Articular Surface | Head Split | Impression | High AVN Risk
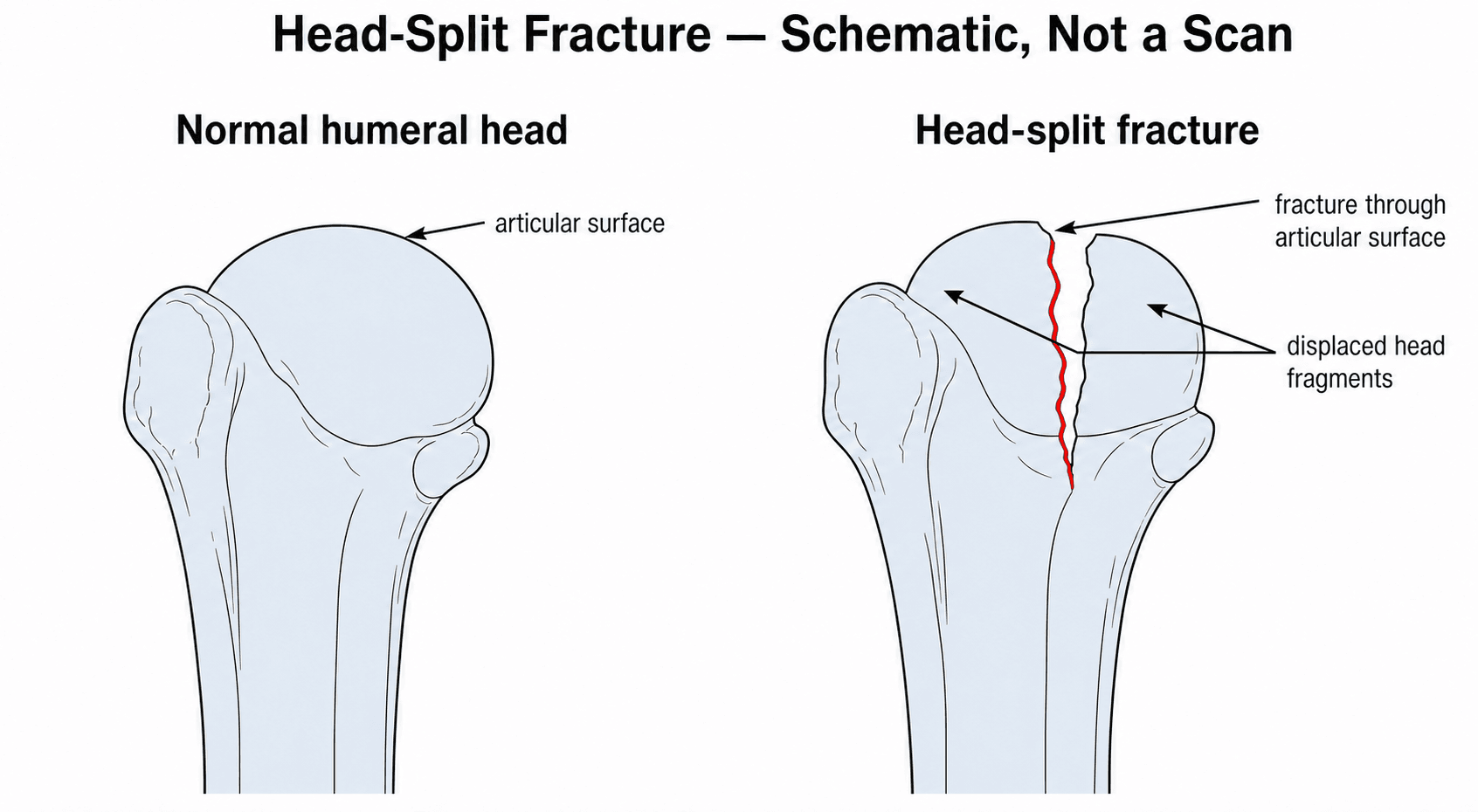
- Head Split Definition: A fracture line traversing the articular surface of the humeral head
- Blood Supply: Disruption of the arcuate artery (ascending branch of circumflex) leads to AVN
- Impression Fractures: Often associated with dislocations (Hill-Sachs or Reverse Hill-Sachs)
- Surgical Dilemma: Reconstruct (high failure rate) vs Replace (activity restrictions)
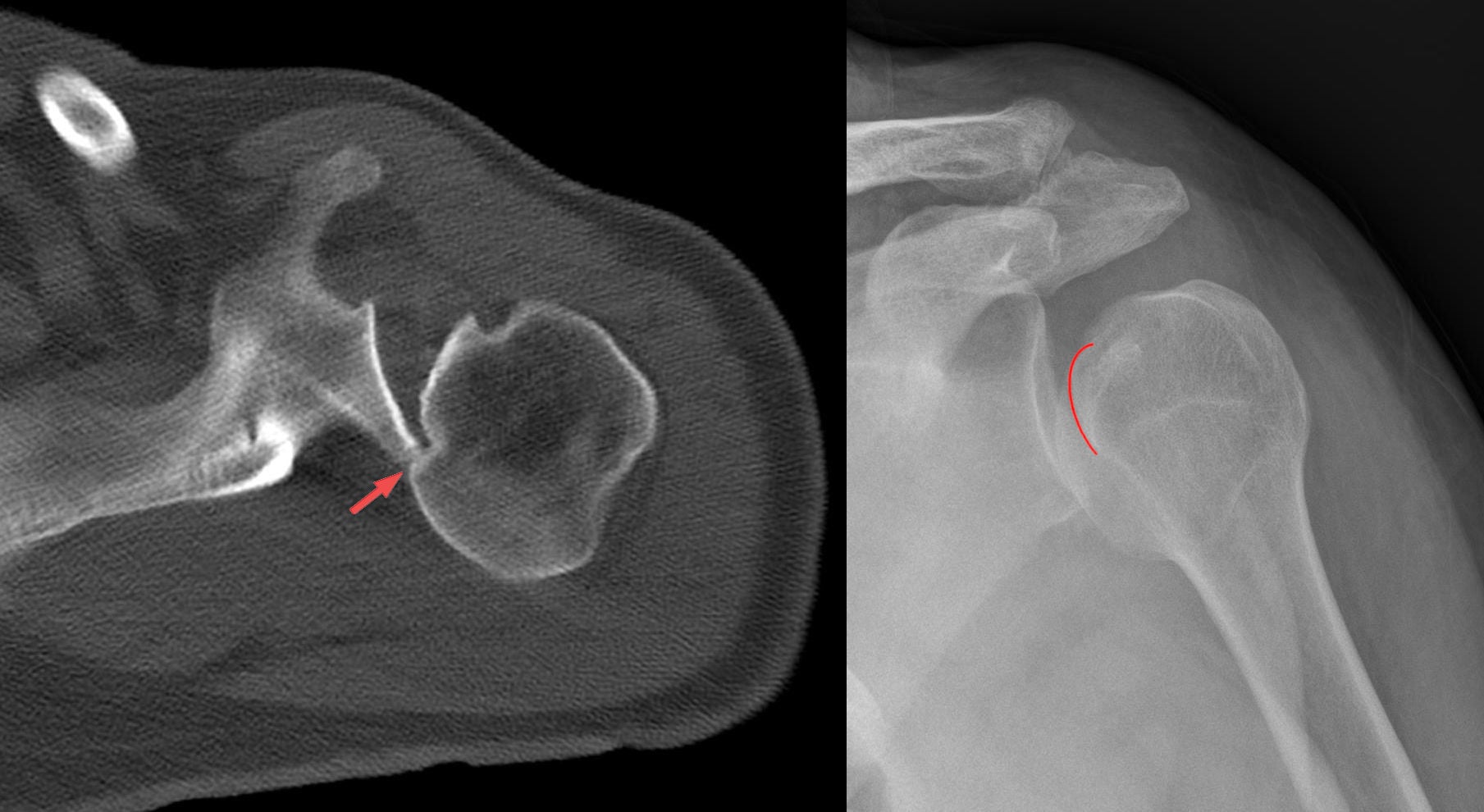
- Examination: Often indistinguishable from other proximal humerus fractures without CT
- “Head-splitting fractures are non-reconstructable in the elderly
- “Headless compression screws (Herbert) are used for articular fixation
- “Reverse Total Shoulder is preferred for elderly with cuff dysfunction
- “Monitor for post-traumatic arthritis
Definition: A true head-split fracture separates the articular surface into segments. It has a very poor prognosis for AVN and is difficult to fix reliably.
