Innate, Adaptive, HLA and Transplant Immunology
- The immune system has two arms. INNATE immunity is the IMMEDIATE, NON-SPECIFIC first line - physical/chemical barriers, PHAGOCYTES (neutrophils and macrophages), NATURAL KILLER (NK) cells and the COMPLEMENT system - and it has NO immunological MEMORY; ADAPTIVE immunity is SLOWER but SPECIFIC and has MEMORY - T LYMPHOCYTES (cell-mediated) and B LYMPHOCYTES that produce ANTIBODIES (humoral immunity).
- The COMPLEMENT system is a cascade of plasma proteins (classical, alternative and lectin pathways converging on C3) that OPSONISES microbes, recruits inflammatory cells (chemotaxis, e.g. C5a), and forms the MEMBRANE ATTACK COMPLEX (C5b-9) to lyse targets - it is part of innate immunity and also contributes to ANTIBODY-MEDIATED (humoral) tissue injury and transplant rejection.
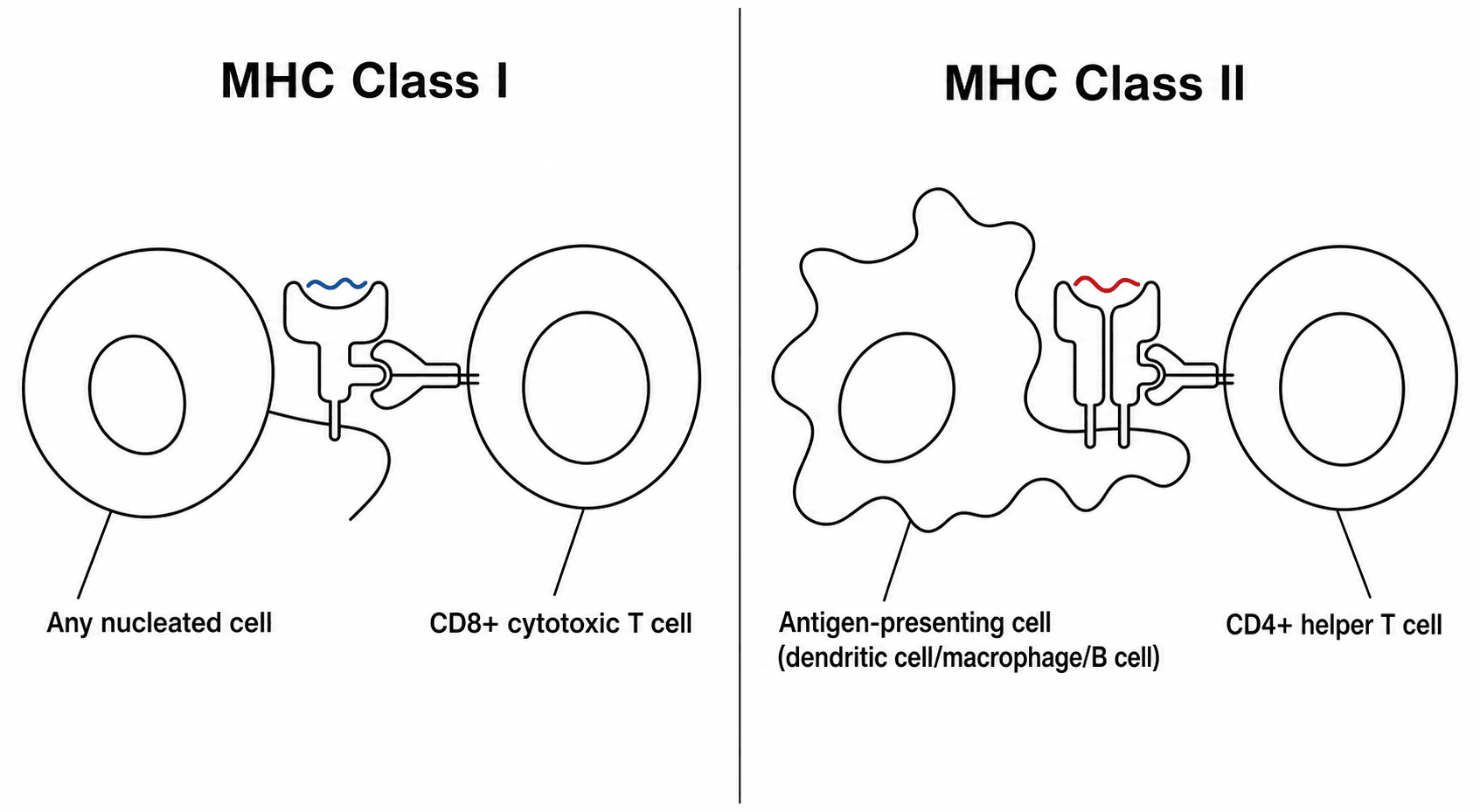
- ADAPTIVE immunity centres on ANTIGEN PRESENTATION via the MAJOR HISTOCOMPATIBILITY COMPLEX (MHC), called HLA in humans: MHC class I (HLA-A/B/C) on all nucleated cells presents to CD8 cytotoxic T cells, and MHC class II (HLA-DR/DQ/DP) on antigen-presenting cells presents to CD4 helper T cells; B cells then make antibodies, and MEMORY cells give a faster, stronger secondary response.
