Biomechanical Loads | Hip 3-7x BW | Free Body Diagrams | Arthroplasty Design
- Joint reaction force = resultant force acting across joint surface in response to external/internal loads
- Calculated using free body diagrams and static equilibrium (ΣF = 0, ΣM = 0)
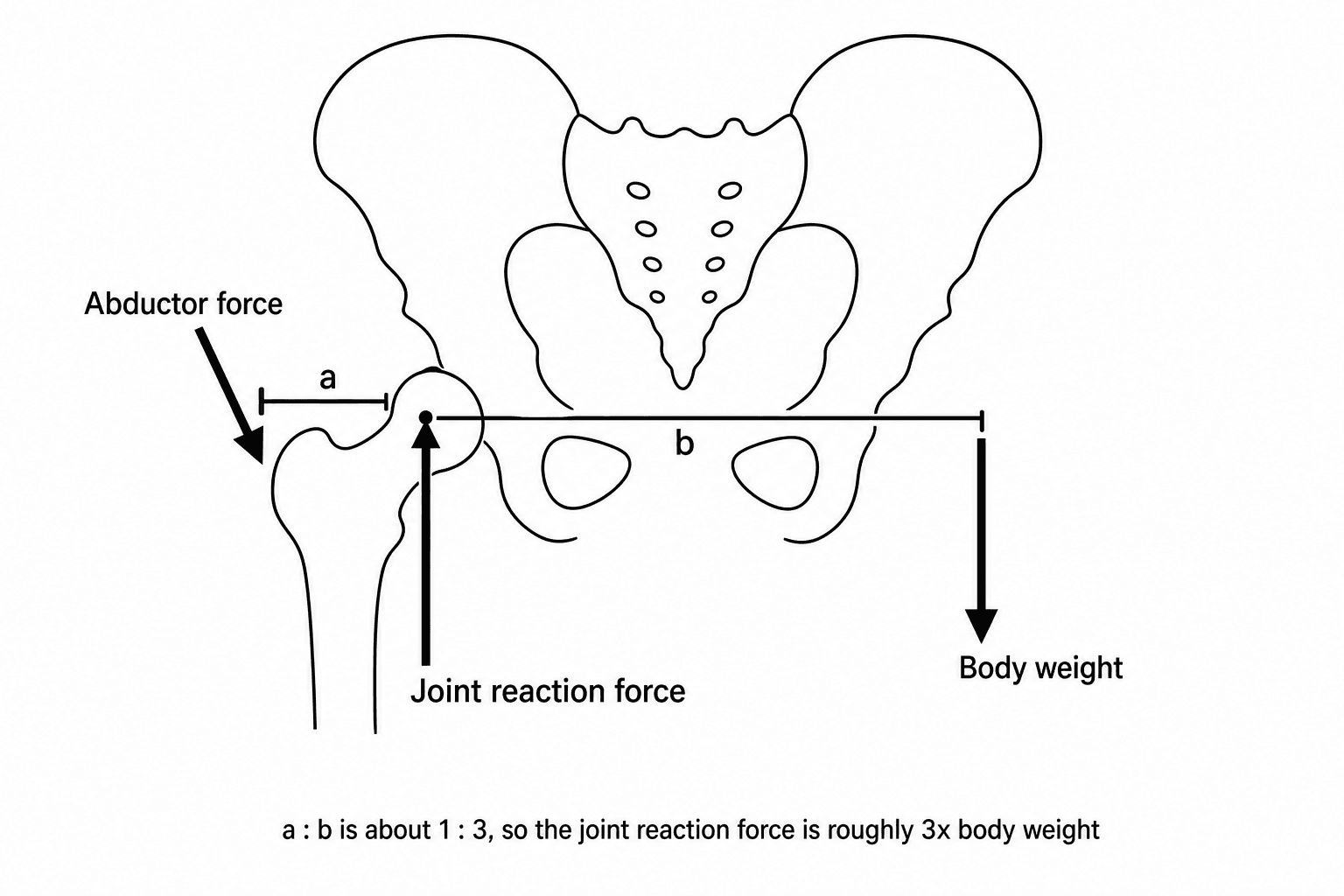
- Hip: 3-7x body weight during normal gait, peak at mid-stance phase
- Abductor muscle force creates large hip reaction force (long moment arm from body weight)
- Clinical relevance: implant design, wear patterns, fixation requirements, bearing surfaces
- “Joint reaction force far exceeds body weight due to muscle forces and leverage
- “Free body diagram essential: isolate joint, show all forces (body weight, muscle, reaction)
- “Reducing moment arm reduces muscle force needed (reduces reaction force)
- “Hip offset restoration critical to maintain normal abductor biomechanics
- “Bearing surface wear directly related to magnitude of reaction force
Essential calculation tool: Isolate the joint segment. Draw all forces (gravity on body, muscle forces, joint reaction). Apply equilibrium: ΣF = 0 and ΣM = 0 (sum of moments about joint = zero). Solve for unknown reaction force magnitude and direction.
Hip joint reaction force reaches 3-7x body weight at mid-stance phase of gait. Abductor muscles (gluteus medius/minimus) contract powerfully to prevent pelvic drop. Short lever arm from muscle insertion means large muscle force required, creating massive joint reaction.
Joint reaction force is NOT just body weight - muscle forces are the major contributor. Muscles have short lever arms (moment arms) compared to body weight, requiring large forces. Example: Hip abductors generate 2-3x body weight force, creating total hip reaction of 3-7x BW.
High reaction forces drive: bearing surface wear, polyethylene degradation, implant loosening, osteolysis. Restoration of normal biomechanics (offset, leg length, joint line) critical. Obesity massively increases forces and implant failure risk.