Impression Association: Impression fractures (Reverse Hill-Sachs) affecting greater than 40% of the head surface are often caused by missed posterior dislocations.
Neurovascular Check: Always assess axillary nerve function. The proximity to the surgical neck puts it at risk.
CT is Mandatory: Plain X-rays cannot accurately characterize the percentage of articular involvement or the number of head fragments.
- Population
- Young (less than 55)
- Key factor
- Bone stock good
- Treatment
- ORIF (Headless screws)
- Population
- Elderly (greater than 65)
- Key factor
- Poor bone stock
- Treatment
- Hemi or Reverse Arthroplasty
- Population
- Any
- Key factor
- Less than 20%
- Treatment
- Non-operative
- Population
- Active
- Key factor
- Greater than 40%
- Treatment
- Allograft / Arthroplasty
LEGOAVN Risk Factors
Hook:If the LEGO pieces are broken (calcar, hinge), AVN risk is high.
Overview
Humeral head fractures involve the articular surface of the proximal humerus. They are distinct from extra-articular tuberosity or surgical neck fractures. These injuries pose significant challenges due to the risk of avascular necrosis (AVN), post-traumatic arthritis, and technical difficulty in reduction.
Mechanism:
- High energy trauma (axial load)
- Fall from height
- Seizures (Impression/Dislocation)
- Osteoporotic bone collapse
Outcomes:
- High rate of complications
- AVN is the primary concern
- Stiffness is common
- Arthroplasty reliable for pain relief but variable function
Anatomy and Pathophysiology
Anatomical Considerations
- Branch of Anterior Humeral Circumflex artery.
- Ascends in bicipital groove.
- Enters head at ligamentous insertion.
- Main supplier to humeral head.
- Current evidence suggests this provides significant supply via posterior cuff.
- Medial hinge preservation protects this supply.
Disruption of the medial calcar often compromises perfusion.
Blood Supply of the Humeral Head: Classic vs Current
Because AVN is the complication that defines this topic, the blood supply deserves to be developed in full - including the modern revision that the anatomy tab hints at ("current evidence suggests the posterior circumflex provides significant supply") but never explains.
The classic teaching is that the anterior humeral circumflex artery (AHCA) is the dominant supplier, via its ascending branch (the arcuate artery / "Laing's arcuate"), which runs up the lateral bicipital groove and enters the bone to perfuse most of the head. This is why the classic exam answer to "which artery is most at risk?" remains the AHCA/arcuate, and why anatomical-neck fractures (which sever it as it enters the head) carry the highest AVN risk.
The modern revision. Quantitative perfusion studies (contrast-enhanced MRI and cadaveric injection work) have shown that the posterior humeral circumflex artery (PHCA) actually supplies the majority of the humeral head - on the order of two-thirds - entering posteromedially. This reframes the medial calcar / medial hinge as critical: an intact dorsomedial metaphyseal segment (the Hertel "calcar") preserves the PHCA contribution, which is exactly why a calcar under ~8 mm predicts ischaemia.
- Classic teaching
- The dominant supply; enters via the lateral bicipital groove
- Current evidence
- A real but smaller contribution; severed in anatomical-neck fractures
- Classic teaching
- A minor contributor
- Current evidence
- Supplies the MAJORITY (~2/3) of the head, entering posteromedially
- Classic teaching
- Protect the arcuate artery in the groove
- Current evidence
- Preserve the MEDIAL HINGE/CALCAR - it carries the dominant posterior supply (links directly to the Hertel under-8mm rule)
This is why the two facts in this topic fit together: the arcuate artery is the classic "named" vessel disrupted in anatomical-neck splits, but it is the length of attached medial calcar (preserving the posterior circumflex) that most strongly predicts whether the head will actually stay perfused.
