Parathyroid Hormone Deficiency | Hypocalcemia | Tetany | Basal Ganglia Calcification
HYPOPARATHYROIDISM CAUSES
Critical Must-Knows
- Biochemistry: Low calcium AND low PTH (distinguishes from vitamin D deficiency)
- Tetany triad: Carpopedal spasm, Chvostek sign, Trousseau sign (neuromuscular irritability)
- Emergency: Severe hypocalcemia (Ca less than 1.8) causes seizures, laryngospasm, cardiac arrhythmias
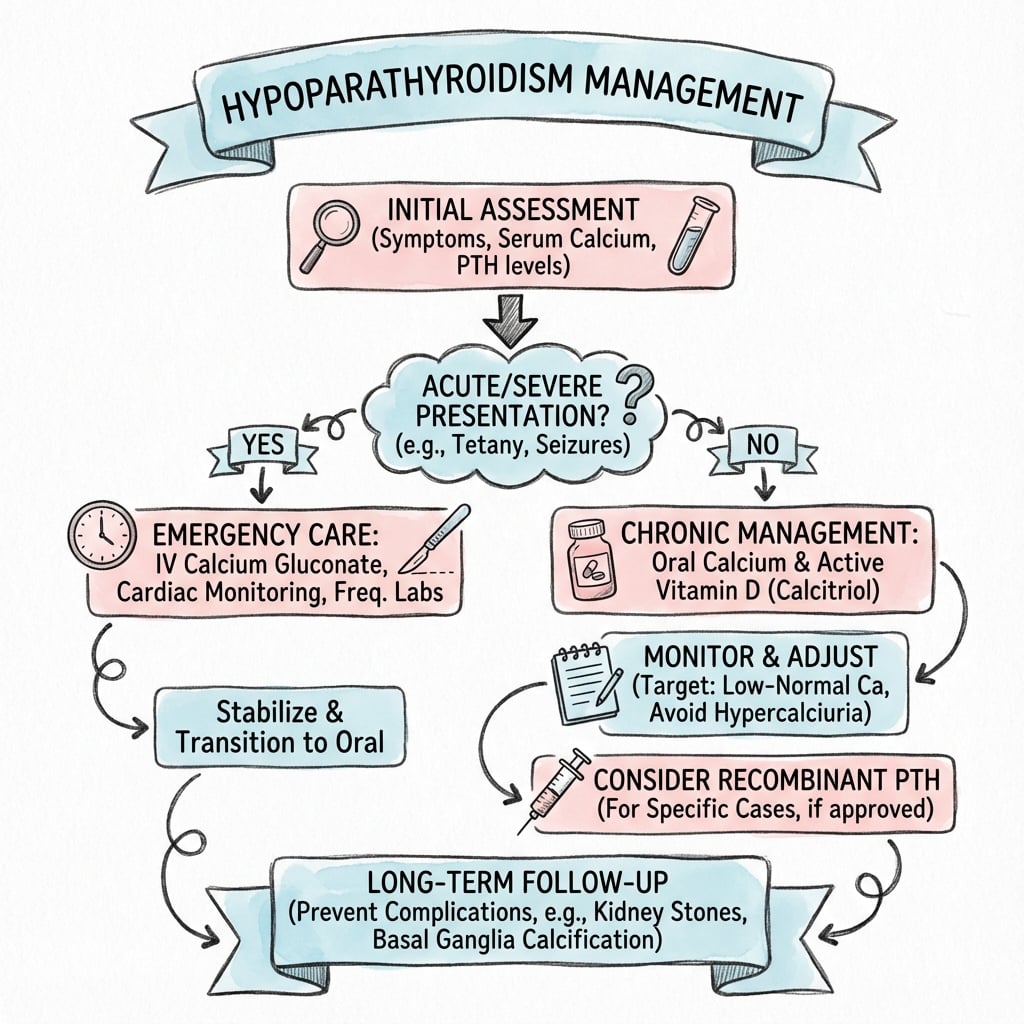
- Treatment: IV calcium gluconate for acute, oral calcium carbonate plus calcitriol for chronic
- Orthopaedic relevance: Basal ganglia calcification, increased bone density, perioperative complications
Clinical Pearls
- "Low calcium WITH low PTH distinguishes hypoparathyroidism from vitamin D deficiency or malabsorption
- "Chvostek sign is facial twitching when tapping facial nerve; Trousseau is carpopedal spasm with BP cuff inflation
- "Post-thyroidectomy hypocalcemia may be transient (temporary ischemia) or permanent (gland removal)
- "Basal ganglia calcification on CT is characteristic finding in chronic hypoparathyroidism
Clinical Imaging
Imaging Gallery

Critical Hypoparathyroidism Exam Points
Biochemical Diagnosis Is Key
Hypoparathyroidism: Low calcium (less than 2.0 mmol/L) AND low PTH (distinguishes from vitamin D deficiency or malabsorption where PTH is elevated). High phosphate is characteristic. Always check magnesium as hypomagnesemia causes functional hypoparathyroidism.
Tetany Is Life-Threatening
Neuromuscular irritability from hypocalcemia causes carpopedal spasm, perioral numbness, and muscle cramps. Severe cases cause laryngospasm (stridor, airway obstruction), seizures (generalized tonic-clonic), and cardiac arrhythmias (prolonged QT, torsades). Requires urgent IV calcium.
Post-Surgical Hypocalcemia
After thyroid/parathyroid surgery: Check calcium daily for 48-72 hours. Transient hypocalcemia (temporary ischemia) recovers in 6 months. Permanent hypoparathyroidism (gland removal) needs lifelong replacement. Risk increased with central neck dissection, reoperative surgery.