Overview and Fundamental Concepts
Joint reaction force is the resultant force acting across a joint surface, arising from the combined effect of external loads (body weight, ground reaction forces) and internal loads (muscle and ligament forces). Understanding joint reaction forces is fundamental to orthopaedic biomechanics, implant design, and the pathophysiology of degenerative joint disease.
These forces are typically several times body weight during routine activities due to the mechanical disadvantage of muscle attachments. Muscles attach close to joints (short moment arms) while body weight acts at a distance (long moment arm from the center of mass), requiring large muscle forces to maintain equilibrium.
Clinical Significance: Joint reaction forces directly influence articular cartilage stress, bearing surface wear in arthroplasty, fixation loads on implants, bone remodeling patterns, and the progression of osteoarthritis. Surgeons must understand these forces to optimize implant positioning, select appropriate bearing surfaces, and counsel patients on activity modification.
The mechanical principle: Muscles have very short lever arms (moment arms) compared to body weight acting from the center of mass. To balance moments about the joint (ΣM = 0), muscle force must be 2-4x body weight. Joint reaction force equals the vector sum of body weight PLUS muscle forces, resulting in 3-7x BW at the hip during normal walking.
Epidemiology and Context
Joint reaction forces vary systematically across joints and activities:
- Hip joint: 2.5-3x BW standing on one leg; 3-7x BW during normal gait (peak mid-stance); up to 8-10x BW during running or stumbling
- Knee joint: 2-3x BW walking; 3-4x BW stair climbing; 6-8x BW running; up to 24x BW during landing from a jump (elite athletes)
- Ankle joint: 4-5x BW during normal walking; 8-13x BW during running due to ground reaction force magnification
- Shoulder joint: 0.5-1.5x BW depending on arm position and load (different mechanics due to non-weight-bearing nature)
These magnitudes have been measured using instrumented implants with telemetry systems, validating theoretical calculations from biomechanical modeling.
Relevance to Arthroplasty
Understanding joint reaction forces is critical for:
- Implant design: Bearing surfaces must withstand millions of cycles at 3-7x body weight loads
- Wear prediction: Volumetric wear directly proportional to load magnitude in polyethylene bearings
- Fixation requirements: Cement mantles and bone-implant interfaces experience these cyclical loads
- Component positioning: Malposition alters moment arms and increases reaction forces
- Patient counseling: Obesity and high-impact activities dramatically increase implant stress and failure risk
Core Concepts - Biomechanical Calculation Principles
Free Body Diagram Method
The standard approach to calculating joint reaction forces uses static equilibrium principles applied to a free body diagram:
Step 1: Isolate the Body Segment Draw the bone segment (e.g., femur for hip analysis) isolated from adjacent segments. The joint becomes a "cut" where internal forces are exposed as unknowns.
Step 2: Identify All Forces Draw vectors for:
- Body weight (W): Acts downward through the center of mass
- Muscle forces (Fm): Primary stabilizers (e.g., hip abductors)
- Joint reaction force (R): Unknown magnitude and direction at joint center
Step 3: Establish Coordinate System Typically horizontal (x) and vertical (y) axes aligned with anatomical planes.
Step 4: Apply Equilibrium Equations
For static equilibrium:
- ΣFx = 0: Sum of horizontal forces equals zero
- ΣFy = 0: Sum of vertical forces equals zero
- ΣM = 0: Sum of moments about any point equals zero
Step 5: Solve for Unknowns Use moment equation to find muscle force, then force equations to find reaction force components. Combine components to get resultant magnitude and direction.
- Definition
- Total body mass × gravity
- Typical Hip Value
- 70 kg × 9.8 = 686 N
- Clinical Significance
- Baseline external load
- Definition
- Glut med/min contraction
- Typical Hip Value
- 2-3x body weight (1500 N)
- Clinical Significance
- Primary force magnitude
- Definition
- dW / dm (body weight / muscle)
- Typical Hip Value
- Typically 2.5:1
- Clinical Significance
- Mechanical disadvantage
- Definition
- Resultant across joint
- Typical Hip Value
- 3-7x BW (2500-5000 N)
- Clinical Significance
- Determines implant wear
Key Biomechanical Principles
Principle 1: Mechanical Advantage and Leverage Muscles operate at a mechanical disadvantage. The moment arm of body weight about the hip joint (typically 10-15 cm) is 2-3 times larger than the abductor muscle moment arm (4-6 cm). This ratio means abductor force must be 2-3 times body weight just to balance the pelvis during single-leg stance.
Principle 2: Vector Addition The joint reaction force is NOT simply body weight minus muscle force. Instead, it is the vector sum (resultant) of all forces acting on the segment. Since muscle force and body weight act in roughly opposite directions vertically but both compress the joint, the reaction force magnitude exceeds either individual force.
Principle 3: Dynamic vs Static Analysis The calculations above assume static equilibrium (standing still). During gait, acceleration terms introduce additional inertial forces (F = ma), further increasing peak reaction forces during mid-stance push-off.
Given: 70 kg person standing on one leg. Body weight moment arm = 12 cm. Abductor moment arm = 5 cm. Find hip reaction force. Step 1: ΣM = 0 about hip center: Fm × 5 = W × 12. Thus Fm = 2.4W = 2.4 × 686 N = 1646 N. Step 2: ΣFy = 0: R = Fm + W = 1646 + 686 = 2332 N = 3.4x body weight. This is the examiner's favorite calculation question!
The free-body method is not limited to the limb joints tabulated in this topic - it applies equally to the lumbar spine, which is a favourite viva extension and is governed by exactly the same short-lever-arm mechanics.
- Why disc loads are so high: the erector spinae act on a very short posterior lever arm (only about 5 to 6 cm behind the disc), whereas a held load and the weight of the trunk act on a long anterior lever arm. To balance the flexion moment about the L5-S1 disc, the back extensors must generate a large force, and the disc compressive (reaction) force is the sum of that muscle force plus body and external load - it can reach several thousand newtons even when lifting modest weights, far exceeding the weight actually held.