Name the arcuate branch of the anterior circumflex as the classic vessel "at risk" in an anatomical-neck fracture, then score the higher mark by adding that modern perfusion studies show the posterior circumflex supplies most of the head, which is why preserving the medial calcar/hinge (Hertel, under ~8 mm = high ischaemia risk) is the single most important vascular consideration in fixation.
Classification
Classification
Articular Segment Involvement:
- Anatomical Neck Fracture: Rare, high AVN risk.
- Impression Fracture:
- Less than 20%
- 20-40%
- Greater than 40%
- Head Splitting: Comminuted articular surface.
Neer focused on displacement and AVN risk.
- AVN Risk
- High
- Reconstructability
- Difficult but possible
- Treatment Choice
- ORIF (Attempt salvage)
- AVN Risk
- Very High
- Reconstructability
- Poor
- Treatment Choice
- Arthroplasty
- AVN Risk
- Low
- Reconstructability
- Good (Ignore)
- Treatment Choice
- Non-op
- AVN Risk
- Variable
- Reconstructability
- Poor
- Treatment Choice
- Arthroplasty / Allograft
The "Head Split" is the most feared pattern. In an elderly patient, it is an automatic indication for arthroplasty as fixation failure and AVN are almost guaranteed.
Clinical Assessment
History and Physical Examination
History
- High energy fall or MVA (Young).
- Low energy fall (Elderly).
- Seizure (Think posterior dislocation/impression).
- Severe pain.
- Crepitus with ANY motion.
- global swelling.
Severe crepitus suggests intra-articular comminution.
Examination
- Extensive ecchymosis (Chest wall/Arm).
- Deformity.
- Axillary Nerve: Check deltoid tone and patch sensation.
- Distal Pulses: Ensure vascular tree is intact.
- Do NOT check ROM: Aggressive motion can displace fragments further.
- Gentle pendulum only if stable.
Protect the soft tissues and neurovascular structures.
Investigations
Imaging Studies
- AP (Grashey): Joint space narrowing, fragmentation.
- Scapular Y: Dislocation check.
- Axillary: Key for head shape and tuberosity position.
- Often underestimates articular involvement.
- Overlapping shadows obscure split lines.
Plain films are screening tools only.
Differential Diagnosis
A head-splitting or impression fracture must be distinguished from the more common proximal humeral injuries and from non-fracture causes of acute shoulder pain, because management diverges sharply.
- Distinguishing features