- ALLOGRAFT REJECTION results from recognition of FOREIGN HLA: HYPERACUTE rejection (minutes-hours) is from PRE-FORMED antibodies (e.g. ABO/HLA) activating complement; ACUTE rejection (days-weeks) is T-cell-mediated (cellular) and/or antibody-mediated (humoral, with donor-specific anti-HLA antibodies and complement); CHRONIC rejection (months-years) is a slow fibro-proliferative immune injury - HLA mismatch and donor-specific antibodies drive these processes.
- ORTHOPAEDIC APPLICATION - bone allografts: standard PROCESSED bone allograft (fresh-frozen, freeze-dried/lyophilised, or irradiated) is only WEAKLY IMMUNOGENIC because processing removes/kills the immunogenic cellular and marrow elements, so bone allografts are NOT routinely ABO/HLA matched and act largely as an osteoconductive (and variably osteoinductive) scaffold incorporated by creeping substitution.
- By contrast, FRESH OSTEOCHONDRAL ALLOGRAFTS (transplanted with viable chondrocytes) are MORE IMMUNOGENIC and can provoke a host immune response; the cartilage matrix is relatively immunoprivileged (chondrocytes shielded from immune cells), but exposed subchondral bone/marrow elements and HLA antigens can elicit a response affecting incorporation - a reason fresh osteochondral allografts are used judiciously and are not HLA-matched but are size-matched and used promptly.
- “Innate = immediate, non-specific, NO memory (barriers, phagocytes, NK cells, complement); Adaptive = specific, MEMORY (T cells, B cells/antibodies, MHC/HLA).
- “Complement: opsonisation + chemotaxis (C5a) + membrane attack complex (C5b-9); MHC I -> CD8, MHC II -> CD4.
- “Allograft rejection: hyperacute (pre-formed antibody/complement), acute (cellular T-cell +/- humoral DSA), chronic (fibroproliferative). Processed bone allograft weakly immunogenic (not HLA-matched); fresh osteochondral more immunogenic.
Barriers, phagocytes (neutrophils/macrophages), NK cells, complement. Fast, non-specific, no memory.
T cells (cell-mediated), B cells/antibodies (humoral), MHC/HLA antigen presentation, immunological memory. Slower, specific.
Innate & Adaptive Immunity
Innate immunity is the body's immediate defence: physical and chemical barriers (skin, mucosa), phagocytes (neutrophils and macrophages) that engulf pathogens, natural killer (NK) cells that kill infected/stressed cells, and the complement system; it is rapid and non-specific and has no memory. Adaptive immunity develops over days but is specific and remembers: T lymphocytes mediate cell-mediated immunity (CD4 helper T cells coordinate the response; CD8 cytotoxic T cells kill target cells), while B lymphocytes differentiate into plasma cells that secrete antibodies (humoral immunity), and memory T and B cells provide a faster, stronger response on re-exposure. The two arms are linked - innate cells (especially antigen-presenting cells) instruct the adaptive response.
Complement is a cascade of plasma proteins activated by three pathways - classical (antibody- triggered), alternative and lectin - that converge on C3. Its key effects are OPSONISATION (C3b coats microbes for phagocytosis), CHEMOTAXIS/inflammation (anaphylatoxins such as C5a recruit neutrophils), and the MEMBRANE ATTACK COMPLEX (C5b-9) that lyses target cells. As an innate mechanism it defends against infection, but it is also a major effector of antibody-mediated (humoral) tissue injury, including in transplant rejection, where donor-specific antibodies fix complement on graft endothelium.
