Posterosuperior Labrum Contact in ABER | GIRD Essential Sign | Posterior Capsule Stretching First-Line
KEY PATHOPHYSIOLOGY STAGES
Critical Must-Knows
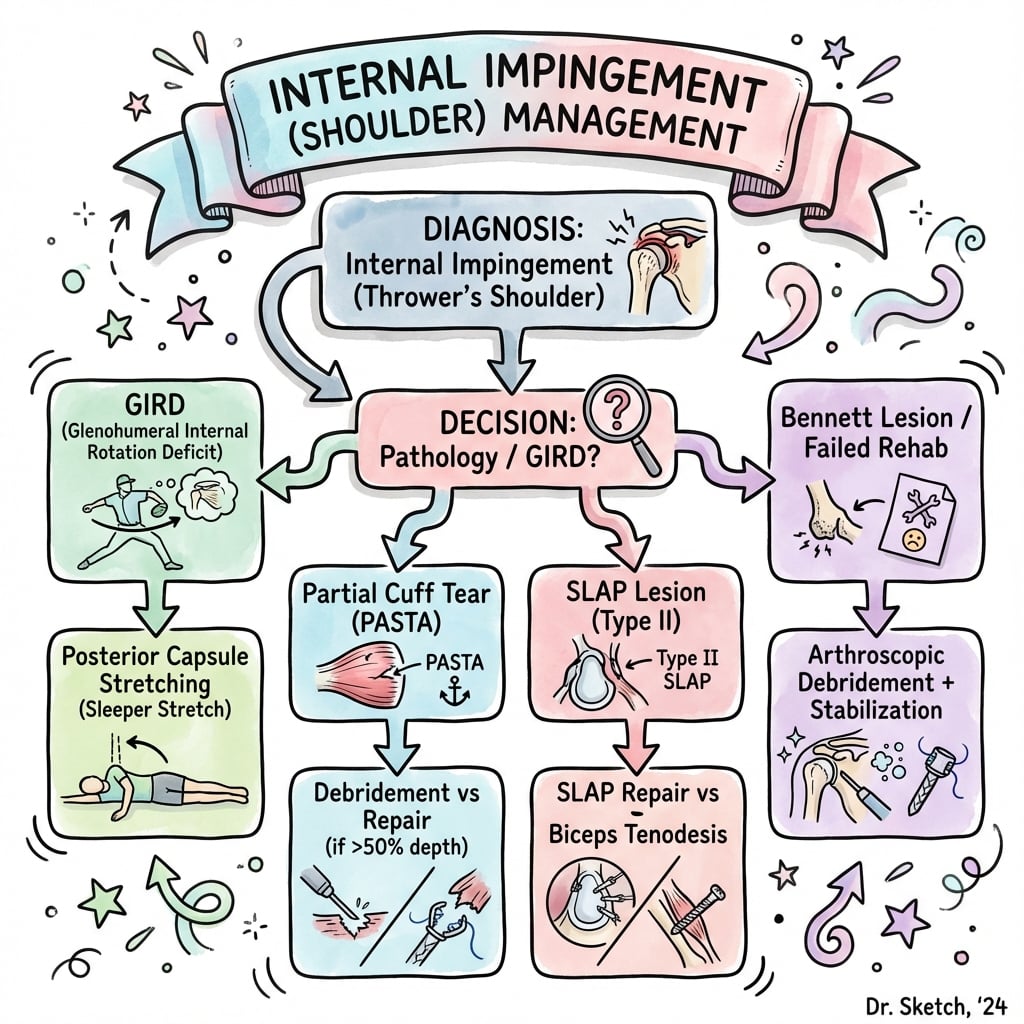
- Internal impingement is contact between posterosuperior rotator cuff and posterosuperior labrum in ABER position
- GIRD (glenohumeral internal rotation deficit) is the hallmark clinical finding - side-to-side difference greater than 20-25 degrees
- SICK scapula (Scapular malposition, Inferior medial border prominence, Coracoid pain, dysKinesis) commonly coexists
- Conservative treatment first - posterior capsule stretching and scapular stabilization for 3-6 months
- Arthroscopic debridement only after failed conservative care - debride labrum/cuff, consider posterior capsular release
Clinical Pearls
- "Internal impingement is a normal contact phenomenon exaggerated in throwers
- "GIRD is caused by posterior capsule contracture from repetitive throwing
- "Distinguish from external impingement (subacromial) - different pathology
- "Return to throwing requires extensive rehab - 6-12 months typical
Clinical Imaging


Critical Internal Impingement Exam Points
GIRD is Diagnostic
Glenohumeral Internal Rotation Deficit is the key physical finding. Measure internal rotation at 90 degrees abduction. Side-to-side difference greater than 20-25 degrees indicates pathologic GIRD requiring treatment.
Contact Not Pathologic
Internal impingement is a normal phenomenon in overhead athletes. Contact between posterosuperior cuff and labrum occurs in all shoulders in ABER. It only becomes pathologic when excessive due to GIRD and capsular imbalance.
Conservative First
Non-operative management is first-line for at least 3-6 months. Posterior capsule stretching (sleeper stretch, cross-body adduction) and scapular stabilization are highly effective. Most athletes return to sport without surgery.