- Vertical line through articular surface; high AVN risk; intra-articular fragments
- Key investigation
- CT (mandatory)
- Management contrast
- ORIF in young, arthroplasty in elderly
- Distinguishing features
- Extra-articular; metaphyseal; tuberosities and head intact
- Key investigation
- AP and axillary radiographs
- Management contrast
- Often non-operative (PROFHER)
- Distinguishing features
- Extra-articular avulsion; superior displacement; cuff at risk
- Key investigation
- Axillary view, MRI for cuff
- Management contrast
- Fix if displaced over 5mm
- Distinguishing features
- Light-bulb sign; reverse Hill-Sachs impression; arm fixed in internal rotation
- Key investigation
- Axillary view / CT
- Management contrast
- Reduction then defect-size-based repair
- Distinguishing features
- Squared-off shoulder; posterolateral impression; recurrent instability
- Key investigation
- AP/axillary, CT for bone loss
- Management contrast
- Reduction; address engaging lesion
- Distinguishing features
- Chronic pain, no acute trauma, osteophytes
- Key investigation
- Radiographs
- Management contrast
- Non-operative or elective arthroplasty
Management Algorithm
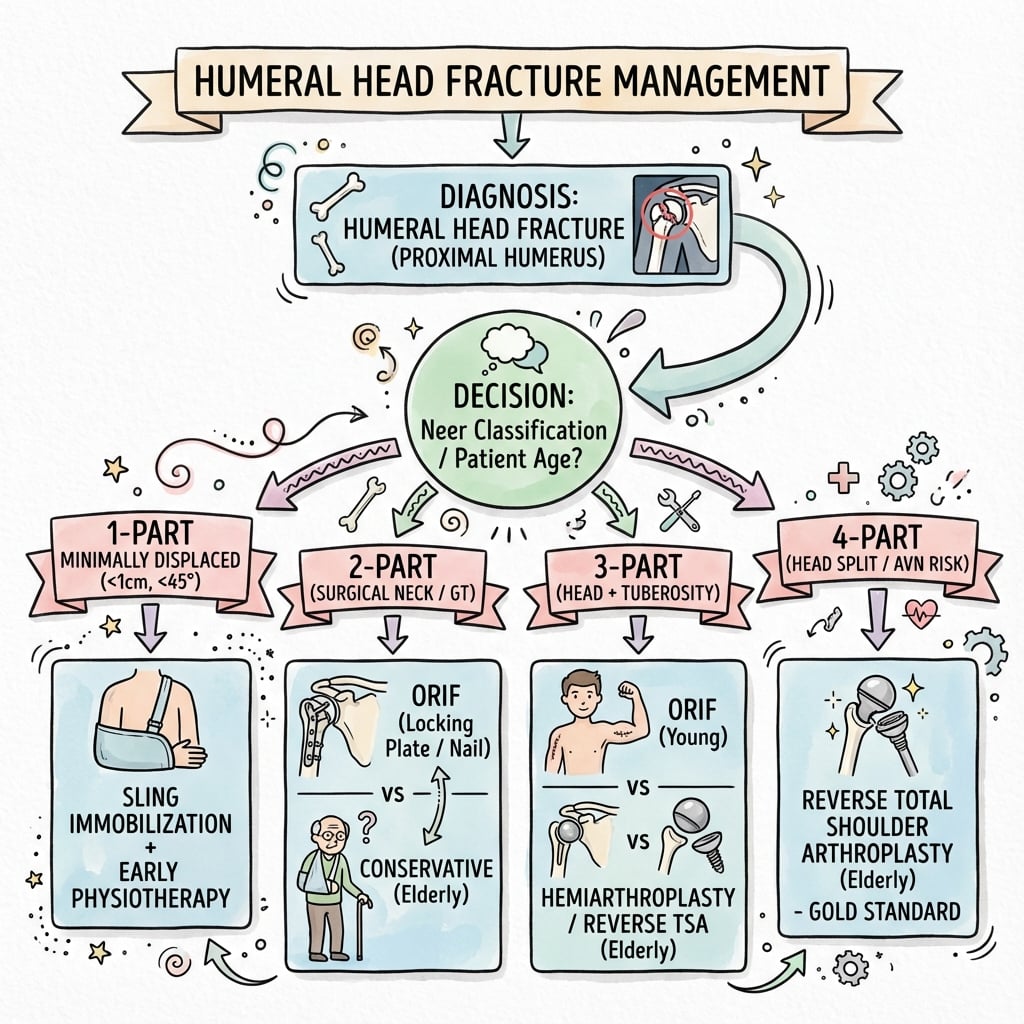
Treatment Decision Making
- Non-displaced fractures.
- Minimally displaced head splits (rarely stay reduced).
- Impression fractures less than 20%.
- Low demand / Medical contraindications.
- Sling 2-4 weeks.
- Early passive motion (prevent stiffness).
- Monitor for displacement (X-ray weekly).
Accepts risk of post-traumatic arthritis.
Surgical Technique
Operative fixation
Indication: Young patient, Head Split.
- Approach: Deltopectoral.
- Reduction: Open book tuberosities to see joint. Clamp head fragments.
- Fixation: 3.0mm or 4.0mm Headless Compression Screws (Herbert).
- Placement: Buried beneath articular cartilage (must be sub-flush).
- Suture: Repair tuberosities/cuff over the construct.
Meticulous technique required to avoid screw cutout.
HEADSurgical Goals
Hook:Keep your HEAD in the game: Restore anatomy or Replace it.
Tuberosity Reconstruction in Fracture Arthroplasty
The topic repeatedly states that "tuberosity healing improves rotation" and a viva explicitly asks "how do you secure the tuberosities?" - yet the technique and its importance are never developed. This is the step that most determines the functional result of arthroplasty done for a head fracture.