- Keep the load close - it is moment-arm control: bending forward or holding a load away from the body lengthens the anterior lever arm, multiplying the extensor force and the disc reaction force. Lifting with the load close to the trunk shortens that lever arm and is the single biggest reduction in spinal load - the biomechanical basis of safe-lifting advice (and why a "straight-back, load-close" technique protects the disc more than leg-versus-back debate alone).
- Raised intra-abdominal pressure (the abdominal muscles bracing against the diaphragm) creates an anterior supporting column that slightly offloads the posterior elements, one rationale for bracing during heavy lifting.
Exam point: the lumbar disc obeys the same rule as the hip - a short erector-spinae lever arm versus a long load lever arm makes L5-S1 compressive (reaction) forces reach several thousand newtons, so the most effective way to lower spinal load is to keep the load close to the body (shorten its moment arm), aided by raised intra-abdominal pressure.
Hip Joint Reaction Forces
Magnitude During Activities
The hip joint experiences some of the highest forces in the human body:
Gait Cycle Analysis: Hip reaction force varies throughout the gait cycle:
- Heel strike: 2-3x BW (initial loading)
- Mid-stance: 4-7x BW (PEAK - single leg support with rapid weight transfer)
- Toe-off: 2-3x BW (push-off phase)
- Swing phase: Less than 1x BW (no ground contact)
The double-peak pattern during stance phase reflects the biomechanical demands of single-leg support and forward propulsion.
Abductor Muscle Mechanics
The hip abductors (gluteus medius and minimus) are the critical force generators:
- Origin: Outer surface of ilium
- Insertion: Greater trochanter of femur
- Moment arm: Approximately 5-6 cm from hip center of rotation
- Function: Prevent pelvic drop on opposite side during single-leg stance
During mid-stance gait, the pelvis and upper body (approximately 5/6 of total body weight) create a large overturning moment about the stance hip. The abductors must generate 2-3x body weight force to counteract this moment due to their short moment arm.
If abductors are weak or non-functional (e.g., superior gluteal nerve injury, severe trochanteric pain syndrome), the patient cannot generate sufficient abductor force. The pelvis drops on the swing leg side, and the patient compensates by lurching the trunk over the stance hip (reducing the body weight moment arm to maintain balance).
Differential Diagnosis of an Abductor-Lurch / Trendelenburg Gait
A positive Trendelenburg sign reflects a failure of the abductor force couple, but several distinct mechanisms produce it. Distinguishing them is a common viva probe because each changes management.
- Mechanism (relation to joint reaction force)
- Abductor force generation lost; cannot balance body-weight moment
- Key Distinguishing Feature
- Weakness with intact tendon; iatrogenic after lateral/anterolateral approaches
- Management Direction
- Protect nerve intra-op; physiotherapy; usually recovers
- Mechanism (relation to joint reaction force)
- Mechanically uncoupled tendon; force not transmitted to trochanter
- Key Distinguishing Feature
- Lateral hip pain, MRI tendon discontinuity, fatty atrophy
- Management Direction
- Repair vs conservative depending on tear and demand
- Mechanism (relation to joint reaction force)
- Shortened abductor moment arm raises required muscle and reaction force
- Key Distinguishing Feature
- Radiographic short offset or low neck-shaft angle
- Management Direction
- Restore offset (THR templating; osteotomy)
- Mechanism (relation to joint reaction force)
- Voluntary off-loading to reduce reaction-force-driven pain
- Key Distinguishing Feature
- Pain-limited, improves with analgesia/aids
- Management Direction
- Treat OA; cane, weight loss, arthroplasty
- Mechanism (relation to joint reaction force)
- High, lateralised centre lengthens body-weight arm and concentrates contact stress
- Key Distinguishing Feature
- Shallow acetabulum, high centre on radiograph
- Management Direction
- Periacetabular osteotomy or reconstruction
- Mechanism (relation to joint reaction force)
- Altered abductor tension-length and pelvic obliquity
- Key Distinguishing Feature
- Measurable limb-length difference; corrects with block
- Management Direction
- Shoe raise; address surgical cause
Effect of Hip Geometry on Forces
Several anatomical and surgical factors alter hip reaction forces:
- Biomechanical Effect
- Larger abductor moment arm
- Force Change
- Reduces force 10-20%
- Clinical Relevance
- Restore offset in THR for normal mechanics
- Biomechanical Effect
- Smaller abductor moment arm
- Force Change
- Increases force 15-30%
- Clinical Relevance
- Avoid excessive medialization in THR
- Biomechanical Effect
- Shortens abductor moment arm
- Force Change
- Increases force
- Clinical Relevance
- May contribute to implant loosening
- Biomechanical Effect
- Reduces body weight moment
- Force Change
- Reduces force 20-40%
- Clinical Relevance
- Effective conservative measure
In total hip replacement, maintaining or restoring normal femoral offset is biomechanically critical. Each 1 cm increase in offset reduces abductor force requirement by approximately 15%, with corresponding reduction in hip reaction force. This reduces bearing surface wear and improves abductor efficiency.
Lengthening the limb tightens the abductors, improving their tension-length relationship but potentially increasing joint reaction force if excessive. Shortening reduces abductor tension and efficiency, potentially causing Trendelenburg gait.
Instrumented Implant Data
Direct measurements from instrumented hip replacements (telemetry systems) have validated theoretical models:
- Bergmann et al. demonstrated peak forces of 2.5-3.5x BW during normal walking in elderly patients with THR
- Younger, more active patients generate forces up to 4-5x BW during normal gait
- Stumbling or fall events can generate transient peaks of 8-10x BW
- Prolonged standing on one leg: sustained 2.5-3x BW
These data inform implant design requirements and wear testing protocols (ISO standards require testing at 3x BW for 5-10 million cycles to simulate 10-20 years of use).
