The Infiltrative Sarcoma of the Elderly
- Myxofibrosarcoma (MFS, formerly 'myxoid malignant fibrous histiocytoma') is one of the COMMONEST soft-tissue sarcomas of the ELDERLY (typically 60s-80s), arising in the subcutaneous or deep soft tissues of the EXTREMITIES (lower limb more than upper) and trunk; histologically it has a MYXOID stroma with curvilinear blood vessels and pleomorphic spindle cells.
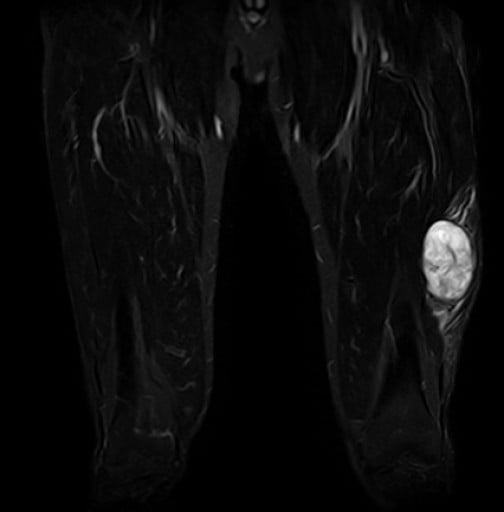
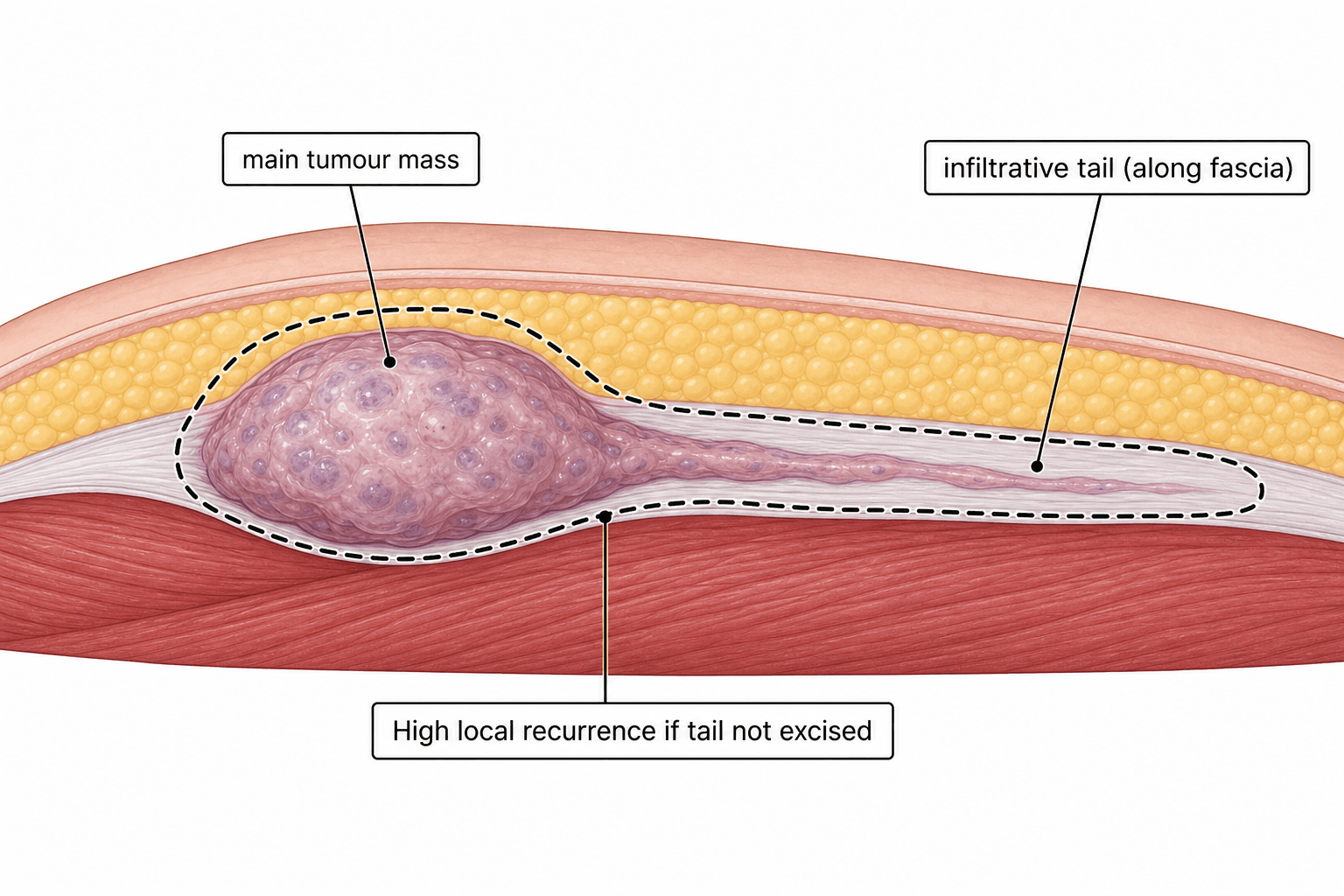
- Its defining feature is an INFILTRATIVE GROWTH PATTERN that extends along FASCIAL planes far beyond the clinically/radiologically obvious mass - sometimes visible on MRI as the 'TAIL SIGN' (a fascial 'tail' of tumour) - which makes the true extent easy to UNDERESTIMATE and underlies its VERY HIGH LOCAL RECURRENCE rate. Critically, the tail sign is seen in FEWER THAN HALF of cases: its ABSENCE does NOT mean the tumour is contained, and must never justify a closer margin.