Why it matters. When the head is replaced for a comminuted fracture, the greater and lesser tuberosities (carrying the rotator cuff) are free fragments that must be reattached and must heal as bone for the cuff to work. In the randomised data cited in this topic, only about 57-65% of tuberosities healed, and crucially the functional outcome of a hemiarthroplasty depended on tuberosity healing, whereas a reverse arthroplasty performed well even when the tuberosities failed (its deltoid-driven mechanics do not rely on the cuff). That single contrast is the core reason RTSA has overtaken hemiarthroplasty for the elderly fracture.
- Detail
- A low-profile, often porous/grafted metaphysis lets the tuberosities sit against bone-friendly metal at the correct height and version
- Detail
- Greater tuberosity posterolateral and lesser tuberosity anteromedial, both BELOW the head/articular margin and reduced to the shaft - restore height and retroversion
- Detail
- Horizontal sutures encircling the stem PLUS vertical sutures from the shaft through the tuberosities and cuff ('tension-band' style) - a cable/suture cage
- Detail
- Autogenous cancellous bone graft (from the resected head) packed behind the tuberosities to promote union
- Detail
- Too-high a head or malreduced tuberosities prevents healing and blocks rotation
Consequence of failure. Tuberosity nonunion or resorption gives a poor result: loss of active external rotation and elevation, and - in a hemiarthroplasty - anterosuperior escape of the prosthetic head. Because RTSA tolerates this far better, it is the safer choice when the tuberosities are badly comminuted or osteoporotic. (Generic RTSA technique and complications such as notching are covered in reverse-total-shoulder-arthroplasty.)
Secure the tuberosities anatomically to bone, at the right height/version, with a horizontal-plus-vertical suture cage around a fracture stem and cancellous graft behind them. State the killer fact: hemiarthroplasty function depends on the tuberosities healing (only ~60% do), whereas reverse arthroplasty works even if they fail - which is exactly why RTSA is preferred in the comminuted, osteoporotic, cuff-poor elderly fracture.
SIZEImpression Fracture Sizing
Hook:Use the SIZE of the defect to determine treatment.
Complications
Potential Complications
Major Risk: Ischemia leads to head collapse. Rate is greater than 50% for displaced head splits. Leads to screw cutout and joint destruction.
Cartilage Damage: Even with healing, the articular damage leads to rapid arthrosis. May require future conversion to arthroplasty.
Tuberosity Failure: In both ORIF and Arthroplasty, if tuberosities don't heal, function is poor (loss of active elevation/rotation).
Frozen Shoulder: Scarring and pain limit motion. Early rehab is balanced against fixation stability.
Postoperative Care
Rehabilitation Protocol
- Sling immobilization.
- Pendulums only.
- Elbow/Wrist/Hand ROM.
- Supine passive forward elevation.
- External rotation restricted (protect subscap/tuberosities).
- Pulley exercises.
- Wean sling.
- AAROM (Wand exercises).
- Hydrotherapy.
- X-ray check for AVN/Collapse.
- Cuff strengthening.
- Scapular stabilizers.
- Return to non-contact activity.
Outcomes
Prognosis
- ORIF: High reoperation rate (20-30%) due to hardware removal or AVN conversion. Good function if reduction maintained and AVN avoided.
- RTSA: Reliable pain relief (90%). Active elevation greater than 130 degrees. Rotation depends on tuberosity healing.
- Hemiarthroplasty: variable pain relief (depends on glenoid wear). Good option if glenoid is pristine, but RTSA is surpassing it for reliability.
Guidelines, Registries & Global Practice
Head-splitting and impression fractures are rare, so almost no dedicated guideline addresses them directly; recommendations are extrapolated from the broader proximal humeral fracture literature, which is dominated by surgical-neck patterns.
Global epidemiology
- Proximal humeral fractures are the third most common fragility fracture after hip and distal radius, with a strongly bimodal distribution (young high-energy, elderly low-energy osteoporotic).
- True head-splitting fractures represent a small minority of proximal humeral injuries; isolated impression fractures are usually a feature of locked dislocations (anterior dislocation produces a Hill-Sachs lesion; posterior dislocation produces a reverse Hill-Sachs).