SICK Scapula Association
SICK scapula commonly coexists - Scapular malposition, Inferior medial border prominence, Coracoid pain, dysKinesis. Address scapular dysfunction as part of comprehensive rehab. Scapular dyskinesis perpetuates impingement.
Quick Decision Guide - Management Algorithm
| Stage | Clinical Findings | Imaging | Treatment |
|---|---|---|---|
| Early (Adaptive) | GIRD present, posterior shoulder pain, no weakness | MRI normal or mild signal change | Posterior capsule stretching, scapular rehab, relative rest |
| Intermediate (Contact) | GIRD, pain in ABER position, partial articular-side tear | MRI: posterosuperior labral fraying, partial undersurface RTC tear | 3-6 months conservative first, then arthroscopic debridement if failed |
| Advanced (Failure) | Persistent pain, weakness, loss of velocity | MRI: full-thickness RTC tear, labral detachment | Arthroscopic repair (labrum, cuff), posterior capsular release |
GIRD - TGIRD - The Pathologic Finding
| G | Glenohumeral rotation Measured at 90 degrees shoulder abduction |
| I | Internal rotation Loss of internal rotation compared to other side |
| R | Relative deficit Side-to-side comparison critical (not absolute values) |
| D | Deficit threshold Greater than 20-25 degrees difference is pathologic |
| G | Glenohumeral rotation Measured at 90 degrees shoulder abduction | R | Relative deficit Side-to-side comparison critical (not absolute values) |
| I | Internal rotation Loss of internal rotation compared to other side | D | Deficit threshold Greater than 20-25 degrees difference is pathologic |
Hook:GIRD is the hallmark finding - always measure and compare to contralateral side
ABER - PABER - Position of Impingement
| A | Abduction 90 degrees shoulder abduction |
| B | B for throwing position Late cocking phase of throw |
| E | External rotation Maximum external rotation (layback) |
| R | Rotator cuff contact Posterosuperior cuff contacts posterosuperior labrum |
| A | Abduction 90 degrees shoulder abduction | E | External rotation Maximum external rotation (layback) |
| B | B for throwing position Late cocking phase of throw | R | Rotator cuff contact Posterosuperior cuff contacts posterosuperior labrum |
Hook:ABER position reproduces the contact that causes internal impingement
SICK - SSICK - Scapular Dysfunction Pattern
| S | Scapular malposition Scapula sits inferior and protracted |
| I | Inferior medial border Inferior angle is prominent |
| C | Coracoid pain Tenderness over coracoid process |
| K | dysKinesis Abnormal scapular motion (winging, dysrhythmia) |
| S | Scapular malposition Scapula sits inferior and protracted | C | Coracoid pain Tenderness over coracoid process |
| I | Inferior medial border Inferior angle is prominent | K | dysKinesis Abnormal scapular motion (winging, dysrhythmia) |
Hook:SICK scapula perpetuates internal impingement - must address both issues
STRETCHES - CSTRETCHES - Conservative Management
| S | Sleeper stretch Side-lying on throwing shoulder, push arm into IR |
| T | Total arc of motion Goal: restore total arc (ER + IR) |
| R | Relative rest Avoid throwing during acute phase |
| E | External rotator strengthening Maintain ER strength balance |
| T | Timing return to throw Progressive interval throwing program |
| C | Cross-body adduction stretch Stretches posterior capsule |
| H | Horizontal adduction Another posterior capsule stretch |
| E | Evaluate scapula Scapular stabilization exercises critical |
| S | Six months minimum Conservative trial 3-6 months before surgery |
| S | Sleeper stretch Side-lying on throwing shoulder, push arm into IR | E | External rotator strengthening Maintain ER strength balance | H | Horizontal adduction Another posterior capsule stretch |
| T | Total arc of motion Goal: restore total arc (ER + IR) | T | Timing return to throw Progressive interval throwing program | E | Evaluate scapula Scapular stabilization exercises critical |
| R | Relative rest Avoid throwing during acute phase | C | Cross-body adduction stretch Stretches posterior capsule | S | Six months minimum Conservative trial 3-6 months before surgery |
Hook:STRETCHES guides comprehensive non-operative management protocol
Overview and Epidemiology
Internal impingement describes the contact between the posterosuperior rotator cuff (supraspinatus and infraspinatus) and the posterosuperior glenoid labrum when the shoulder is in the ABER (abduction-external rotation) position. This is a normal phenomenon that becomes pathologic when exaggerated.
Mechanism and adaptation:
- Repetitive overhead throwing creates adaptive changes
- Posterior capsule contracture develops from repetitive microtrauma
- GIRD (loss of internal rotation) results from posterior tightness
- Obligate anterior translation occurs to achieve full external rotation
- Excessive contact between cuff and labrum causes pathologic changes
Normal vs Pathologic
Internal impingement contact occurs in all shoulders during ABER position. It only becomes pathologic when posterior capsule contracture (GIRD) causes excessive contact forces, leading to labral fraying and partial-thickness articular-sided rotator cuff tears.