Perioperative Management Critical
For orthopaedic surgery: Optimize calcium preoperatively (target 2.0-2.2 mmol/L lower limit normal). Monitor calcium postoperatively if NPO prolonged. Avoid hyperventilation (alkalosis increases protein binding, lowers ionized calcium). Have IV calcium available.
CATS GO NUMBCATS GO NUMB - Hypocalcemia Clinical Features
| C | Convulsions Seizures from severe hypocalcemia (neuronal irritability) |
| A | Arrhythmias Prolonged QT interval, torsades de pointes, cardiac arrest |
| T | Tetany Carpopedal spasm, muscle cramps, neuromuscular irritability |
| S | Spasm Laryngospasm (stridor), bronchospasm (wheezing) |
| G | Gastrointestinal Abdominal cramps, diarrhea (rare) |
| O | Ocular Cataracts (chronic hypocalcemia, subcapsular) |
| N | Neuropsychiatric Anxiety, depression, irritability, cognitive impairment |
| U | Urine Hypocalciuria (low urine calcium, opposite of hyperparathyroidism) |
| M | Muscle weakness Proximal myopathy, fatigue |
| B | Basal ganglia calcification Parkinsonism, chorea, dystonia (chronic cases) |
| C | Convulsions Seizures from severe hypocalcemia (neuronal irritability) | S | Spasm Laryngospasm (stridor), bronchospasm (wheezing) | N | Neuropsychiatric Anxiety, depression, irritability, cognitive impairment | B | Basal ganglia calcification Parkinsonism, chorea, dystonia (chronic cases) |
| A | Arrhythmias Prolonged QT interval, torsades de pointes, cardiac arrest | G | Gastrointestinal Abdominal cramps, diarrhea (rare) | U | Urine Hypocalciuria (low urine calcium, opposite of hyperparathyroidism) | ||
| T | Tetany Carpopedal spasm, muscle cramps, neuromuscular irritability | O | Ocular Cataracts (chronic hypocalcemia, subcapsular) | M | Muscle weakness Proximal myopathy, fatigue |
Hook:CATS GET low calcium and GO NUMB - think tetany, seizures, arrhythmias!
PTH ABSENTPTH ABSENT - Effects of PTH Deficiency
| P | Phosphate elevated Loss of renal phosphate excretion (PTH normally promotes phosphaturia) |
| T | Tetany Neuromuscular irritability from low ionized calcium |
| H | Hypocalcemia Reduced bone calcium release and reduced renal calcium reabsorption |
| A | Alkaline phosphatase low Reduced bone turnover (opposite of hyperparathyroidism) |
| B | Bone density increased Paradoxically denser bones (reduced remodeling) |
| S | Subcapsular cataracts Chronic hypocalcemia causes lens calcium deposition |
| E | ECG changes Prolonged QT interval (risk of torsades de pointes) |
| N | Neurologic calcification Basal ganglia calcification on CT (50% of chronic cases) |
| T | Treatment needed Calcium and activated vitamin D (calcitriol) lifelong |
| P | Phosphate elevated Loss of renal phosphate excretion (PTH normally promotes phosphaturia) | A | Alkaline phosphatase low Reduced bone turnover (opposite of hyperparathyroidism) | E | ECG changes Prolonged QT interval (risk of torsades de pointes) |
| T | Tetany Neuromuscular irritability from low ionized calcium | B | Bone density increased Paradoxically denser bones (reduced remodeling) | N | Neurologic calcification Basal ganglia calcification on CT (50% of chronic cases) |
| H | Hypocalcemia Reduced bone calcium release and reduced renal calcium reabsorption | S | Subcapsular cataracts Chronic hypocalcemia causes lens calcium deposition | T | Treatment needed Calcium and activated vitamin D (calcitriol) lifelong |
Hook:When PTH is ABSENT, calcium drops, phosphate rises, and bones paradoxically get denser!
CHVOSTEK TROUSSEAUCHVOSTEK TROUSSEAU - Tetany Examination
| C | Chvostek sign Facial twitching when tapping facial nerve anterior to ear (CN VII) |
| H | Hyperreflexia Brisk deep tendon reflexes from neuromuscular irritability |
| V | Visible spasm Carpopedal spasm with wrist flexion and finger extension |
| O | Obstetrician hand Classic position in carpopedal spasm (adducted thumb) |
| T | Trousseau sign Carpopedal spasm induced by BP cuff inflation above systolic for 3 min |
| R | Reflex irritability Increased neuromuscular excitability |
| O | Oral perioral numbness Tingling around mouth, lips (early symptom) |
| U | Ulnar nerve tapping Can elicit hand muscle twitching |
| C | Chvostek sign Facial twitching when tapping facial nerve anterior to ear (CN VII) | O | Obstetrician hand Classic position in carpopedal spasm (adducted thumb) | O | Oral perioral numbness Tingling around mouth, lips (early symptom) |
| H | Hyperreflexia Brisk deep tendon reflexes from neuromuscular irritability | T | Trousseau sign Carpopedal spasm induced by BP cuff inflation above systolic for 3 min | U | Ulnar nerve tapping Can elicit hand muscle twitching |
| V | Visible spasm Carpopedal spasm with wrist flexion and finger extension | R | Reflex irritability Increased neuromuscular excitability |
Hook:CHVOSTEK (face) and TROUSSEAU (hand) are the two classic tetany signs - test both in suspected hypocalcemia!
Overview and Epidemiology
Hypoparathyroidism is a disorder of insufficient parathyroid hormone (PTH) secretion, leading to hypocalcemia, hyperphosphatemia, and disrupted calcium homeostasis. Unlike the more common secondary hyperparathyroidism (elevated PTH from chronic hypocalcemia), hypoparathyroidism is characterized by inappropriately low or absent PTH in the setting of hypocalcemia.