- Position relevant to head fractures
- Inconclusive/limited evidence for most operative vs non-operative decisions; emphasises shared decision-making and individualized care
- Position relevant to head fractures
- Early senior assessment, CT for intra-articular or complex patterns, and timely referral of reconstructable injuries to specialist upper-limb units
- Position relevant to head fractures
- Classifies articular involvement as 11-C; recommends CT for surgical planning and head-preserving fixation only where vascularity and bone stock permit
- Position relevant to head fractures
- Supports reverse arthroplasty over hemiarthroplasty in elderly non-reconstructable fractures, reflecting RCT and registry data
Registry evidence
- Multiple national arthroplasty registries (AOANJRR, NJR, the Nordic registries) document a marked shift from hemiarthroplasty to reverse total shoulder arthroplasty for fracture indications in patients over 65, with better implant survivorship and lower revision rates for RSA than fracture hemiarthroplasty.
- Registry data consistently show that fracture is a higher-risk arthroplasty indication than elective osteoarthritis, reinforcing careful patient selection.
High- vs limited-resource practice variation
- High-resource settings: routine CT with 3D reconstruction, ready access to headless compression screws, osteoarticular allograft, and modular reverse arthroplasty systems.
- Limited-resource settings: reliance on plain radiographs, greater use of non-operative management or hemiarthroplasty where reverse systems or allograft are unavailable, and selective referral of young reconstructable head splits to tertiary centres.
- Long-term surveillance for AVN and post-traumatic arthritis (clinical and radiographic, typically to 2 years) is recommended wherever feasible.
Controversies and Areas of Uncertainty
No randomized data exist for head-splitting fractures. Joint preservation is favoured in patients under 50 to avoid lifelong arthroplasty constraints, but reported AVN and reoperation rates after ORIF are high. The threshold of age, comminution and bone quality at which replacement becomes preferable is undefined.
RCT (Sebastia-Forcada) and registry data favour reverse arthroplasty for elderly non-reconstructable fractures, yet hemiarthroplasty may still suit younger patients with intact cuff and reconstructable tuberosities. Long-term durability of reverse implants in this group remains uncertain.
The classic cut-offs (under 20% ignore, 20-40% transfer/graft, over 40% arthroplasty/allograft) are based on small series and biomechanical reasoning, not high-level evidence. Engagement during functional motion may matter more than absolute percentage.
Hertel criteria predict intraoperative ischemia, but ischemia does not always progress to symptomatic collapse, and revascularization can occur. Whether a high Hertel score alone should mandate primary replacement is debated.
MCQ Practice
Self-Assessment Questions
Q: Which artery provides the primary blood supply to the humeral head and is most at risk in anatomical neck fractures?
- A) Posterior Humeral Circumflex artery
- B) Anterior Humeral Circumflex artery (Arcuate branch)
- C) Suprascapular artery
- D) Thoracoacromial artery
- E) Subscapular artery
A: B - The arcuate branch of the Anterior Humeral Circumflex Artery ascends in the bicipital groove and enters the head intra-articularly. It is most commonly disrupted in anatomical neck fractures.
Q: According to Hertel, which factor is the strongest predictor of humeral head ischemia?
- A) Age greater than 60
- B) Medial hinge less than 8mm
- C) 4-part fracture pattern
- D) Head split component
- E) Tuberosity displacement greater than 1cm
A: B - A medial metaphyseal head extension (medial hinge) of less than 8mm is the strongest predictor of ischemia due to disruption of the posterior circumflex contribution.
Q: What is the preferred treatment for a displaced head-splitting fracture in a 75-year-old active patient?
- A) Non-operative treatment
- B) ORIF with locking plate
- C) Hemiarthroplasty
- D) Reverse Total Shoulder Arthroplasty
- E) Resection Arthroplasty
A: D - RTSA is preferred in the elderly with head-splitting fractures due to the high failure rate of ORIF (AVN/Cutout) and the unreliability of Hemiarthroplasty (tuberosity healing/cuff function).
Q: A 'Reverse Hill-Sachs' lesion is associated with which direction of shoulder instability?
- A) Anterior
- B) Posterior
- C) Inferior (Luxatio Erecta)
- D) Multidirectional
- E) Superior
A: B - A Reverse Hill-Sachs lesion is an impression fracture on the anteromedial aspect of the humeral head, caused by impaction against the posterior glenoid rim during a Posterior dislocation.