At-risk populations:
- Baseball pitchers (most common)
- Volleyball players (servers, spikers)
- Tennis players (servers)
- Swimmers (freestyle, butterfly)
- Javelin throwers
- Handball players
Age and presentation:
- Typically affects adolescents to young adults (15-35 years)
- Professional and elite amateur athletes most affected
- Can occur in recreational athletes with high volume
- Males more common than females (reflecting sport participation)
Pathophysiology and Mechanisms
Normal shoulder kinematics in throwing:
The overhead throw occurs in distinct phases:
- Wind-up: Preparation phase
- Early cocking: Arm moves into abduction and external rotation
- Late cocking: Maximum external rotation (layback) - ABER position
- Acceleration: Internal rotation and forward propulsion
- Deceleration: Eccentric posterior cuff activity to slow arm
- Follow-through: Completion of motion
Late Cocking Phase
Late cocking phase is when internal impingement occurs. The shoulder is in 90 degrees abduction and maximum external rotation (up to 180 degrees in elite throwers). At this position, the posterosuperior cuff is maximally tightened and contacts the posterosuperior labrum.
Glenohumeral internal rotation deficit (GIRD):
Definition: Loss of glenohumeral internal rotation in the throwing shoulder compared to the non-throwing shoulder when measured at 90 degrees abduction.
Pathologic threshold: Greater than 20-25 degrees side-to-side difference
Mechanism of GIRD development:
- Posterior capsule contracture from repetitive eccentric loading during deceleration
- Posterior rotator cuff tightness (infraspinatus, teres minor)
- Humeral retroversion (bony adaptation in young throwers - NOT the same as GIRD)
- Acquired contracture vs congenital retroversion must be distinguished
Biomechanical consequences of GIRD:
The GIRD Cascade
GIRD creates a kinematic chain dysfunction: Posterior capsule tightness → Loss of internal rotation → Obligate anterosuperior humeral translation to achieve external rotation → Increased contact force at posterosuperior labrum → Labral fraying and articular-sided cuff tears → Pain and dysfunction.
Total rotational motion concept:
Healthy throwers often have:
- Increased external rotation (adaptive gain)
- Decreased internal rotation (adaptive loss)
- Preserved total arc of rotation (ER + IR)
Pathologic GIRD occurs when:
- Total arc of motion is decreased (not just shifted)
- Internal rotation loss exceeds external rotation gain
- Side-to-side total arc difference greater than 5-10 degrees
SICK scapula syndrome:
Scapular dyskinesis commonly coexists with internal impingement.
Components:
- S: Scapular malposition (inferior and protracted positioning)
- I: Inferior medial border prominence
- C: Coracoid pain and tenderness
- K: Dyskinesis (abnormal scapular motion - winging, lack of smooth rhythm)
Mechanism: Repetitive throwing overloads pectoralis minor → Scapular protraction and anterior tilt → Loss of scapular stability → Perpetuates impingement
Pathologic tissue changes:
| Structure | Early Changes | Advanced Changes |
|---|---|---|
| Posterior capsule | Thickening, contracture | Severe tightness, adhesions |
| Posterosuperior labrum | Fraying, degeneration | Detachment, SLAP-like tears |
| Rotator cuff (articular side) | Partial-thickness tear (less than 50%) | High-grade partial or full-thickness tear |
| Infraspinatus | Tendinopathy, signal change | Tear progression to full thickness |
Classification and Staging
Jobe Classification (modified for internal impingement)
| Stage | Description | Pathology | Treatment |
|---|---|---|---|
| I | Adaptive phase | Posterior capsule tightness, GIRD present, no structural damage | Conservative management |
| II | Contact phase | Posterosuperior labral fraying, partial articular-sided cuff tears | Conservative first, surgery if failed |
| III | Failure phase | Full-thickness rotator cuff tear, labral detachment | Surgical repair indicated |
Most athletes present in Stage II with contact pathology but no complete structural failure.
This staging guides treatment decisions and prognosis for return to sport.
Clinical Presentation and Assessment
History:
- Sport: Baseball pitcher most common, volleyball, tennis
- Symptom onset: Usually gradual, related to high volume (late season)
- Pain location: Posterior shoulder
- Position: Pain in late cocking phase (arm back, maximal ER)
- Functional deficit: Loss of velocity, control, or endurance
- Associated symptoms: Occasional anterior instability sensation (from anterior translation)
Physical examination:
Physical Examination Findings
| Test | Technique | Positive Finding | Significance |
|---|---|---|---|
| GIRD measurement | Supine, 90deg abduction, measure IR | Greater than 20-25deg loss vs contralateral | Hallmark finding - diagnostic of posterior capsule contracture |
| Total arc of motion | Sum of ER + IR at 90deg abduction | Decreased total arc vs contralateral | Indicates true capsular contracture (not just adaptation) |
| ABER position pain | 90deg abduction, maximum ER | Posterior shoulder pain reproduced | Reproduces impingement contact |
| Sleeper position pain | Side-lying on affected side, IR arm | Posterior pain, resistance | Tests posterior capsule tightness |
| Scapular dyskinesis | Observe scapular motion with arm elevation | Winging, lack of smooth rhythm, asymmetry | SICK scapula pattern |
| Coracoid tenderness | Palpate coracoid process | Focal tenderness | Part of SICK scapula syndrome |
| Rotator cuff strength | ER, IR, supraspinatus testing | Weakness suggests tear progression | Indicates structural damage |
GIRD Measurement Critical
GIRD measurement is THE key examination finding. Measure internal rotation at 90 degrees abduction with scapula stabilized. Compare to contralateral side. Greater than 20-25 degrees difference is pathologic and requires treatment with posterior capsule stretching.