The free-body analysis above is essentially Pauwels' balance-beam (seesaw) model of the hip: the femoral head is the fulcrum, body weight acts on the long medial lever arm and the abductors pull on the short lateral lever arm, so the abductors must generate a large force and the resultant joint reaction force is several times body weight. This single concept generates two high-yield exam applications.
1. Reducing the reaction force by changing the lever arms - anything that lengthens the abductor lever arm or shortens the body-weight lever arm lowers the required muscle force and therefore the reaction force. This is the principle behind increasing femoral offset, medialising the hip centre with the trunk (Pauwels), and a valgus or medial-displacement intertrochanteric osteotomy used historically for OA and for difficult femoral-neck nonunions.
2. Pauwels classification of femoral neck fractures - the orientation of the fracture line relative to the horizontal determines how the joint reaction force is resolved across it:
- Pauwels I (about 30 degrees) - the force is largely compressive across the fracture, favouring union.
- Pauwels II (about 50 degrees) - intermediate.
- Pauwels III (about 70 degrees, near-vertical) - the force becomes largely shear, which displaces the fracture and gives the highest nonunion and fixation-failure rate. The more vertical the fracture, the more a fixed-angle device (sliding hip screw or a fixed-angle plate) is favoured over parallel screws, and a valgus osteotomy can convert shear into compression.
Exam point: the hip is a Pauwels balance beam (fulcrum at the head, long body-weight arm vs short abductor arm); lengthening the abductor arm or shortening the body-weight arm lowers the reaction force, and a more vertical (Pauwels III) femoral neck fracture converts that large reaction force into shear, driving nonunion and changing the fixation choice.
Knee Joint Reaction Forces
Magnitude and Activity Dependence
Knee joint forces are lower than hip during walking but can exceed hip forces during high-impact activities:
- Heel strike: 2x BW (initial impact absorption)
- Mid-stance: 2-3x BW (controlled flexion, quadriceps eccentric contraction)
- Terminal stance: 2.5-3x BW (push-off preparation)
- Swing phase: Minimal force (less than 0.5x BW)
- Ascending stairs: 3-4x BW (quadriceps work to extend knee against gravity)
- Descending stairs: 3-4.5x BW (eccentric quadriceps control, often higher than ascending)
Patellofemoral vs Tibiofemoral Forces
The knee has two articulations with different force patterns:
- Primarily compression from body weight and ground reaction force
- Range: 2-4x BW during walking
- Distributed across medial and lateral compartments (60:40 ratio medially in normal alignment)
- Forces from quadriceps tendon and patellar tendon creating compressive force on patella
- Magnitude = Quadriceps force × sin(knee flexion angle / 2)
- Peak at 30-60 degrees flexion (stair climbing, rising from chair)
- Can reach 5-7x BW during deep knee bends or squatting
Understanding the different force patterns explains why patellofemoral arthritis and tibiofemoral arthritis present with different symptom patterns (PF pain with stairs, TF pain with walking).
Quadriceps Force and Reaction Force
The quadriceps muscle group is the primary force generator at the knee:
During gait, the quadriceps must:
- Absorb impact during early stance (eccentric contraction)
- Stabilize knee during mid-stance (isometric contraction)
- Extend knee for push-off (concentric contraction in terminal stance)
The quadriceps force can be 3-4x body weight during these activities, contributing to the total knee reaction force through the patellar mechanism.
Biomechanical Calculation Example: Standing from a chair (60-degree knee flexion):
- Quadriceps force required: approximately 4x BW
- Patellar contact force: Fq × sin(60°/2) ≈ 4 × 0.5 = 2x BW
- Tibiofemoral compression: 3-4x BW (vector sum of forces)
Effect of Alignment on Knee Forces
Coronal plane alignment critically affects medial vs lateral compartment loading:
- Mechanical Axis
- Through knee center
- Medial Compartment Force
- 60% of total force
- Lateral Compartment Force
- 40% of total force
- Mechanical Axis
- Medial to knee center
- Medial Compartment Force
- 70-90% of total force
- Lateral Compartment Force
- 10-30% of total force
- Mechanical Axis
- Lateral to knee center
- Medial Compartment Force
- 30-40% of total force
- Lateral Compartment Force
- 60-70% of total force
- Mechanical Axis
- Through prosthesis center
- Medial Compartment Force
- Equal distribution
- Lateral Compartment Force
- Equal distribution
Clinical Implications:
- Varus malalignment overloads medial compartment, accelerating medial OA progression
- Lateral compartment unloading in varus knees leads to medial bone loss and deformity progression
- Total knee replacement aims to restore neutral alignment for equal load distribution
- High tibial osteotomy shifts mechanical axis laterally to unload diseased medial compartment
Shoulder Joint Reaction Forces
Unique Characteristics of Shoulder Biomechanics
The shoulder differs fundamentally from hip and knee:
Key Differences:
- Non-weight-bearing: Arm weight (approximately 5% of body weight) is much less than lower extremity loads
- Mobility over stability: Shallow glenoid socket prioritizes range of motion
- Muscular suspension: Rotator cuff and deltoid balance forces to center humeral head
- Variable loading: Forces depend heavily on arm position and external loads carried
Deltoid and Rotator Cuff Force Balance
The shoulder force equilibrium involves a unique interplay:
- Primary function: Arm elevation (abduction)
- Force direction: Superior (tends to pull humeral head upward into acromion)
- Magnitude: 2-3x arm weight during abduction
- Primary function: Humeral head compression and inferior pull
- Force direction: Medial and inferior (counteracts deltoid superior force)
- Magnitude: 1.5-2x arm weight
- Net effect: Compresses and centers humeral head on glenoid
The deltoid (superior force) and rotator cuff (inferior force) create a force couple that allows smooth elevation while maintaining glenohumeral joint stability. Rotator cuff tears disrupt this balance, allowing superior migration of the humeral head (superior escape).