Q: When fixing a head-split fracture in a young patient, which implant minimizes articular damage?
- A) 4.5mm Cortical Screws
- B) 3.5mm Locking Screws
- C) Headless Compression Screws (Herbert)
- D) K-wires
- E) Suture Buttons
A: C - Buried Headless Compression Screws are designed to be sunk below the cartilage surface, providing compression across the split without prominence that would damage the glenoid.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You see a 75-year-old female with a comminuted humeral head splitting fracture. The tuberosities are also fractured. What is your management plan?”
“A 30-year-old male has a 40% impression fracture of the anterior humeral head (Reverse Hill-Sachs) after a seizure. It engages. Options?”
“Explain the Hertel Criteria for predicting AVN.”
Key Facts
- Def: Articular involvement (Split/Impression)
- Risk: AVN (Arcuate artery)
- Predictor: Hertel less than 8mm hinge
- Assoc: Posterior dislocation (Impression)
- Salvage: RTSA in elderly
Surgical Steps (ORIF)
- Deltopectoral approach
- Open book tuberosities
- Reduce head fragments (Clamps)
- Buried Headless Screws
- Reattach Tuberosities
Common Pitfalls
- Missing the head split on X-ray (Get CT)
- Prominent hardware in joint
- Using Hemi in cuff-deficient elderly
- Ignoring posterior instability
Examiner Favorites
- Hertel criteria for AVN
- Blood supply to head
- Reverse vs Hemi decision
- Management of missed posterior dislocation
Evidence Base
Key Studies
Hertel et al. - Predictors of Humeral Head Ischemia
- Prospective study of 100 intracapsular proximal humerus fractures with intraoperative perfusion assessment
- Best predictors: metaphyseal head extension under 8mm (accuracy 0.84), disrupted medial hinge (0.79), and basic fracture pattern (0.70)
- Combination of anatomical neck fracture, short calcar and disrupted hinge gave positive predictive value up to 97% for ischemia
Sebastia-Forcada et al. - RSA vs Hemiarthroplasty (RCT)
- Blinded RCT of 62 patients over 70 years with complex fractures: reverse arthroplasty (n=31) vs hemiarthroplasty (n=31)
- RSA gave significantly higher UCLA (29.1 vs 21.1) and Constant (56.1 vs 40.0) scores and better forward elevation (120 vs 80 degrees)
- RSA had a lower revision rate; 6 hemiarthroplasties needed revision to RSA for proximal migration, and HA function depended on tuberosity healing
Gerber and Lambert - Allograft Reconstruction for Locked Posterior Dislocation
- Four chronic locked posterior dislocations with anteromedial head defects over 40% reconstructed with femoral head allograft
- Stability restored and maintained in all four at mean 68 months; three reported little or no pain
- Lesser tuberosity transfer (McLaughlin) is recommended for smaller defects; arthroplasty traditionally preferred for very large defects
Solberg et al. - Locked Plating vs Hemiarthroplasty
- Comparative series of 3- and 4-part fractures in patients 55 years and older: locked plate (n=38) vs hemiarthroplasty (n=48)
- Locked plating gave higher Constant scores (68.6 vs 60.6) despite a higher complication rate, with the advantage greatest in 3-part fractures
- Osteonecrosis (6) and screw perforation (6) were common; loss of fixation occurred only with over 20 degrees of initial varus angulation
PROFHER Trial - Surgery vs Non-operative Treatment
- Multicentre RCT of 250 adults with displaced surgical-neck fractures: surgery vs sling immobilisation
- No significant difference in Oxford Shoulder Score over 2 years (39.1 vs 38.3) and no difference in complications or secondary surgery
- Results do not support the trend toward increased surgery; the trial explicitly excluded head-splitting fractures
Handoll and Brorson - Cochrane Review
- Systematic review of 31 RCTs (1941 participants) of proximal humeral fracture management
- High/moderate-quality evidence of no benefit of surgery over non-operative care for most displaced neck fractures, with more reoperations after surgery
- Explicitly notes the evidence does NOT cover head-splitting fractures, fracture-dislocations, or fractures in young patients