Additional tests:
- Posterior impingement sign: Pain with horizontal adduction and internal rotation
- Internal rotation resistance strength test (IRRST): Resisted IR at 90deg abduction reproduces pain
- Relocation test: May be positive (anterior translation component)
Differential diagnosis:
| Condition | Key Differentiating Features |
|---|---|
| External (subacromial) impingement | Pain in forward flexion, positive Neer/Hawkins, different location |
| Anterior instability | Apprehension in ABER, history of dislocation, positive relocation |
| SLAP tear | Biceps-related symptoms, O'Brien's test positive, overhead motion pain |
| Cervical radiculopathy | Neck pain, dermatomal symptoms, Spurling's test positive |
| Thoracic outlet syndrome | Vascular/neurologic symptoms, positive Adson's test |
Investigations
Imaging protocol:
Plain radiographs:
- AP, scapular Y, axillary views
- Usually normal in early internal impingement
- May show:
- Subtle changes at posterosuperior glenoid (sclerosis)
- Calcification in posterior capsule (chronic)
- Bennett lesion (posteroinferior glenoid ossification) - related pathology
Bennett Lesion
Bennett lesion is a posteroinferior glenoid ossification of the posterior band of the inferior glenohumeral ligament at its glenoid insertion. In a systematic review of thrower's exostoses, a radiographic lesion was present in roughly half of imaged throwing athletes, of whom about three-quarters were symptomatic, and the posteroinferior location predominated (Freehill 2020). It represents a separate throwing adaptation, not internal impingement itself, although both can coexist.
MRI/MR arthrography:
MRI is the gold standard for diagnosing internal impingement pathology.
Key findings:
- ABER view (abduction-external rotation MRI sequence) - best visualizes posterosuperior pathology
- Posterosuperior labral fraying or detachment
- Partial-thickness articular-sided rotator cuff tear (high signal on T2)
- Cystic changes in posterosuperior humeral head (contact zone)
- Posterior capsular thickening
MRI findings by severity:
| Finding | Early | Intermediate | Advanced |
|---|---|---|---|
| Labrum | Normal | Fraying, increased signal | Detachment |
| Rotator cuff | Normal or signal change | Partial articular-sided tear | High-grade partial or full-thickness |
| Capsule | Subtle thickening | Moderate thickening | Severe contracture |
| Bone | Normal | Cystic change humeral head | Posterosuperior glenoid wear |
Ultrasound:
- Dynamic examination possible
- Can visualize partial-thickness cuff tears
- Operator-dependent
- Less useful for labral pathology
CT scan:
- Not typically indicated
- May be used to assess:
- Humeral retroversion (bony adaptation in young throwers)
- Glenoid version
- Osseous Bennett lesion
Advanced imaging:
- MR arthrography: May improve sensitivity for labral tears
- ABER position MRI: Specialized sequence to visualize impingement contact zone
Management Algorithm
Non-operative treatment is FIRST-LINE for all internal impingement.
Success rate: 70-80% return to sport with conservative management alone
Duration: Minimum 3-6 months trial before considering surgery
Core principles:
- Relative rest from throwing (complete rest not required)
- Posterior capsule stretching (primary intervention)
- Scapular stabilization exercises
- Maintain rotator cuff strength
- Progressive return to throwing program
Posterior capsule stretching techniques:
-
Sleeper stretch:
- Lie on throwing shoulder
- Arm forward at 90 degrees
- Use opposite hand to push throwing arm into internal rotation
- Hold 30 seconds, repeat 5 times, 3x daily
-
Cross-body adduction stretch:
- Bring throwing arm across body
- Use opposite hand to assist stretch
- Hold 30 seconds, repeat 5 times, 3x daily
-
Horizontal adduction stretch:
- Similar to cross-body but at 90 degrees flexion
- Stretches posterior capsule effectively
Scapular stabilization program:
- Serratus anterior strengthening (wall slides, push-up plus)
- Lower trapezius strengthening (prone Y, T, W exercises)
- Middle trapezius strengthening (rows)
- Pectoralis minor stretching (doorway stretch)
Rotator cuff strengthening:
- External rotator focus (infraspinatus, teres minor)
- Maintain internal rotator strength
- Avoid excessive ER strengthening (can worsen GIRD)
Conservative management should address the entire kinetic chain including core, legs, and trunk.
Surgical Technique
Patient positioning:
- Beach chair or lateral decubitus position
- Lateral decubitus allows better access to posterior structures
- Arm in traction (10-15 lbs) for lateral decubitus
Portal placement:
- Posterior viewing portal: Standard posterior portal
- Anterior working portal: Mid-glenoid or low anterior
- Posterolateral accessory portal: For posterior labrum access
- Port of Wilmington: Anterosuperior portal for suture passage
Diagnostic arthroscopy sequence:
- Glenohumeral joint evaluation (anterior, superior)
- Posterosuperior inspection (key area)
- Labral assessment (fraying, detachment)
- Rotator cuff assessment (articular side from joint)
- Subacromial space evaluation (rule out external impingement)
Systematic examination ensures all pathology is identified before proceeding with treatment.