Shoulder Reaction Force During Abduction
During shoulder abduction to 90 degrees:
Force Analysis:
- Arm weight: 5% BW = 35 N (for 70 kg person)
- Deltoid force: approximately 800-1000 N (to overcome arm weight moment)
- Rotator cuff force: approximately 600-800 N (to balance deltoid)
- Glenohumeral reaction force: 1-1.5x body weight (700-1000 N)
The reaction force is much lower than hip or knee because the arm weight is small. However, carrying external loads (groceries, tools, weights) dramatically increases the reaction force, potentially reaching 2-3x body weight.
Clinical Relevance to Shoulder Arthroplasty
Reverse shoulder replacement alters the normal biomechanics to compensate for a deficient rotator cuff:
- Medialized center of rotation: Reduces deltoid moment arm, reducing force needed
- Distal and lateral offset: Increases deltoid moment arm and pretensions deltoid for more efficient force generation
- Reaction force changes: Can increase contact force but distributes over larger glenosphere surface
- Net effect: Allows deltoid to elevate arm without functional rotator cuff
In anatomic shoulder replacement, posterior glenoid wear is common due to:
- Posterior subluxation tendency in osteoarthritic shoulders
- Eccentric loading (posterior force concentration)
- Increased reaction force magnitude on smaller contact area
- Component loosening risk if not corrected (posterior augmented glenoid components)
Clinical Implications for Arthroplasty
Bearing Surface Wear and Joint Forces
Polyethylene wear is directly proportional to joint reaction force magnitude:
Volumetric wear ∝ (Contact force × Sliding distance) / Material hardness
- Doubling body weight approximately doubles wear rate in THA
- High-impact activities (running, jumping) with forces of 6-10x BW cause disproportionate wear
- Obesity is a major risk factor for accelerated polyethylene wear and osteolysis
- Wear debris generation leads to osteolysis, aseptic loosening, and revision surgery
- Effect on Reaction Force
- Increases force proportionally
- Effect on Wear
- Linear increase in wear
- Clinical Action
- Weight loss before surgery; consider hard bearings
- Effect on Reaction Force
- Forces 6-10x BW
- Effect on Wear
- Exponential increase
- Clinical Action
- Activity modification; avoid polyethylene if young/active
- Effect on Reaction Force
- Reduces force 10-20%
- Effect on Wear
- Reduced wear rate
- Clinical Action
- Template carefully; prioritize offset in THR
- Effect on Reaction Force
- Reduces hip force 20-40%
- Effect on Wear
- Significant wear reduction
- Clinical Action
- Recommend during high-wear period (first 2 years)
Implant Fixation Requirements
Joint reaction forces determine the loads at the bone-implant interface:
- Cement mantle must withstand shear and compressive stresses from cyclical loads
- High reaction forces increase cement stress and creep (time-dependent deformation)
- Adequate cement thickness (2-4 mm) distributes stress; thin mantles crack
- Modern cementing technique emphasizes pressurization to improve bone-cement interdigitation
- Initial press-fit stability must resist motion under cyclical loading until osseointegration occurs
- Micromotion greater than 150 microns prevents bone ingrowth and causes fibrous encapsulation
- High reaction forces can exceed friction force, causing early migration and failure
- Porous coating and surface treatments (hydroxyapatite, trabecular metal) promote osseointegration
Stiff implants (e.g., cobalt-chrome stems) carry more load than surrounding bone due to elastic modulus mismatch. This reduces bone stress below threshold for remodeling (Wolff's law), causing proximal bone resorption. Joint reaction force magnitude influences extent of stress shielding.
Component Positioning and Biomechanics
Surgical technique directly affects postoperative joint reaction forces:
- Femoral offset: Every 5 mm reduction increases abductor force 15%, increasing reaction force and wear
- Limb length: Excessive lengthening increases abductor force; excessive shortening reduces efficiency
- Cup position: Excessive medialization reduces offset, increasing reaction forces
- Anteversion: Incorrect version alters force direction, causing edge loading and accelerated wear
- Alignment: Neutral mechanical axis ensures equal medial/lateral force distribution
- Joint line: Lowering joint line increases patellofemoral forces by altering patellar height
- Rotation: Internal rotation of femoral or tibial component alters patellar tracking and PF forces
- Slope: Posterior tibial slope affects anteroposterior stability and quadriceps force requirements
- Glenoid version: Retroversion increases posterior eccentric force, accelerating wear
- Humeral offset: Affects deltoid and rotator cuff lever arms, altering force requirements
- Reverse TSA lateralization: Optimal lateralization balances deltoid efficiency with reaction force magnitude
Strategies to Reduce Joint Reaction Forces
Patient Factors and Activity Modification
Weight Reduction: Every 1 kg of body weight lost reduces peak hip reaction force by 3-7 kg during gait. For an obese patient losing 10 kg:
- Hip force reduction: 30-70 kg peak load reduction
- Cumulative benefit: Millions of loading cycles over years
- Wear reduction: Proportional decrease in polyethylene wear rate
- Recommendation: Weight loss is the single most effective intervention for force reduction
Activity Guidelines:
- Peak Force
- 3-5x BW
- Recommendation Post-THA/TKA
- Encouraged, no limit
- Rationale
- Low impact, good for cardiovascular health
- Peak Force
- 1-2x BW
- Recommendation Post-THA/TKA
- Excellent option
- Rationale
- Low force, good ROM exercise
- Peak Force
- Minimal force
- Recommendation Post-THA/TKA
- Ideal exercise
- Rationale
- No impact, full body workout
- Peak Force
- 2-4x BW
- Recommendation Post-THA/TKA
- Acceptable with technique
- Rationale
- Moderate force, avoid twisting
- Peak Force