Epidemiology:
- Prevalence: 70,000-90,000 cases in the United States (rare disorder)
- Post-surgical: 75% of cases are iatrogenic following thyroid or parathyroid surgery
- Permanent post-thyroidectomy: 1-2% of total thyroidectomies, higher after reoperative or central neck dissection (up to 10%)
- Autoimmune: 15-20% of cases, often part of polyglandular syndrome
- Genetic/congenital: 5-10%, includes DiGeorge syndrome
Why Hypoparathyroidism Matters to Orthopaedics
Hypoparathyroidism causes perioperative complications (hypocalcemic seizures, arrhythmias if calcium not optimized), basal ganglia calcification leading to movement disorders (extrapyramidal symptoms), and paradoxically increased bone density (reduced remodeling). Recognition is critical for preoperative optimization and avoiding metabolic crises during surgery.
Physiology and Pathophysiology
PTH Physiology Review
Normal PTH functions:
PTH Effects on Target Organs (Absent in Hypoparathyroidism)
| Organ | Normal PTH Action | Effect of PTH Deficiency | Result |
|---|---|---|---|
| Bone | Activates osteoclasts (calcium release) | Reduced bone resorption | Paradoxically increased bone density, low turnover |
| Kidney (proximal tubule) | Promotes phosphate excretion | Phosphate retention | Hyperphosphatemia (elevated serum phosphate) |
| Kidney (distal tubule) | Increases calcium reabsorption | Reduced calcium reabsorption | Hypocalcemia, hypocalciuria |
| Kidney (1-alpha hydroxylase) | Activates vitamin D to calcitriol | Reduced active vitamin D | Impaired intestinal calcium absorption |
Net result of PTH deficiency: Low serum calcium, high serum phosphate, low urine calcium
Causes of Hypoparathyroidism
Post-Surgical Hypoparathyroidism (75% of cases)
Mechanisms:
- Gland removal: Inadvertent excision during thyroidectomy, parathyroidectomy for hyperparathyroidism, radical neck dissection
- Vascular injury: Devascularization of parathyroid glands during surgery (temporary or permanent)
- Autotransplantation failure: Intentional autotransplantation may not engraft successfully
Risk factors for permanent hypoparathyroidism:
- Total thyroidectomy (higher than hemithyroidectomy)
- Central lymph node dissection (thyroid cancer)
- Reoperative surgery (scar tissue, difficult dissection)
- Parathyroid not identified/preserved during surgery
- Concurrent parathyroid pathology
Time course:
- Transient: Symptoms develop within 24-72 hours post-op, resolve within 6 months (temporary ischemia or stunning)
- Permanent: Symptoms persist beyond 6 months, require lifelong replacement
Surgeons monitor calcium postoperatively and supplement as needed during recovery period.
Pathophysiology of Hypocalcemia
Hypocalcemia mechanisms:
Reduced Calcium Mobilization
- Bone: Absent PTH-mediated osteoclast activation
- Calcium remains sequestered in bone
- Bone density paradoxically increases (reduced remodeling)
- Low bone turnover state (low alkaline phosphatase)
Reduced Calcium Absorption
- Kidney: Decreased renal calcium reabsorption (DCT)
- Intestine: Reduced active vitamin D (calcitriol) synthesis
- Impaired intestinal calcium absorption despite low serum calcium
- Result: Net calcium loss
Hyperphosphatemia mechanism:
- PTH normally promotes renal phosphate excretion via inhibition of sodium-phosphate cotransporter in proximal tubule
- Absent PTH leads to phosphate retention
- High serum phosphate further suppresses 1-alpha hydroxylase (worsens vitamin D activation)
Neuromuscular effects:
- Ionized calcium is critical for normal neuron and muscle function
- Low calcium reduces action potential threshold (increased neuronal excitability)
- Results in tetany, seizures, and cardiac conduction abnormalities
Clinical Assessment
Acute Hypocalcemia Presentation
Life-Threatening Manifestations
Severe hypocalcemia (Ca less than 1.8 mmol/L) is a medical emergency. Laryngospasm causes stridor and potential airway obstruction. Seizures (tonic-clonic) can occur without warning. Cardiac arrhythmias (prolonged QT, torsades de pointes, ventricular fibrillation) may be fatal. Immediate IV calcium gluconate is required.
Neuromuscular irritability (tetany):
- Carpopedal spasm: Most characteristic finding - wrist flexion with finger extension and thumb adduction (obstetrician hand position)
- Perioral paresthesias: Tingling or numbness around mouth and lips (often earliest symptom)
- Muscle cramps: Painful cramps in hands, feet, back, legs
- Laryngospasm: Sensation of throat tightness, stridor (high-pitched inspiratory sound)
- Seizures: Generalized tonic-clonic seizures without focal features
Cardiovascular:
- Prolonged QT interval: ECG shows QTc over 450 ms (males) or 470 ms (females)
- Heart failure: Rarely, severe chronic hypocalcemia causes dilated cardiomyopathy
- Arrhythmias: Torsades de pointes, ventricular tachycardia/fibrillation
Neuropsychiatric:
- Anxiety, irritability
- Depression
- Cognitive impairment, confusion
- Psychosis (rare)
Physical Examination Signs
Classic Hypocalcemia Signs
| Sign | Technique | Positive Finding | Sensitivity |
|---|---|---|---|
| Chvostek sign | Tap facial nerve 2 cm anterior to ear lobe | Ipsilateral facial muscle twitching (orbicularis oculi, nasalis) | 70% in hypocalcemia (10% false positive in normals) |
| Trousseau sign | Inflate BP cuff 20 mmHg above systolic for 3 minutes | Carpopedal spasm (wrist flexion, finger extension, thumb adduction) | 94% in hypocalcemia (more specific than Chvostek) |
| Peroneal nerve sign | Tap peroneal nerve at fibular head | Foot dorsiflexion and toe extension | Less commonly tested but present in severe cases |
Trousseau vs Chvostek Specificity
Trousseau sign is more specific (94% sensitivity, low false positive) than Chvostek sign (70% sensitivity, 10% false positive in normocalcemic individuals). If testing for hypocalcemia, Trousseau is preferred. However, both may be negative in very severe hypocalcemia (muscle weakness prevents spasm) or chronic cases with adaptation.