Complications
Complications of Internal Impingement Treatment
| Complication | Incidence | Prevention/Management |
|---|---|---|
| Failure to return to sport | 30-40% (surgery) | Extensive preop and postop rehab, realistic expectations |
| Recurrent GIRD | Common if stretching stopped | Lifelong posterior capsule stretching program |
| Stiffness after surgery | 10-20% | Early ROM, avoid over-aggressive capsular release |
| Posterior instability | Rare (under 5%) | Conservative capsular release, avoid excessive release |
| Progression of cuff tear | 10-15% if partial tear | Consider repair if greater than 50% thickness |
| Axillary nerve injury | Rare (under 1%) | Stay glenoid-side during posterior capsular release |
| Persistent pain | 20-30% | Address biomechanics, kinetic chain, return to sport criteria |
Failure to return to sport:
- Most significant "complication" for athletes
- Factors: Inadequate rehab, poor biomechanics, unrealistic expectations
- Prevention: Comprehensive rehab, address kinetic chain, gradual return
- Management: Continued non-operative care, consider career counseling
Recurrent GIRD:
- Very common if stretching program abandoned
- Prevention: Educate athlete on lifelong maintenance
- Management: Resume stretching program immediately when GIRD detected
Stiffness:
- Can occur after surgery, especially with capsular release
- Prevention: Early ROM exercises, avoid immobilization
- Management: Aggressive physical therapy, consider manipulation under anesthesia if severe
Return to Sport Reality
Return to pre-injury level of throwing occurs in only 60-70% after surgery (compared to 70-80% with conservative management). Surgery is not a shortcut to recovery. Emphasize the superiority of non-operative management when possible.
Postoperative Care and Rehabilitation
Post-operative protocol (arthroscopic debridement ± posterior capsular release):
- Sling for comfort (not strict immobilization)
- Pendulum exercises day 1
- Passive ROM to tolerance
- No stretching yet (allow capsule to heal if released)
- Ice, pain control
- Progress to active-assisted ROM
- Begin gentle posterior capsule stretching (week 3-4)
- Scapular stabilization exercises
- Light rotator cuff strengthening (isometrics)
- Goal: Full passive ROM by 6 weeks
- Advance to full active ROM
- Progressive rotator cuff strengthening
- Scapular stabilization progression
- Light sport-specific activities (no throwing)
- Confirm GIRD correction
- Interval throwing program begins
- Start at 45 feet, light toss
- Maintain stretching program
- Monitor symptoms closely
- Progress distance gradually
- Progress throwing distance and intensity
- Introduce mound throwing (pitchers)
- Sport-specific training
- Return to competition if asymptomatic
- Typical return 6-9 months for debridement
Athletes who undergo simple debridement can typically return to throwing by 4-6 months with good outcomes.
Outcomes and Prognosis
Outcomes with conservative management:
| Outcome | Percentage | Notes |
|---|---|---|
| Return to same level | 70-80% | With comprehensive rehab program |
| Return to lower level | 10-15% | Modified participation |
| Unable to return | 10-15% | Career-ending |
Prognostic factors for conservative success:
- Early intervention (before structural damage)
- Compliance with stretching program
- Correction of GIRD (greater than 20 degrees improvement)
- Scapular dyskinesis addressed
- Biomechanical coaching
- Younger age
- Shorter symptom duration
Outcomes with surgical management:
| Procedure | Return to Sport | Satisfaction | Timeline |
|---|---|---|---|
| Debridement alone | 60-70% | 70-80% | 6-9 months |
| Debridement + capsular release | 65-75% | 75-85% | 6-9 months |
| Labral/cuff repair | 50-60% | 60-70% | 9-12 months |
Surgery Not Superior
Conservative management has better outcomes than surgery for internal impingement. Surgery should only be considered after 3-6 months of failed conservative care. The idea that surgery is a "fix" is incorrect - it is a salvage procedure after non-operative failure.
Factors predicting surgical success:
- GIRD corrected preoperatively
- Limited structural damage (no full-thickness tears)
- Debridement only (vs repair procedures)
- Good preoperative strength
- Excellent postoperative rehab compliance
- Realistic expectations
Factors predicting surgical failure:
- Full-thickness rotator cuff tear
- Persistent GIRD postoperatively
- Poor biomechanics not addressed
- Inadequate rehabilitation
- Return too early
- Unrealistic expectations
Long-term considerations:
- Recurrence of symptoms common if maintenance abandoned
- Progressive cuff degeneration in some athletes
- Career longevity may be shortened
- May need to modify throwing mechanics or volume
Evidence Base
- Original description of internal (posterosuperior) impingement. 17 throwing athletes (mean age 25 years) with unexplained shoulder pain and NO clinical/radiological/arthroscopic anterior instability underwent arthroscopy.
- With the arm in 90 degrees abduction and full external rotation (throwing position), impingement was directly observed between the posterosuperior glenoid rim and the undersurface of supraspinatus/infraspinatus.
- Partial articular-sided cuff rupture in 8 patients, capsulotendinous tears in 9, and posterosuperior labral lesions in 12 — defining a distinct entity from Neer subacromial and Jobe instability-related impingement.
- Landmark unified concept rejecting microinstability as the universal cause of the disabled throwing shoulder.