MHC/HLA & Antigen Presentation
The major histocompatibility complex (MHC) - the human leukocyte antigen (HLA) system - presents peptide antigens to T cells and is the basis of allorecognition. MHC class I (HLA-A, -B, -C) is on all nucleated cells and presents intracellular peptides to CD8 cytotoxic T cells; MHC class II (HLA-DR, -DQ, -DP) is on antigen-presenting cells (dendritic cells, macrophages, B cells) and presents extracellular peptides to CD4 helper T cells, which then orchestrate the B-cell antibody response and cytotoxic responses. Because HLA is highly polymorphic, an individual's HLA is recognised as foreign by another's immune system - the central problem in transplantation. (HLA associations are also high-yield in rheumatology, e.g. HLA-B27 with the seronegative spondyloarthropathies.)
Allograft Rejection & Orthopaedic Application
- Hyperacute (minutes-hours): PRE-FORMED recipient antibodies (e.g. ABO or anti-HLA) bind donor endothelium and activate complement -> rapid thrombosis/graft loss.
- Acute (days-weeks): cellular (T-cell-mediated) and/or humoral/antibody-mediated rejection (donor-specific anti-HLA antibodies, DSA, with complement) - the main form prevented by immunosuppression in solid-organ transplants.
- Chronic (months-years): a slow fibro-proliferative immune-mediated injury causing graft fibrosis and failure. HLA mismatch and donor-specific antibodies drive these processes; NK cells (via KIR-HLA interactions) also contribute.
- Processed bone allograft (fresh-frozen, freeze-dried/lyophilised, irradiated) is only WEAKLY IMMUNOGENIC: processing removes or kills the immunogenic cells and marrow, leaving a largely acellular matrix that acts as an osteoconductive (and variably osteoinductive) scaffold incorporated by creeping substitution. For this reason bone allografts are NOT routinely ABO/HLA matched - unlike solid organs - and immunosuppression is not used.
- Fresh OSTEOCHONDRAL allograft (transplanted with viable chondrocytes) is MORE immunogenic: the hyaline cartilage matrix is relatively immunoprivileged (chondrocytes are shielded within matrix from immune cells), but exposed subchondral bone/marrow and HLA antigens can provoke a host response that may affect incorporation; these grafts are size-matched and used promptly but are not HLA-matched.
- Implant materials and wear debris also engage the immune system (e.g. macrophage-driven osteolysis, metal hypersensitivity) - see our Wear/Osteolysis and Metal Hypersensitivity topics.
Hypersensitivity: Gell & Coombs Types I-IV
Innate and adaptive immunity, complement, rejection and metal hypersensitivity are tied together by one framework - the Gell & Coombs hypersensitivity classification, core applied-basic-science viva material:
- Type I (immediate, IgE-mediated): allergen cross-links IgE on mast cells → degranulation (histamine) → anaphylaxis/urticaria within minutes. Orthopaedic examples: latex allergy, drug/antibiotic anaphylaxis.
- Type II (antibody-mediated, cytotoxic): IgG/IgM against cell-surface antigens, activating complement and ADCC. Examples: transfusion (ABO) reactions, hyperacute graft rejection, autoimmune cytopenias.
- Type III (immune-complex): circulating antigen-antibody complexes deposit in tissues and fix complement → vasculitis/synovitis. Examples: rheumatoid arthritis, SLE, serum sickness.
- Type IV (delayed, cell-mediated): T-cell/macrophage response peaking at 48 to 72 hours, with no antibody. Examples: metal hypersensitivity (nickel/cobalt-chromium implant reactions, including ALVAL - an aseptic lymphocyte-dominated vasculitis-associated lesion - around metal-on-metal implants), contact dermatitis, the tuberculin (Mantoux) skin test, and acute cellular transplant rejection.
The orthopaedic punchline: metal hypersensitivity / ALVAL is Type IV, hyperacute rejection is Type II, and the inflammatory arthropathies (RA, SLE) involve Type III. (Implant metal hypersensitivity and ALVAL in depth belong to our Metal Hypersensitivity / Wear-Osteolysis topics; here is the framework.)
Gell & Coombs: I immediate IgE (latex/drug anaphylaxis); II antibody-cytotoxic + complement (transfusion, hyperacute rejection); III immune-complex (RA, SLE); IV delayed T-cell, 48 to 72 hours, no antibody (metal hypersensitivity/ALVAL, contact dermatitis, Mantoux, acute cellular rejection).
The Immune Status of the Orthopaedic Patient
An "immunology in orthopaedics" topic must also cover the patient's own immune competence, which changes peri-operative decisions:
- The immunosuppressed / on-biologics patient: disease-modifying biologics (anti-TNF, anti-IL-6, rituximab) and corticosteroids raise the infection risk of surgery. The usual approach is to hold biologic agents around surgery (timed to the drug's dosing cycle) to reduce infection while balancing a disease flare, often continue methotrexate, and give peri-operative steroid cover for those on long-term steroids; restart biologics once the wound is healing and there is no infection.