Chronic Hypoparathyroidism Manifestations
Skeletal:
- Increased bone mineral density: Paradoxical finding (DEXA shows high T-scores)
- Reduced bone turnover: Low alkaline phosphatase, low bone formation markers
- Abnormal bone quality: Despite high density, may have impaired bone strength (static bone disease)
Neurological:
- Basal ganglia calcification: Present in 50% of chronic cases on CT brain
- Extrapyramidal symptoms: Parkinsonism (tremor, rigidity, bradykinesia), chorea, dystonia
- Papilledema: Rare, from increased intracranial pressure (pseudotumor cerebri)
- Seizures: Recurrent seizures if calcium not well controlled
Ophthalmologic:
- Cataracts: Subcapsular cataracts (posterior subcapsular) from chronic hypocalcemia
- Lens calcium deposition: Visible on slit lamp examination
Dental:
- Enamel hypoplasia: If hypoparathyroidism present during tooth development (childhood)
- Delayed tooth eruption: In congenital cases
- Dental caries: Increased risk
Dermatologic:
- Dry, coarse skin
- Brittle nails
- Hair loss (alopecia)
Biochemical and Imaging Investigations
Biochemistry
Biochemical Profiles in Hypocalcemia
| Condition | Calcium | PTH | Phosphate | Vitamin D |
|---|---|---|---|---|
| Hypoparathyroidism | Low (less than 2.0) | Low or undetectable | High (over 1.5) | Low calcitriol, normal 25-OH |
| Vitamin D deficiency | Low | High (appropriate) | Low/normal | Low 25-OH vitamin D |
| Chronic kidney disease | Low | High (secondary HPT) | High | Low calcitriol (impaired 1-alpha hydroxylase) |
| Pseudohypoparathyroidism | Low | High (PTH resistance) | High | Normal/low |
| Hypomagnesemia | Low | Low (functional hypoparathyroidism) | Variable | Normal |
Key diagnostic tests:
Serum calcium (total and ionized):
- Total calcium: Less than 2.0 mmol/L indicates hypocalcemia (normal 2.2-2.5)
- Ionized calcium: More accurate (not affected by albumin); less than 1.1 mmol/L is abnormal
- Correct for albumin: Corrected Ca = measured Ca + 0.02 x (40 - albumin in g/L)
Parathyroid hormone (PTH):
- Inappropriately low or undetectable in setting of hypocalcemia
- Normal PTH in hypocalcemia is inappropriate (should be elevated)
- Intact PTH assay is standard
Serum phosphate:
- Elevated (over 1.5 mmol/L; normal 0.8-1.5) due to lack of PTH-mediated renal excretion
- Hyperphosphatemia is characteristic of hypoparathyroidism
25-OH vitamin D:
- Usually normal in hypoparathyroidism (distinguishes from vitamin D deficiency)
- If low, suggests concurrent vitamin D deficiency requiring separate treatment
1,25-dihydroxy vitamin D (calcitriol):
- Low despite hypocalcemia (PTH normally stimulates 1-alpha hydroxylase)
- Not routinely measured but explains need for calcitriol supplementation
Magnesium:
- Must check - hypomagnesemia (less than 0.7 mmol/L) causes functional hypoparathyroidism
- Magnesium deficiency impairs PTH secretion and PTH action
- Correct magnesium before diagnosing true hypoparathyroidism
Alkaline phosphatase:
- Normal or low (reduced bone turnover, opposite of hyperparathyroidism)
24-hour urine calcium:
- Low (hypocalciuria) due to reduced filtered load despite reduced renal reabsorption
- Distinguishes from other causes of hypocalcemia
Electrocardiography
ECG findings:
- Prolonged QT interval (QTc over 450-470 ms) - most characteristic finding
- Prolonged ST segment: Increases QT duration
- T wave changes: May be flattened or inverted
- Arrhythmias: Torsades de pointes (polymorphic VT with prolonged QT), ventricular fibrillation
QT Prolongation and Sudden Death Risk
Prolonged QT interval (QTc over 500 ms) significantly increases risk of torsades de pointes (twisting of the points - polymorphic VT) and sudden cardiac death. Avoid QT-prolonging medications (antiarrhythmics, antipsychotics, antibiotics). Monitor ECG when correcting calcium. Severe cases may require temporary pacing.