- Proposed that posteroinferior capsular contracture produces glenohumeral internal rotation deficit (GIRD), posterosuperior shift of the glenohumeral contact point and scapulohumeral hyperangulation, driving pathologic internal impingement and peel-back SLAP lesions.
- Companion Parts II (SLAP evaluation/treatment) and III (SICK scapula, scapular dyskinesis, kinetic chain) frame rehabilitation around restoring internal rotation and scapular control.
- Seven cadaveric shoulders tested at 90 degrees abduction and maximum external rotation (late cocking). Posteroinferior capsular plication was used to simulate contracture and induce GIRD.
- Simulated GIRD significantly increased glenohumeral contact pressure (P less than 0.05) and shifted the humeral head posteriorly during internal impingement.
- Confirms the mechanical link between posterior capsular tightness/GIRD and forceful internal impingement.
- 505 examinations on 296 professional pitchers over 8 seasons; 75 shoulder injuries and 20 surgeries. ROM measured supine at 90 degrees abduction with the scapula stabilised at the coracoid.
- Contrary to common teaching, isolated GIRD, total-rotation deficit and flexion deficit were NOT significantly associated with shoulder injury or surgery in this cohort.
- Insufficient external rotation (less than 5 degrees more ER on the throwing side) carried 2.2x risk of shoulder injury and 4.0x risk of surgery — i.e. loss of the expected ER gain, not IR loss alone, was the predictor.
- Comprehensive review of pathomechanics, examination and imaging of internal impingement, integrating instability, posterior capsular contracture and scapular dyskinesis as contributing factors.
- Presents a structured diagnostic and therapeutic algorithm: structured non-operative care first (posterior capsular stretching, scapular and cuff rehabilitation), with arthroscopy reserved for failure.
- Emphasises MR arthrography and the ABER sequence for demonstrating posterosuperior labral and articular-sided cuff lesions.
- Reaffirms that internal impingement is normal physiological posterosuperior contact that becomes symptomatic with repetitive overhead load, producing partial articular-sided cuff tears and posterosuperior labral lesions.
- Implicates a combination of factors — repetitive load, physiological humeral remodelling (retroversion), posterior capsular contracture and scapular dyskinesis causing scapulohumeral hyperangulation.
- Supports critical, individualised assessment and non-operative-first management.
- 27 studies; 158 of 306 athletes (52%) had a thrower's exostosis on imaging, of whom 75% were symptomatic. Lesions were posteroinferior in 70%, posterosuperior in 28%.
- Bennett lesion is a posteroinferior glenoid ossification of the posterior band of the inferior glenohumeral ligament — a throwing adaptation that can coexist with, but is distinct from, internal impingement.
- Surgery is reserved for refractory cases; only 61% returned to pre-injury performance after operative excision/repair.
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Classic Presentation in Baseball Pitcher
"A 22-year-old professional baseball pitcher presents with posterior shoulder pain during the late cocking phase of throwing. He has lost 10 mph velocity over the past 2 months. On examination, he has 55 degrees of internal rotation on the throwing side vs 80 degrees on the non-throwing side, measured at 90 degrees abduction. External rotation is 95 degrees bilaterally. What is your diagnosis and management?"
Scenario 2: Surgical Decision-Making After Failed Conservative Care
"The pitcher from Scenario 1 has undergone 4 months of intensive physical therapy with posterior capsule stretching. His GIRD has improved from 25 degrees to 15 degrees. However, he still has posterior shoulder pain when attempting to throw and cannot achieve full velocity. MRI shows posterosuperior labral fraying and a 30% partial articular-sided tear of the infraspinatus. He wants to continue his professional career. What is your recommendation?"
Scenario 3: Differential Diagnosis Challenge
"A 19-year-old collegiate volleyball player presents with shoulder pain during serving and spiking. She describes the pain as 'deep inside' her shoulder when her arm is back. She also notes occasional clicking. On examination, she has GIRD of 15 degrees, pain with ABER position, and a positive O'Brien's test. MRI shows posterosuperior labral signal abnormality and a possible SLAP lesion. How do you differentiate between internal impingement and a SLAP tear, and how does this affect your management?"
MCQ Practice Points
Definition Question
Q: What is the anatomic contact in internal impingement of the shoulder? A: Posterosuperior rotator cuff (supraspinatus-infraspinatus junction) contacts the posterosuperior glenoid labrum when the shoulder is in ABER (abduction-external rotation) position. This is a normal phenomenon that becomes pathologic with repetitive overhead activity.
GIRD Question
Q: What is the pathologic threshold for GIRD (glenohumeral internal rotation deficit)? A: Greater than 20-25 degrees loss of internal rotation compared to the contralateral shoulder, measured at 90 degrees of shoulder abduction with the scapula stabilized. This indicates posterior capsule contracture requiring treatment.
Management Question
Q: What is first-line treatment for internal impingement syndrome in a throwing athlete? A: Conservative management with posterior capsule stretching (sleeper stretch, cross-body adduction stretch) and scapular stabilization exercises for minimum 3-6 months. This has 70-80% success rate for return to sport, which is superior to surgical outcomes.
SICK Scapula Question
Q: What does the SICK scapula mnemonic stand for? A: S: Scapular malposition (inferior and protracted), I: Inferior medial border prominence, C: Coracoid pain and tenderness, K: dysKinesis (abnormal scapular motion). This commonly coexists with internal impingement and must be addressed in treatment.