- The asplenic / hyposplenic patient (e.g. after post-traumatic splenectomy): loss of the spleen's filtering and antibody function leaves a lifelong risk of overwhelming post-splenectomy infection (OPSI) from encapsulated organisms (pneumococcus, meningococcus, Haemophilus). Manage with vaccination against these organisms (ideally before, or after, splenectomy), antibiotic prophylaxis/standby, and patient education - relevant whenever the orthopaedic/trauma team is responsible for such a patient.
- General principle: the immunocompromised surgical patient (also diabetes, chemotherapy, transplant immunosuppression) has a higher infection risk and a blunted response, demanding meticulous antisepsis, optimisation, and a low threshold for investigating infection.
(The cytokines and their inhibitors are covered in our Inflammation/Cytokines topic; the point here is the peri-operative immune status.)
Mind the patient's immunity: hold biologics around surgery (continue methotrexate, give steroid cover) to cut infection risk; the asplenic patient (post-traumatic splenectomy) needs vaccination against encapsulated organisms and antibiotic prophylaxis against OPSI; the immunocompromised patient has a higher, blunted-response infection risk.
Mnemonics & Memory Aids
INNATE
Hook:INNATE = immediate, non-specific, no memory.
MHC 1-8 / 2-4
Hook:Rule of 8: MHC I x CD8 = 8; MHC II x CD4 = 8.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Outline the difference between innate and adaptive immunity, and explain the role of complement and MHC/HLA.”
“Why are bone allografts not HLA-matched, and how does this differ for fresh osteochondral allografts?”
Innate immunity
- Immediate, non-specific, NO memory
- Barriers, phagocytes (neutrophils/macrophages), NK cells, complement
- Complement: opsonisation (C3b), chemotaxis (C5a), membrane attack complex (C5b-9)
Adaptive immunity
- Specific, has MEMORY
- T cells (CD4 helper, CD8 cytotoxic) - cell-mediated; B cells -> antibodies (humoral)
- MHC I (HLA-A/B/C) -> CD8; MHC II (HLA-DR/DQ/DP) -> CD4
Allograft rejection
- Hyperacute: pre-formed antibody + complement (minutes-hours)
- Acute: cellular (T-cell) +/- humoral (DSA + complement) (days-weeks)
- Chronic: fibro-proliferative immune injury (months-years)
Orthopaedic allografts
- Processed bone allograft: weakly immunogenic - NOT HLA-matched; osteoconductive scaffold (creeping substitution)
- Fresh osteochondral allograft: viable chondrocytes - more immunogenic; cartilage relatively immunoprivileged
- Osteochondral grafts size-matched + used promptly (not HLA-matched)
Evidence & Key Studies
KIR and their HLA class I ligands in chronic rejection and graft loss in transplantation
- Incompatibility between donor and recipient for HLA (MHC) class I generates complex cellular and humoral immune responses largely responsible for rejection and graft loss.
- Alloreactive natural killer (NK) cells, regulated by killer immunoglobulin-like receptors (KIR) interacting with HLA class I, contribute to rejection - linking innate (NK) and adaptive (HLA) immunity.
- Demonstrates that HLA matching and KIR-HLA combinations influence rejection risk - the immunological basis of allorecognition.
Consensus recommendations on donor-specific anti-HLA antibodies (DSA) in transplantation
- Donor-specific anti-HLA antibodies (DSA) are an important cause of graft (engraftment) failure, reflecting antibody-mediated (humoral) rejection.
- DSA are detected by multiplex bead arrays and complement-binding (C1q) assays, linking antibody, HLA and the complement cascade.
- Higher DSA levels confer higher rejection/failure risk, and desensitization removes/neutralises antibodies and inhibits complement activation - illustrating humoral allorejection mechanisms.
The role of HLA (MHC) class I mismatch in cellular and humoral rejection and the contribution of NK cells/KIR come from the cited Littera study, and the role of donor-specific anti-HLA antibodies and complement in antibody-mediated rejection from the cited Kongtim consensus. The innate/adaptive framework, complement cascade, MHC/HLA antigen presentation and the immunogenicity of processed bone versus fresh osteochondral allografts are standard, well-established teaching. (See also our Inflammation/Cytokines, Bone Grafts and Osteochondral Allograft topics.)