Imaging
CT brain (non-contrast):
- Basal ganglia calcification: Bilateral symmetric calcification of globus pallidus, putamen, caudate (50% of chronic cases)
- Dentate nuclei calcification: Cerebellar calcification
- Calcification correlates with duration and severity of hypocalcemia, not always symptomatic
DEXA bone density scan:
- Increased bone mineral density: Paradoxical finding (T-scores often +2 to +4 SD above normal)
- Z-scores more relevant (compare to age-matched controls)
- High density does not equal normal bone quality (low turnover state)
Parathyroid imaging (if etiology unclear):
- Ultrasound neck to assess for parathyroid tissue (may show atrophic or absent glands)
- Sestamibi scan not useful (requires functioning parathyroid tissue)
Acute and Chronic Management
Acute Hypocalcemia Management
Severe Symptomatic Hypocalcemia (Medical Emergency)
Indications for IV calcium:
- Ionized calcium less than 1.0 mmol/L (total Ca less than 1.8)
- Tetany, carpopedal spasm
- Seizures
- Laryngospasm, stridor
- Cardiac arrhythmias, prolonged QT
Immediate treatment:
Step 1: IV calcium gluconate
- Loading dose: 10-20 mL of 10% calcium gluconate (90-180 mg elemental calcium) IV over 10 minutes
- Continuous infusion: 50-100 mL calcium gluconate in 500 mL D5W or normal saline, run at 50 mL/hour (adjust to maintain calcium)
- Monitoring: Continuous cardiac monitoring (watch for bradycardia if infused too rapidly), check ionized calcium every 2-4 hours initially
Caution: IV calcium can cause bradycardia if infused too quickly, extravasation causes tissue necrosis (ensure good IV access), incompatible with bicarbonate (precipitates)
Step 2: Address underlying cause
- Check and correct magnesium if low (magnesium sulfate 2 g IV over 15 min, then 1-2 g/hour infusion)
- Start oral calcium and calcitriol (see chronic management) once patient stable
Step 3: Airway management if laryngospasm
- High-flow oxygen
- Heliox (helium-oxygen mixture) may relieve stridor
- Emergent intubation if complete airway obstruction
This is life-saving treatment requiring ICU monitoring.
Chronic Hypoparathyroidism Management
Goals:
- Maintain serum calcium in low-normal range (2.0-2.2 mmol/L)
- Avoid hypercalciuria (keep urine calcium less than 300 mg/24hr)
- Prevent long-term complications (nephrolithiasis, nephrocalcinosis, basal ganglia calcification)
- Maintain quality of life
Calcium supplementation:
- Calcium carbonate: 1-3 g elemental calcium daily (divided doses with meals)
- Calcium citrate: Alternative if poor gastric acid (does not require acid for absorption)
- Titrate dose based on serum calcium and urine calcium
Activated vitamin D (essential):
- Calcitriol (1,25-dihydroxy vitamin D): 0.25-1 mcg twice daily
- Direct active form (bypasses need for PTH-mediated activation)
- More potent than cholecalciferol or ergocalciferol
- Risk of hypercalciuria (monitor 24-hour urine calcium)
Thiazide diuretics (adjunct):
- Hydrochlorothiazide: 25-50 mg daily
- Increases renal calcium reabsorption (reduces urine calcium)
- Useful if hypercalciuria develops despite dose optimization
- Caution: May cause hypokalemia, monitor electrolytes
Recombinant human PTH (rhPTH 1-84):
- Teriparatide or rhPTH 1-84: Subcutaneous injection
- Reserved for refractory cases not controlled on standard therapy
- Expensive, not widely available
- Improves calcium control and may reduce calcium/calcitriol requirements
Magnesium:
- Replace if deficient (oral magnesium oxide 400-800 mg daily)
- Necessary for PTH secretion and action
Monitoring schedule:
Chronic Hypoparathyroidism Monitoring
| Test | Frequency | Target | Action if Abnormal |
|---|---|---|---|
| Serum calcium | Every 1-3 months when stable | 2.0-2.2 mmol/L (low-normal) | Adjust calcium or calcitriol dose |
| Serum phosphate | Every 3-6 months | Within normal range (less than 1.5) | High phosphate suggests overtreatment |
| 24-hour urine calcium | Every 6-12 months | Less than 300 mg/day | Add thiazide if over 300, reduce calcium dose |
| Renal ultrasound | Annually or if hypercalciuria | No stones or nephrocalcinosis | Reduce calcium/calcitriol if stones develop |
| Serum creatinine | Every 6-12 months | Normal eGFR (over 60) | Reduce calcium load if renal impairment |
| Ophthalmology exam | Every 1-2 years | No cataracts | Cataract surgery if vision impaired |
Perioperative Considerations for Orthopaedic Surgery
Preoperative Optimization
Optimize Calcium Before Elective Surgery
Target serum calcium 2.0-2.2 mmol/L before elective orthopaedic surgery. Verify compliance with calcium and calcitriol. Check ionized calcium (more accurate than total calcium). Postpone elective surgery if calcium less than 1.9 mmol/L (risk of perioperative complications). Have IV calcium available in OR.
Preoperative assessment:
- Verify diagnosis: Review history, confirm on calcium/calcitriol replacement
- Check current calcium status: Serum total and ionized calcium, phosphate, magnesium
- ECG: Assess baseline QT interval (prolonged QT increases anesthetic risk)
- Medication review: Ensure patient taking medications, assess compliance
- Endocrinology consultation: For complex or poorly controlled cases
Medication management:
- Continue calcium and calcitriol on day of surgery if oral intake permitted
- If NPO prolonged (greater than 24 hours), may need IV calcium supplementation
Intraoperative Management
Monitoring:
- Continuous ECG monitoring for QT prolongation and arrhythmias
- Consider ionized calcium monitoring if prolonged case or significant fluid shifts
- Avoid rapid alkalosis (hyperventilation reduces ionized calcium by increasing protein binding)
Anesthetic considerations:
- Muscle relaxants: May have prolonged duration in hypocalcemia (monitor neuromuscular blockade)
- Citrated blood products: Large volume transfusion can chelate calcium (check ionized calcium)
- Hyperventilation: Avoid excessive hyperventilation (respiratory alkalosis decreases ionized calcium)
IV calcium availability:
- Have 10% calcium gluconate immediately available in OR
- If calcium drops or tetany/arrhythmia develops, give 10 mL IV calcium gluconate over 10 minutes
Postoperative Management
Monitoring:
- Check ionized calcium on arrival to recovery (especially if prolonged NPO or large fluid resuscitation)
- Continue cardiac monitoring if QT prolonged
- Resume oral calcium and calcitriol as soon as oral intake tolerated
Complications to watch for:
- Tetany: Carpopedal spasm, perioral numbness (check Trousseau/Chvostek signs)
- Seizures: Especially if calcium drops acutely
- Cardiac arrhythmias: Monitor for torsades de pointes if QT prolonged
IV to oral transition:
- If patient NPO prolonged postoperatively, may need IV calcium infusion temporarily
- Transition to oral once taking medications reliably
- Check calcium 24-48 hours after stopping IV calcium to ensure oral therapy adequate
Hypoparathyroidism in Spine Surgery
Hyperventilation during spine surgery (to reduce epidural venous bleeding) can precipitate hypocalcemic crisis in patients with hypoparathyroidism. Respiratory alkalosis increases calcium binding to albumin, lowering ionized calcium. Monitor ionized calcium intraoperatively if hyperventilating. Have IV calcium available. Avoid excessive hyperventilation.