- 6-10x BW
- Recommendation Post-THA/TKA
- Not recommended
- Rationale
- High impact increases wear and loosening risk
- Peak Force
- 10x+ BW
- Recommendation Post-THA/TKA
- Contraindicated
- Rationale
- Extreme forces, high revision risk
Assistive Devices
Biomechanical effect:
- Creates upward force on opposite side, reducing body weight moment about stance hip
- Reduces hip abductor force requirement by 20-40%
- Reduces hip reaction force by 20-40% (proportional to reduction in abductor force)
- Technique: Cane in hand opposite to affected hip; advance cane with affected leg
- Bilateral support reduces force on each hip/knee by distributing weight across all four points
- Particularly effective during early postoperative period when bone ingrowth occurring
- Disadvantage: Slower gait, less efficient than cane for long-term use
- Cushioned soles with shock absorption reduce impact forces at heel strike
- Rocker-bottom soles reduce ankle and midfoot forces by smoothing push-off transition
- Effect is modest (5-10% force reduction) but may benefit marginal cases
Surgical Optimization
- Restore offset: Use appropriate femoral stem offset; consider high-offset stems for large patients
- Avoid medialized cups: Maintain hip center of rotation near anatomic position
- Optimize limb length: Match contralateral side; avoid excessive lengthening (increases force) or shortening (reduces abductor efficiency)
- Consider hard bearings: Ceramic or metal bearings for young, high-demand patients to resist wear from high forces
- Neutral alignment: Restore mechanical axis to knee center for equal compartment loading
- Maintain joint line: Avoid distal femoral over-resection that lowers joint line and increases PF forces
- Optimize rotation: Correct femoral and tibial component rotation for optimal patellar tracking
- Consider constraint level: Higher forces may require more constrained designs (PS vs CR)
- Reverse for cuff deficiency: Alters biomechanics to reduce deltoid force requirements
- Optimize lateralization: Balance force efficiency with glenoid stress in reverse TSA
- Correct glenoid version: Avoid posterior glenoid wear by addressing retroversion
Management Algorithm
Guidelines, Registries & Global Practice
Global Epidemiology
Joint reaction forces are the mechanical driver behind load-related cartilage degeneration, so the global burden of osteoarthritis (OA) frames their clinical importance. According to PubMed, the Global Burden of Disease 2019 analysis reports age-standardised prevalence per 100,000 of approximately 4376 for knee OA, 1726 for hand OA and 401 for hip OA, with hip and knee OA prevalence rising significantly between 1990 and 2019 (Li XX et al., Int J Rheum Dis 2024 DOI). High body-mass is a leading modifiable contributor: increased body weight raises every lower-limb joint reaction force in direct proportion, accelerating OA and, after arthroplasty, bearing wear. Obesity prevalence is high in many high-income countries (around 30% of adults), magnifying joint loading at a population level.
Guideline Positions (Side by Side)
There is no joint-reaction-force-specific guideline; the principles are operationalised within OA management and arthroplasty optimisation guidance. The table summarises how major bodies translate the underlying biomechanics into practice.
- Relevant Guidance
- Management of OA of the hip and knee
- Stance on Load Reduction
- Strongly recommends weight loss and low-impact exercise to reduce joint loading; supports patient-specific activity counselling
- Evidence Level
- Moderate-strong
- Relevant Guidance
- Osteoarthritis: assessment and management (NG226)
- Stance on Load Reduction
- Therapeutic exercise and weight management are core first-line; offers arthroplasty when conservative load-modifying measures are insufficient
- Evidence Level
- Moderate
- Relevant Guidance
- Best-practice arthroplasty standards
- Stance on Load Reduction
- Emphasise restoring offset, leg length and alignment to normalise muscle and joint reaction forces
- Evidence Level
- Consensus
- Relevant Guidance
- Consensus on hip and knee biomechanics
- Stance on Load Reduction
- Endorse biomechanical optimisation (offset, alignment) and pre-operative risk-factor modification
- Evidence Level
- Consensus
- Relevant Guidance
- Hip and knee wear-simulator standards
- Stance on Load Reduction
- Codify in vivo telemetry force profiles (Bergmann, Kutzner) into mandatory implant testing
- Evidence Level
- Standard
Registry Evidence
National arthroplasty registries provide the largest real-world signal that joint loading governs implant survival. According to PubMed, an Australian-led meta-analysis of more than 3.1 million total knee arthroplasties found higher all-cause revision (OR 1.15) and deep infection (OR 1.47) in obese patients (Onggo JR et al., ANZ J Surg 2021 DOI). Registry observations consistent with force principles include:
- AOANJRR (Australia): higher cumulative revision in high-BMI patients and in younger, higher-demand recipients, and better survivorship when normal biomechanics (offset, alignment) are restored.
- NJR (England, Wales, NI) and AJRR (USA): report increased early revision for instability and loosening with malposition, the mechanism of which is altered moment arms and reaction-force direction.
- Bearing-surface trends (hard-on-hard or highly cross-linked polyethylene for young, active patients) reflect the force-wear relationship (Archard's law).
Practice Variation and Controversies
- Mechanical versus kinematic alignment in TKA: instrumented-implant data (Kutzner et al., Bone Joint J 2017) show varus malalignment raises the medial force ratio, fuelling debate over how much constitutional varus is safe to leave.
- BMI thresholds for elective arthroplasty: some systems apply hard BMI cut-offs while others reject them as inequitable; evidence for force-driven complications informs but does not settle this.