Surgical Indication Question
Q: When should arthroscopic debridement be considered for internal impingement? A: After failed conservative management (minimum 3-6 months trial) with persistent pain limiting performance despite GIRD correction efforts, AND documented structural pathology on MRI (posterosuperior labral fraying, partial articular-sided rotator cuff tear).
Return to Sport Question
Q: What percentage of overhead athletes return to pre-injury level after arthroscopic treatment for internal impingement? A: 60-70% after arthroscopic debridement, which is actually lower than the 70-80% success rate with conservative management alone. This emphasizes that surgery is a salvage procedure, not a superior treatment option.
Guidelines, Registries & Global Practice
Internal impingement is a clinical/biomechanical diagnosis of the overhead athlete; there is no joint-replacement registry for it and no single national society has issued a dedicated standalone guideline. The evidence base is therefore built from the original arthroscopic description, biomechanical models, prospective athlete cohorts and society-level overhead-athlete/shoulder-instability consensus. The world standard of care is consistent: non-operative management first, surgery only for refractory structural failure.
Global epidemiology (PubMed-backed):
| Domain | Evidence | Source |
|---|---|---|
| At-risk population | Throwing/overhead athletes; dominant arm; typically 15-35 years | Walch 1992 (PMID 22959196) |
| Injury predictor in pitchers | Insufficient external-rotation gain → 2.2x shoulder injury, 4.0x surgery; isolated GIRD NOT independently significant in a 296-pitcher prospective cohort | Wilk 2015 (PMID 26272516) |
| GIRD and injury (earlier data) | Pitchers with GIRD nearly twice as likely to be injured, but not statistically significant (P=0.17) in a 122-pitcher series | Wilk 2010 (PMID 21131681) |
| Associated bony adaptation | Thrower's exostosis (incl. Bennett lesion) on imaging in roughly half of throwers; ~75% symptomatic; posteroinferior predominant | Freehill 2020 (PMID 32704507) |
Common Teaching vs Best Current Evidence
The classic teaching that "GIRD greater than 20-25 degrees causes injury" is a useful clinical screen but is not a clean independent predictor in the best prospective data (Wilk 2015, PMID 26272516). The more robust message is to assess the total rotational arc and whether the expected external-rotation gain is preserved. Treat loss of total arc and posterior capsular contracture, not an isolated IR number.
Side-by-side guidance (overhead athlete shoulder):
| Body / region | Position on internal impingement | Evidence level |
|---|---|---|
| AAOS / AOSSM (US) | No disease-specific guideline; consensus within overhead-athlete and shoulder-instability literature favours structured non-operative care first, debridement/capsular management for failures | Expert consensus / Level IV-V |
| BOA / BESS (UK) | Managed within shoulder instability and atraumatic instability pathways; physiotherapy-led rehabilitation (e.g. structured programmes) is first-line for atraumatic/overhead shoulder dysfunction | Level IV-V, programme-based RCT evidence for rehab |
| EFORT / ESSKA (Europe) | Recognise posterosuperior impingement as a distinct entity; arthroscopic options range from debridement to selective SLAP/biceps and capsular procedures after failed rehabilitation | Level IV |
| AO Foundation | Not a fracture/fixation topic — no AO guidance; relevant only for associated bony glenoid lesions | N/A |
| Universal landmark concept | GIRD / posterior capsular contracture model and SICK scapula drive rehabilitation worldwide | Burkhart 2003 (PMID 12671624) |
Registry evidence: Not applicable — this is a soft-tissue/biomechanical sports diagnosis, not an arthroplasty or implant procedure, so the joint registries (NJR, AJRR, AOANJRR, SHAR, NZJR) do not capture it. Outcome data derive from athlete cohort studies and case series rather than registries.
Global practice variation:
- Sport mix drives the case-mix, not the pathology. Baseball pitchers dominate North American series; cricket fast bowlers (similar late-cocking biomechanics), handball, javelin, tennis serving, volleyball and competitive swimming predominate in Europe, Australasia and Asia. The underlying GIRD/posterior-capsule mechanism is identical.
- High-resource settings use MR arthrography with ABER sequences and arthroscopy for refractory cases; limited-resource settings rely on clinical GIRD assessment, plain radiographs and supervised physiotherapy, with strong outcomes given that non-operative care is first-line everywhere.
- Return-to-sport timing is shaped by the competitive calendar (e.g. off-season surgery), professional contracts and access to sports physiotherapy, rather than by differing surgical doctrine.