Complications of Hypoparathyroidism
Acute and Chronic Complications
| Complication | Mechanism | Presentation | Management |
|---|---|---|---|
| Seizures | Neuronal hyperexcitability from low calcium | Generalized tonic-clonic seizures | IV calcium gluconate, anticonvulsants if recurrent |
| Laryngospasm | Vocal cord spasm from hypocalcemia | Stridor, respiratory distress, airway obstruction | IV calcium, heliox, emergent intubation if severe |
| Cardiac arrhythmias | Prolonged QT interval, altered repolarization | Torsades de pointes, ventricular fibrillation, sudden death | IV calcium, magnesium, avoid QT-prolonging drugs, pacing |
| Basal ganglia calcification | Chronic hypocalcemia causes calcium deposition | Parkinsonism, chorea, dystonia, cognitive impairment | Optimize calcium control, symptomatic treatment |
| Cataracts | Lens calcium deposition (subcapsular) | Progressive vision impairment | Cataract surgery if vision affected |
| Nephrolithiasis/nephrocalcinosis | Hypercalciuria from high calcium doses | Renal stones, renal impairment | Reduce calcium dose, add thiazide, increase hydration |
| Heart failure | Severe chronic hypocalcemia (rare) | Dilated cardiomyopathy, reduced ejection fraction | Optimize calcium, standard heart failure management |
| Pseudotumor cerebri | Increased intracranial pressure (rare) | Headache, papilledema, vision changes | Lumbar puncture, acetazolamide, optimize calcium |
Controversies and Areas of Uncertainty
- Is PTH replacement disease-modifying? rhPTH(1-84) and the long-acting prodrug palopegteriparatide reduce calcium/calcitriol requirements and improve biochemistry, but whether they prevent hard endpoints (renal impairment, basal ganglia calcification, fractures) is unproven. PTH analogues also carry a historical osteosarcoma class warning from rodent data.
- Optimal calcium target: guidelines recommend low-normal calcium, yet no trial links any specific target to clinical outcomes. The balance between symptom relief and hypercalciuria/nephrocalcinosis is individualised.
- Phosphate versus calcium control: calcium-phosphate product, not calcium alone, drives basal ganglia and ectopic calcification, but routine phosphate-lowering strategies are not standardised.
- Bone paradox: bone mineral density is high and fracture risk is not increased in cohort data, but bone is low-turnover with abnormal microarchitecture; the true fracture and quality implications remain debated.
- Defining "permanent": the 6- versus 12-month threshold after thyroidectomy varies between studies, inflating heterogeneity in reported incidence.
- Routine post-thyroidectomy PTH protocols: early PTH measurement can triage supplementation and discharge, but cost-effectiveness and the best cut-offs differ between surgical units.
Evidence Base and Key Studies
Predictors of Post-Thyroidectomy Hypocalcaemia (Systematic Review)
- Systematic review and meta-analysis of 115 observational studies of post-thyroidectomy hypocalcaemia
- Median incidence: transient hypocalcaemia 27% (IQR 19-38), permanent 1% (IQR 0-3)
- Independent predictors of permanent hypocalcaemia: 24h calcium below 1.88 mmol/L, fewer than two parathyroid glands identified, reoperation for bleeding, Graves disease, heavier specimens
- Meta-analysis: inadvertent parathyroid excision (OR 1.90), gland autotransplantation (OR 2.03), Graves disease (OR 1.75) and female sex (OR 2.28) raise transient hypocalcaemia risk
ESE Clinical Guideline: Treatment of Chronic Hypoparathyroidism in Adults
- European Society of Endocrinology GRADE-based guideline on chronic hypoparathyroidism
- Activated vitamin D analogues (calcitriol/alfacalcidol) plus calcium are standard therapy, not hormone replacement
- Target serum calcium in the low-normal range to relieve symptoms while avoiding hypercalciuria
- Monitor 24-hour urinary calcium and renal function to limit nephrolithiasis and nephrocalcinosis
- Few high-quality trials exist; no studies link a specific calcium target to clinical endpoints
Basal Ganglia Calcification in Idiopathic Hypoparathyroidism
- Study of 145 patients with idiopathic hypoparathyroidism; subset of 49 followed for a mean of 6.9 years
- Basal ganglia calcification present in 73.8% (95% CI 66.6-81.0), most often globus pallidus (68.8%), putamen (55.9%) and caudate (54.8%)
- Calcification associated with choroid plexus calcification, cataract and increased seizure risk
- Progression of calcification related to the calcium/phosphorus ratio, highlighting the value of phosphate control
- Overt parkinsonism/dystonia was uncommon (3 cases) despite the high imaging prevalence
REPLACE: Recombinant Human PTH(1-84) for Hypoparathyroidism
- Phase 3 double-blind RCT (REPLACE): 134 adults randomised 2:1 to rhPTH(1-84) 50-100 mcg/day vs placebo for 24 weeks