- Offset targeting: increasing femoral offset reduces abductor and reaction force but risks trochanteric pain and leg-length issues, so targets vary between centres.
Pre-operative and Conservative Optimisation
- Pre-operative weight optimisation and dietitian input are increasingly embedded in arthroplasty pathways internationally to lower joint reaction forces before surgery.
- Physiotherapy-led gait retraining and contralateral cane education reduce hip joint reaction force conservatively.
- Multimodal analgesia supports the activity modification and load-reduction programmes that underpin conservative OA care before arthroplasty.
MCQ Practice Points
Q: What is the hip joint reaction force during single-leg stance and why is it so high?
A: Approximately 2.5-3× body weight. High because of mechanical disadvantage: Body weight (minus stance leg ~55 kg for 70 kg person) acts through moment arm ~10-12 cm from hip. Abductors have moment arm only ~5 cm. To balance, abductors must generate ~2× BW force. Joint reaction force = vector sum of body weight + abductor force, directed superolaterally. During walking, peak force reaches 3-7× BW.
Q: Compare the joint reaction forces at the hip, knee, and ankle during normal gait.
A: Hip: 3-7× BW walking, up to 10× BW stumbling. Knee: 2-3× BW walking, 3-4× stairs, 6-8× running. Ankle: 4-5× BW walking, 8-13× BW running - highest forces in lower limb. Ankle forces are highest due to long lever arm of forefoot and short Achilles moment arm. These values guide implant design and fixation strength requirements.
Q: How does using a walking stick in the opposite hand reduce hip joint reaction force?
A: A walking stick on the contralateral side creates an external moment that assists the hip abductors. Using only 10-15% of body weight through the stick can reduce hip joint reaction force by 20-30%. The stick effectively reduces the moment arm of body weight that abductors must counter. This is why osteoarthritis patients intuitively use a stick on the opposite side.
Q: What forces act on the knee joint during stair climbing?
A: 3-4× body weight. Higher than level walking because: 1) Greater knee flexion angle increases patellofemoral forces, 2) Quadriceps must generate high force to extend knee against gravity, 3) Body weight acts through longer moment arm in flexion. Patellofemoral joint force during stair descent can reach 7-8× BW. Clinical relevance: early symptom in patellofemoral OA, TKA rehabilitation.
Q: How does contact area affect contact stress in the hip joint?
A: Contact stress = Force / Contact area. In the normal hip, joint reaction force is distributed over 70-80% of available articular surface area. In hip dysplasia, reduced coverage concentrates force over smaller area, dramatically increasing contact stress and accelerating cartilage damage. Periacetabular osteotomy increases coverage area, reduces peak contact stress, and delays or prevents OA.
At a Glance
Joint reaction force is the resultant force acting across a joint, calculated using free body diagrams and static equilibrium equations (ΣF = 0, ΣM = 0). Forces far exceed body weight due to short muscle lever arms: the hip experiences 3-7x body weight during gait, the knee 2-4x during walking, and the ankle 4-5x during normal activities. These magnitudes drive bearing surface wear in arthroplasty, implant fixation requirements, and the progression of osteoarthritis. Clinically, forces can be reduced through contralateral cane use (20-30% reduction), weight loss, increased hip offset (reducing abductor force required), and avoiding high-impact activities.
FEMURJoint Reaction Force Calculation
Hook:Use FEMUR method to calculate joint reaction forces in biomechanics viva!
MODALFactors Increasing Joint Reaction Forces
Hook:MODAL factors increase joint reaction forces and implant stress!
CLAWReducing Joint Reaction Forces Clinically
Hook:Use your CLAW to reduce joint reaction forces in arthroplasty patients!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 70 kg patient is standing on one leg. The moment arm of body weight about the hip joint center is 12 cm. The moment arm of the hip abductor muscles is 5 cm. Calculate the hip abductor muscle force and the total hip joint reaction force. Assume static equilibrium and forces acting in vertical plane only.”
“You are planning a total hip replacement in a 45-year-old male tradesman, 95 kg, BMI 32, who wishes to return to physically demanding work involving repetitive lifting and carrying. Discuss how joint reaction forces influence your choice of bearing surface and surgical technique.”
“An examiner asks you to explain the biomechanical principle of how a contralateral cane reduces hip joint reaction forces. Draw a free body diagram and explain the mechanism.”
Core Definitions
- Joint reaction force = resultant force across joint surface from external + internal loads
- Calculated using free body diagrams and equilibrium (ΣF=0, ΣM=0)
- Magnitude FAR EXCEEDS body weight due to muscle forces and leverage
- Primary clinical relevance: implant wear, fixation loads, component design
Force Magnitudes (Multiples of Body Weight)
- Hip: 2.5x BW standing one leg; 3-7x BW normal gait; 8-10x BW stumbling
- Knee: 2-3x BW walking; 3-4x BW stairs; 6-8x BW running; 24x BW jump landing
- Ankle: 4-5x BW walking; 8-13x BW running (higher than hip/knee!)
