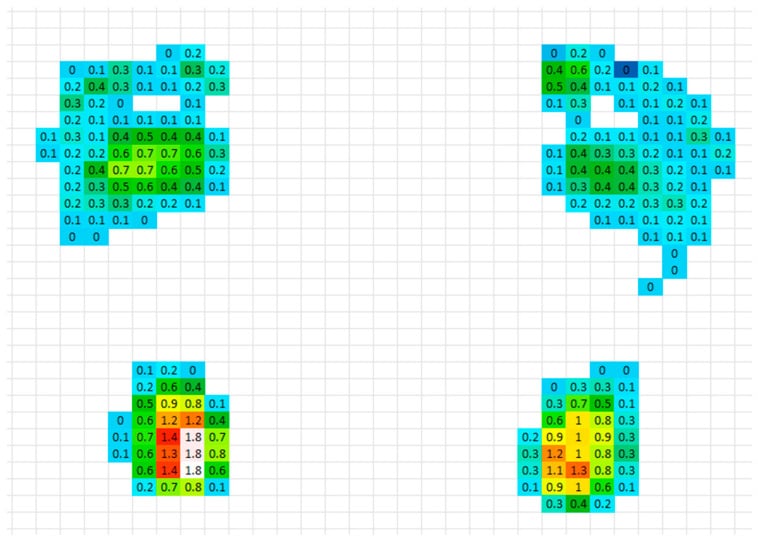
Foot orthoses for pes planovalgus and flexed-knee gait in a child with hereditary spastic paraplegia
- Children with hereditary spastic paraparesis develop foot/lower-limb deformity (pes planovalgus and a flexed-knee gait), and customised foot orthoses are widely used to manage plantar pressure and improve structural support.
- Optimised personalised insoles substantially reduced peak plantar pressure and improved load distribution in a paediatric patient with HSP, pes planovalgus and flexed-knee gait.
- Orthotic management is a noninvasive intervention to prevent secondary complications and improve gait mechanics in HSP - reflecting the spasticity-driven, CP-like orthopaedic sequelae.
Hereditary spastic paraplegia initially diagnosed as cerebral palsy
- From an Alberta registry of 90 HSP families, individuals in 29 families had a paediatric presentation of spasticity and 20 presented under 3 years of age. Fourteen families had received an initial diagnosis of cerebral palsy - 70 percent of the children presenting under 3 - with the correct diagnosis made only after symptom progression prompted neurogenetic assessment.
- Whole exome sequencing identified pathogenic or likely pathogenic variants in nine of the fourteen cases across six genes; in the remaining five, progression and a positive family history made HSP the most likely diagnosis without a confirmed variant.
- The authors conclude that in a young child with spastic diplegia and no clear history of prematurity, intrauterine growth restriction, infection or vascular insult, HSP should be considered, because accurate diagnosis alters prognosis, management and recurrence risk. This is a registry chart review from one Canadian province and cannot give the proportion of all CP-labelled children who in fact have HSP.
The development of pes planovalgus and a flexed-knee gait in children with hereditary spastic paraplegia and the role of foot orthoses to manage plantar pressure and improve gait come from the cited Alsaleh report. The corticospinal-tract basis and progressive nature of HSP, the lysosomal (arylsulfatase A) basis and neuroregression of metachromatic leukodystrophy, the broader spasticity-driven CP-like sequelae (equinus, crouch, hip displacement, contractures, neuromuscular scoliosis), and management with the cerebral-palsy toolkit (tone management, orthoses, selective surgery, hip/spine surveillance) tailored to the progressive trajectory are standard, well-established teaching. The misdiagnosis figures come from the Suchowersky registry review, which is from a single Canadian province and describes the proportion of known HSP patients previously labelled CP - not the proportion of CP-labelled children who actually have HSP. Beyond that, there is essentially no condition-specific orthopaedic outcome literature: no hip-surveillance series, no comparative results for soft-tissue or bony surgery, no scoliosis cohort, no validated migration-percentage threshold and no return-to-function data in either disease. Every protocol quoted here is imported from cerebral palsy, and the page says so rather than presenting borrowed thresholds as established for these conditions.