- Primary endpoint met by 48/90 (53%) on rhPTH(1-84) vs 1/44 (2%) on placebo (difference 51.1%, 95% CI 39.9-62.3; p<0.0001)
- Endpoint = at least 50% reduction in oral calcium and active vitamin D while maintaining serum calcium
- Most common adverse events: hypocalcaemia, muscle spasm, paraesthesia, headache, nausea; serious AE rates similar between groups
- Daily subcutaneous injection; high cost and limited availability
Co-morbidity in Postsurgical Hypoparathyroidism
- Danish registry cohort of postsurgical hypoparathyroidism matched 1:3 to general-population controls
- Increased risk of hospitalisation for infection (HR 1.42, 95% CI 1.20-1.67) and depression/bipolar disorder (HR 1.99, 95% CI 1.14-3.46)
- No increase in overall fracture risk; upper-extremity fracture risk was lower (HR 0.69, 95% CI 0.49-0.97)
- No excess of cataract, spinal stenosis or overall malignancy
- Reflects the low-turnover, dense-bone state of chronic PTH deficiency
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Post-Thyroidectomy Hypocalcemia
"A 45-year-old woman underwent total thyroidectomy for multinodular goiter 48 hours ago. She now complains of tingling around her mouth and muscle cramps in her hands. On examination, Trousseau sign is positive. Blood tests show calcium 1.7 mmol/L (normal 2.2-2.5), phosphate 1.8 mmol/L, and PTH 8 pg/mL (normal 10-65). How do you assess and manage this patient?"
Scenario 2: Hypocalcemic Seizure
"A 28-year-old man with known hypoparathyroidism (post-parathyroidectomy for severe hyperparathyroidism 2 years ago) presents to the emergency department with a generalized tonic-clonic seizure. He admits he ran out of his medications 2 weeks ago and has not been taking calcium or calcitriol. Blood tests show calcium 1.5 mmol/L, ionized calcium 0.9 mmol/L, phosphate 2.0 mmol/L, PTH undetectable, magnesium 0.6 mmol/L (low). ECG shows QTc 520 ms. How do you manage this patient?"
Scenario 3: Preoperative Optimization for Spine Surgery
"A 55-year-old woman with chronic hypoparathyroidism (autoimmune, diagnosed 10 years ago) is scheduled for elective lumbar fusion for degenerative spondylolisthesis. She takes calcium carbonate 1500 mg three times daily and calcitriol 0.5 mcg twice daily. Preoperative labs show calcium 1.9 mmol/L, ionized calcium 1.05 mmol/L, phosphate 1.6 mmol/L. ECG shows QTc 480 ms. Her surgery is scheduled in 3 days. How do you proceed?"
MCQ Practice Points
Biochemical Diagnosis Question
Q: A patient has serum calcium 1.8 mmol/L and PTH 5 pg/mL (low). What is the most likely diagnosis? A: Hypoparathyroidism. Low calcium with low PTH indicates insufficient PTH secretion. In hypocalcemia, PTH should be elevated (secondary hyperparathyroidism); if it's low, that's inappropriate and diagnostic of hypoparathyroidism. Check phosphate (expect high) and magnesium (low Mg causes functional hypoparathyroidism).
Trousseau vs Chvostek Question
Q: Which sign is more specific for hypocalcemia: Trousseau or Chvostek? A: Trousseau sign (94% sensitivity, very low false positive rate). Chvostek sign has 70% sensitivity but 10% false positive rate in normocalcemic individuals. Trousseau is induced carpopedal spasm with BP cuff inflation above systolic for 3 minutes. Chvostek is facial twitching when tapping facial nerve.
Post-Surgical Hypocalcemia Question
Q: How do you differentiate transient from permanent post-thyroidectomy hypoparathyroidism? A: Time course: Transient hypocalcemia recovers within 6 months (parathyroid gland ischemia or stunning with eventual recovery). Permanent hypoparathyroidism persists beyond 6 months (gland removal or permanent damage) and requires lifelong calcium and calcitriol replacement. Check PTH at 6 months - if still low, permanent.
Magnesium and Calcium Question
Q: Why does hypomagnesemia cause hypocalcemia? A: Hypomagnesemia (Mg less than 0.7 mmol/L) causes functional hypoparathyroidism through two mechanisms: (1) Impaired PTH secretion from parathyroid glands (magnesium required for hormone release), and (2) End-organ PTH resistance (skeletal and renal PTH resistance). Result is low calcium despite low PTH. Correct magnesium first before diagnosing true hypoparathyroidism.
Perioperative Management Question
Q: A patient with hypoparathyroidism is undergoing spine surgery. The anesthesiologist hyperventilates the patient to reduce epidural bleeding. What effect does this have on calcium? A: Hyperventilation causes respiratory alkalosis (increased pH) which increases calcium binding to albumin, lowering ionized calcium. This can precipitate hypocalcemic crisis (tetany, seizures, laryngospasm) in patients with hypoparathyroidism who have limited calcium reserve. Monitor ionized calcium intraoperatively and avoid excessive hyperventilation. Have IV calcium available.