- Shoulder: 0.5-1.5x BW (non-weight-bearing, lower forces)
Hip Biomechanics - Essential Facts
- Abductor muscles (glut med/min) prevent pelvic drop during single-leg stance
- Abductor moment arm ~5 cm; body weight moment arm ~12 cm (2.5:1 ratio)
- Mechanical disadvantage requires abductor force = 2-3x body weight
- Hip reaction = abductor force + body weight = 3-4x BW static, 3-7x BW gait
- Peak force at mid-stance phase of gait cycle (single leg support)
Free Body Diagram Calculation Steps
- 1. Isolate segment; draw all forces (W, Fm, R)
- 2. Define coordinate system and measure moment arms
- 3. ΣM=0 about joint: Solve for muscle force Fm
- 4. ΣF=0: Solve for reaction force R (R = Fm + W for vertical)
- 5. Combine components if 2D/3D to get resultant magnitude
Factors Increasing Reaction Forces
- Obesity (proportional increase - 1 kg weight = 3-7 kg peak hip force)
- High-impact activities (running 6-8x BW, jumping 10-24x BW)
- Reduced offset/moment arm (medialized cup, coxa vara)
- External loads carried (groceries, tools, weights)
- Malalignment (varus knee overloads medial compartment)
Reducing Forces Clinically
- Weight loss (single most effective: 1 kg lost = 3-7 kg force reduction)
- Contralateral cane (reduces hip force 20-40% via opposing moment)
- Activity modification (walk vs run; avoid impact sports post-arthroplasty)
- Surgical optimization: restore offset, maintain alignment, optimize biomechanics
- Assistive devices (walker, cane, shoe cushioning)
THR/TKR Biomechanical Principles
- Restore femoral offset: 5 mm reduction increases force 15%, accelerates wear
- Neutral alignment TKR: equal medial/lateral distribution prevents overload
- Bearing surface selection: hard bearings (ceramic) for high forces/young patients
- Component position affects moment arms and force distribution
- Wear proportional to force (Archard's law): High forces = high wear rate
Exam Mnemonics
- FEMUR: Free body, Equilibrium, Moment arms, Unknown reaction, Resultant
- MODAL: Muscle forces, Obesity, Dynamic activities, Anatomical factors, Load carrying
- CLAW: Cane, Lateralize rotation center, Avoid impact, Weight reduction
- Hip forces: 3-7 BW gait (remember 'three to seven steps')
Viva Traps to Avoid
- Stating R = Fm - W (WRONG! R = Fm + W, both compress joint)
- Forgetting to convert kg to Newtons (× 9.8 m/s²)
- Ipsilateral cane reduces force (NO! Must be contralateral)
- Joint force equals body weight (NO! Forces are multiples of BW)
- Not drawing free body diagram when asked by examiner
Evidence Base and Key Studies
Bergmann Hip Contact Force Telemetry (Landmark In Vivo Dataset)
- Direct in vivo measurement of hip contact forces using instrumented femoral implants with telemetry in four patients during activities of daily living
- Average peak hip contact force walking at about 4 km/h: 238% body weight
- Stair ascent 251% BW; stair descent 260% BW (descent exceeds ascent)
- Implant torsion about the stem axis is approximately 23% greater on stair ascent than level walking, a key driver of stem fixation failure
Kutzner In Vivo Tibiofemoral Loading (Landmark Knee Dataset)
- Instrumented TKA with telemetry measured tibiofemoral contact forces in five subjects during activities of daily living
- Peak resultant force highest on stair descent (346% BW), then stair ascent (316% BW) and level walking (261% BW)
- Resultant force acted almost vertically on the tibial plateau even in high flexion; shear forces were 10-20 times smaller than the axial force
- In vivo dynamic forces were generally lower than predicted by many mathematical models, but exceeded several existing implant test standards
Kutzner: Coronal Alignment Drives Mediolateral Force Distribution
- Instrumented TKA in nine patients with full-leg coronal radiographs
- Medial force ratio correlated strongly with tibiofemoral alignment in one-legged stance (R-squared 0.88) and dynamic single-limb loading (R-squared 0.59)
- Varus malalignment increased the medial force ratio to as much as 88% of total load
- Force shifted laterally during double-limb support and higher flexion angles
Obesity, Joint Loading and Arthroplasty Outcomes (Large Meta-Analysis)
- Meta-analysis of 91 studies and over 3.1 million total knee arthroplasties (Australian-led, AOANJRR-linked authors)
- Obese patients (BMI 30 or more) had higher all-cause revision risk (OR 1.15, 95% CI 1.08-1.24)
- Deep infection risk increased (OR 1.47); morbid obesity (BMI 40 or more) raised deep infection risk further (OR 1.98)
- Higher rates of complications, readmission and wound problems, consistent with elevated mechanical joint loading plus metabolic risk
Asayama: Reconstructed Hip Geometry and Abductor Strength after THA
- 60 limbs in 30 unilateral THA patients with a normal contralateral hip compared radiographically and by dynamometry
- The ratio of femoral offset to the body-weight lever arm correlated positively with abductor strength ratio (r 0.49, p 0.006)
- The ratio of hip-centre height to pelvic height correlated negatively with strength (r -0.57, p 0.001)
- Slightly increased offset with restoration of a normal, slightly inferomedial hip centre optimised abductor function
Neumann: Contralateral Cane Reduces Hip Abductor Demand
- Randomised crossover EMG study of 24 subjects with a unilateral hip prosthesis
- Cane held contralateral to the prosthesis reduced hip abductor EMG activity by 31% versus walking with no cane
- Near-maximal contralateral cane effort reduced abductor activity by 42%
- An ipsilateral cane produced no significant reduction, confirming the cane must be on the opposite side
Bergmann: First In Vivo Glenohumeral Contact Forces
- First worldwide in vivo measurement of glenohumeral contact force using an instrumented shoulder implant with telemetry
- Contact force remained below 100% body weight for most activities of daily living
- Force rose to about 130% BW near the limits of motion or against external resistance
- Peak of about 150% BW occurred when turning a blocked steering wheel with maximal effort
Global Burden of Osteoarthritis (GBD 2019)
- GBD 2019 age-standardised prevalence per 100,000: knee OA 4376, hand OA 1726, hip OA 401
- Hip and knee OA prevalence rose significantly from 1990 to 2019 (hip AAPC +0.43%, knee +0.17%)
- Europe and the Americas carry the highest hip OA burden; Asia has a high knee OA burden
- High body-mass is a leading modifiable contributor to OA disability worldwide