Differential Diagnosis of the Painful Overhead Shoulder
| Condition | Key history | Discriminating examination | Imaging / confirmation |
|---|---|---|---|
| Internal (posterosuperior) impingement | Posterior 'deep' pain in late cocking (ABER), velocity loss, gradual onset | GIRD / reduced total arc, pain reproduced in ABER, positive posterior impingement sign | MRA/ABER MRI: posterosuperior labral fraying + articular-sided cuff tear |
| External (subacromial) impingement | Pain with forward elevation/overhead reaching, older or non-throwing patient | Positive Neer and Hawkins-Kennedy, painful arc, subacromial tenderness | Bursal-sided changes, acromial morphology; relief with subacromial block |
| Anterior glenohumeral instability | Apprehension/'dead arm' in ABER, history of subluxation/dislocation | Positive apprehension AND relocation (pain relieved by posterior force) | MRA: anteroinferior labral (Bankart) lesion |
| SLAP / superior labral tear | Mechanical clicking, biceps-region pain, overhead pain in multiple positions | Positive O'Brien (active compression), dynamic labral shear; peel-back at arthroscopy | MRA superior labral detachment at 12 o'clock (vs 10-11 o'clock for internal impingement) |
| Bennett lesion (thrower's exostosis) | Posterior shoulder ache in throwers, may be incidental | Posteroinferior glenoid tenderness, often coexists with GIRD | Posteroinferior glenoid ossification on axillary radiograph/CT (Freehill 2020) |
| Cervical radiculopathy | Neck pain, dermatomal arm symptoms, paraesthesia | Positive Spurling, neurological deficit, normal local shoulder tests | Cervical MRI; nerve root compression |
| Thoracic outlet / neurovascular | Positional arm heaviness, vascular or neurological symptoms | Positional provocation (Roos/Adson), pulse/colour change | Vascular studies, dynamic imaging |
Exam Context
Be prepared to describe the pathomechanics of GIRD causing internal impingement (Burkhart 2003; Mihata 2015 cadaveric model). Understand that structured non-operative management is first-line with the majority of athletes returning to sport. Know the GIRD measurement technique (90 degrees abduction, scapula stabilised) and the classic pathologic threshold (greater than 20-25 degrees), but be ready to qualify it with the prospective evidence (Wilk 2015) that the total rotational arc and preserved external-rotation gain matter more than an isolated IR deficit. Emphasise that surgery is reserved for failed conservative care and has inferior return-to-sport rates to successful non-operative management.
INTERNAL IMPINGEMENT OF THE SHOULDER
Clinical summary
CORE PATHOPHYSIOLOGY
- •Contact between posterosuperior rotator cuff and posterosuperior labrum in ABER position
- •Normal phenomenon that becomes pathologic with repetitive overhead activity
- •GIRD (glenohumeral internal rotation deficit) is the hallmark clinical finding
- •Posterior capsule contracture → GIRD → Obligate anterior translation → Excessive contact
- •Results in posterosuperior labral fraying and partial articular-sided cuff tears
GIRD MEASUREMENT
- •Patient supine, shoulder 90 degrees abduction, elbow 90 degrees flexion
- •Stabilize scapula to isolate glenohumeral motion
- •Measure maximum passive internal rotation bilaterally
- •Pathologic threshold: greater than 20-25 degrees side-to-side difference
- •Also measure total arc (ER + IR) - loss of total arc indicates true contracture
CLINICAL PRESENTATION
- •Overhead throwing athletes (baseball, cricket, volleyball, tennis, swimming)
- •Posterior shoulder pain in late cocking phase (ABER position)
- •Loss of velocity or performance in throwing/serving
- •GIRD on examination (greater than 20-25 degrees)
- •Pain reproduced in ABER position
- •SICK scapula commonly coexists
SICK SCAPULA
- •S: Scapular malposition (inferior and protracted)
- •I: Inferior medial border prominence
- •C: Coracoid pain and tenderness
- •K: dysKinesis (abnormal scapular motion)
- •Must address scapular dysfunction in treatment
CONSERVATIVE MANAGEMENT (FIRST-LINE)
- •70-80% return to sport success rate (superior to surgery)
- •Minimum 3-6 months trial before considering surgery
- •Posterior capsule stretching: Sleeper stretch, cross-body adduction (5x30sec, 3x daily)
- •Scapular stabilization exercises (serratus, trapezius strengthening)
- •Rotator cuff strengthening maintenance
- •Interval throwing program after symptoms resolve (6-12 months total)
- •Lifelong maintenance stretching required
SURGICAL MANAGEMENT
- •Indications: Failed 3-6 months conservative care, persistent symptoms
- •Arthroscopic debridement: Posterosuperior labral fraying, partial cuff tear
- •Posterior capsular release: For persistent GIRD
- •Do NOT repair partial tears under 50% thickness (avoid conversion to full-thickness)
- •Do NOT repair degenerative labral fraying (debride only)
- •Return to sport: 60-70% (inferior to conservative management)
- •Timeline: 6-9 months (debridement), 9-12 months (if repair needed)
IMAGING
- •Plain radiographs: Usually normal, rule out Bennett lesion
- •MRI/MRA: Posterosuperior labral fraying, partial articular-sided cuff tear
- •ABER view MRI: Best visualizes contact zone
- •Cystic changes in posterosuperior humeral head (contact zone)
- •Posterior capsular thickening
KEY EXAM PEARLS
- •Internal impingement is NORMAL contact that becomes PATHOLOGIC
- •GIRD greater than 20-25 degrees is pathologic threshold
- •Conservative management has BETTER outcomes than surgery (70-80% vs 60-70%)
- •Posterior capsule stretching is PRIMARY treatment
- •Surgery is SALVAGE after failed conservative care, not first-line
- •SICK scapula commonly coexists - must address scapular dysfunction
- •Lifelong maintenance stretching required (no cure, only management)
- •Distinguish from SLAP tears (can coexist but different treatment)