Guidelines, Registries & Global Practice
Global Epidemiology
- Prevalence: roughly 25-40 per 100,000 population in Western registry data; defined as an orphan/rare disease in Europe and the US
- Dominant cause worldwide: post-surgical, accounting for around 75% of chronic cases; permanent hypoparathyroidism follows about 1-3% of total thyroidectomies and more after central neck dissection or reoperation
- Non-surgical causes (autoimmune, genetic, infiltrative, hypomagnesaemia-related) predominate in regions with lower thyroid-surgery volumes and in paediatric cohorts
- Idiopathic/non-surgical disease is relatively more represented in South Asian and Middle Eastern series, where it presents with prominent basal ganglia calcification and seizures
Major Guidelines Side by Side
Society Guidance on Chronic Hypoparathyroidism
| Body | Calcium target | First-line therapy | Distinctive emphasis |
|---|---|---|---|
| ESE (Europe, 2015) | Low-normal serum calcium, symptom-guided | Calcium plus activated vitamin D (calcitriol/alfacalcidol) | GRADE-based; monitor 24h urine calcium and renal function |
| First International Conference / workshop (2016) | Lower half of reference range | Calcium plus active vitamin D; PTH if poorly controlled | Unified diagnostic criteria and complication surveillance |
| International Consensus Guidelines (2022) | Asymptomatic low-normal calcium | Conventional therapy; PTH analogues reserved for refractory cases | Quality of life and long-term renal/CNS endpoints |
| Surgical societies (BAETS, AAES, AHNS) | Avoid symptomatic hypocalcaemia perioperatively | Routine post-thyroidectomy calcium plus or minus PTH protocols | Parathyroid identification, preservation and autotransplantation |
Registry and Database Signals
National registries are emerging rather than mature for hypoparathyroidism, but population datasets are informative. Danish national-registry cohorts (Underbjerg and colleagues) link postsurgical disease to excess infection and neuropsychiatric morbidity and to increased renal stones/insufficiency in idiopathic disease, while showing no overall fracture excess despite high bone mineral density. The international PARADIGHM observational registry tracks long-term outcomes and PTH-replacement safety across multiple countries.
High- vs Limited-Resource Practice Variation
- High-resource settings: intraoperative or early postoperative PTH-guided protocols, ionised calcium assays, calcitriol availability, and access to PTH analogues (rhPTH 1-84 / palopegteriparatide) for refractory disease
- Limited-resource settings: reliance on total serum calcium with albumin correction, plain (parent) vitamin D or alfacalcidol where calcitriol is scarce, and greater burden of late-presenting idiopathic disease with established basal ganglia calcification, cataract and seizures
- Universal priorities: surgeon experience and meticulous parathyroid preservation remain the single most effective preventive measure regardless of resource level
HYPOPARATHYROIDISM
Clinical summary
Key Biochemistry
- •Hypoparathyroidism: Low Ca (less than 2.0), Low PTH, High phosphate (over 1.5)
- •Vitamin D deficiency: Low Ca, High PTH (appropriate), Low 25-OH vit D
- •Pseudohypoparathyroidism: Low Ca, High PTH (PTH resistance), High phosphate
- •Always check magnesium - low Mg causes functional hypoparathyroidism
Clinical Features (CATS GO NUMB)
- •Convulsions (seizures from neuronal irritability)
- •Arrhythmias (prolonged QT, torsades de pointes)
- •Tetany (carpopedal spasm, Chvostek/Trousseau signs)
- •Spasm (laryngospasm with stridor, bronchospasm)
- •Basal ganglia calcification (Parkinsonism, chorea)
Causes
- •Post-surgical (75%): Thyroidectomy, parathyroidectomy, neck surgery
- •Autoimmune (15-20%): Isolated or polyglandular syndrome type 1
- •Genetic (5-10%): DiGeorge syndrome, X-linked, CASR mutations
- •Hypomagnesemia: Functional hypoparathyroidism (reversible with Mg)
Examination Signs
- •Chvostek sign: Facial twitch when tapping facial nerve (70% sensitive, 10% false positive)
- •Trousseau sign: Carpopedal spasm with BP cuff inflation for 3 min (94% sensitive, more specific)
- •Prolonged QT interval on ECG (QTc over 450-470 ms)
- •Carpopedal spasm: Wrist flexion, finger extension, thumb adduction (obstetrician hand)
Acute Management
- •IV calcium gluconate: 10-20 mL of 10% over 10 min, then infusion at 50 mL/hr
- •Correct magnesium if low (Mg sulfate 2 g IV, then infusion)
- •Continuous cardiac monitoring (watch for bradycardia with rapid infusion)
- •Transition to oral: Calcium carbonate 1-3 g/day + calcitriol 0.25-0.5 mcg bid
Chronic Management
- •Target serum calcium 2.0-2.2 mmol/L (low-normal, avoid hypercalciuria)
- •Calcium carbonate 1-3 g elemental calcium/day (with meals)
- •Calcitriol 0.25-2 mcg/day (activated vitamin D, essential)
- •Thiazide diuretics if hypercalciuria (increases renal Ca reabsorption)
- •Monitor: Calcium every 1-3 months, urine calcium every 6-12 months
Perioperative Management
- •Target preop calcium 2.0-2.2 mmol/L, postpone elective surgery if less than 1.9
- •Check ECG (prolonged QT increases anesthetic risk)
- •Continue oral Ca/calcitriol on day of surgery if permitted
- •Have IV calcium available in OR, monitor ionized Ca if prolonged case
- •Avoid hyperventilation (alkalosis lowers ionized calcium)
Complications
- •Seizures (hypocalcemic, generalized tonic-clonic)
- •Laryngospasm (airway obstruction, stridor)
- •Cardiac arrhythmias (torsades de pointes, VF, sudden death)
- •Basal ganglia calcification (Parkinsonism, dystonia)
- •Cataracts (subcapsular from chronic hypocalcemia)
- •Nephrolithiasis (from hypercalciuria with treatment)