- On MRI the lesion is typically T2/STIR HYPERINTENSE (reflecting the myxoid content); the presence and extent of an infiltrative tail and of perilesional oedema are prognostically important, and DIFFUSE perilesional oedema is associated with WORSE survival - so detailed pre-operative MRI is essential to plan an adequate resection.
- MFS spans a GRADE spectrum from low to high; LOCAL RECURRENCE is high across grades, while DISTANT METASTASIS (especially to the LUNG) increases with grade, and low-grade tumours can recur at a HIGHER grade over time.
- TREATMENT is WIDE LOCAL EXCISION with GENEROUS margins planned on pre-operative MRI to encompass the infiltrative tail - inadequate margins frequently cause recurrence - usually combined with RADIOTHERAPY (neoadjuvant or adjuvant) for high-grade or large/deep tumours; chemotherapy has a limited role.
- Because of the infiltrative tail and high recurrence, these patients need MULTIDISCIPLINARY (sarcoma MDT) care, meticulous margin assessment, and LONG-TERM follow-up with surveillance imaging for both local recurrence and pulmonary metastases.
- “Myxofibrosarcoma = common soft-tissue sarcoma of the ELDERLY (extremities); myxoid stroma + curvilinear vessels.
- “Infiltrative growth along fascia -> MRI 'TAIL SIGN' (T2/STIR-bright myxoid mass) -> margins underestimated -> very high LOCAL recurrence.
- “Treat with WIDE excision (MRI-planned generous margins) + radiotherapy; metastatic risk (lung) rises with grade; long-term follow-up.
MFS spreads with an infiltrative tail along fascia beyond the visible mass (the MRI 'tail sign'), so margins are underestimated -> very high local recurrence. The sign is seen in fewer than half of cases - its absence proves nothing.
Pre-operative MRI to map the tail, wide excision with generous margins to encompass it, plus radiotherapy for high-grade/large tumours.
Presentation, Imaging & Behaviour
Myxofibrosarcoma typically presents as a slowly enlarging soft-tissue mass in the extremity (often subcutaneous) of an elderly patient. Histologically it has a myxoid stroma with characteristic curvilinear vessels and pleomorphic spindle cells, and it spans a spectrum from low to high grade. Its hallmark is the infiltrative growth along fascial planes that produces the MRI 'tail sign' - a fascial tail of tumour extending beyond the main mass - so the true extent is easily underestimated. On MRI the lesion is typically T2/STIR hyperintense (myxoid content), and diffuse perilesional oedema is associated with a worse prognosis. The infiltrative behaviour drives a very high local recurrence rate, while distant metastasis (especially lung) increases with grade.
The Tail Sign Is Absent in More Than Half - and That Changes Nothing About the Margin
The tail sign is the memorable feature of this tumour, and it is the single most misleading one, because a study that reviewed pre-operative MRI specifically looking for it found it in fewer than half of cases. The infiltration, however, is present regardless. What varies is whether it happens to be visible.
Absence of a tail sign is not evidence of a contained tumour. The infiltration that drives recurrence is microscopic extension along fascial planes; a "tail" is only what that extension looks like when enough of it is confluent, oedematous and long enough to be resolved on MRI. A tumour whose infiltration is short, patchy or oriented out of the imaged plane produces no tail and precisely the same recurrence problem. Reading a tail-free MRI as permission for a closer margin is the error the sign invites.
- What it tells you
- Infiltration confirmed and partly mapped - resect to include it, and beyond it
- What it does NOT license
- Assuming the tail's visible end is the tumour's true end; the microscopic front lies further
- What it tells you
- Nothing reassuring. More than half of these tumours never show one
- What it does NOT license
- Reducing the margin, or treating the lesion as circumscribed
- What it tells you
- Adverse prognostic sign - associated with significantly worse overall survival than circumscribed oedema
- What it does NOT license
- Dismissing it as reactive change; it may harbour tumour and it marks a worse-behaving lesion
- What it tells you
- Better prognostic group than diffuse
- What it does NOT license
- Concluding the disease is confined - oedema pattern is prognostic, not a margin map
The practical resolution is that the margin is dictated by the tumour type, not by whether a tail was seen. Plan the resection on the assumption that infiltration extends beyond what is visible, take the investing fascia as a barrier where anatomy allows, and let a visible tail extend the resection rather than let its absence contract one.
The Differential of a T2-Bright Myxoid Soft-Tissue Mass
A bright, myxoid-looking soft-tissue mass on T2/STIR has a specific differential, and the trap is to dismiss it as a benign intramuscular myxoma. The discriminators are the patient's age, the depth/site, the internal architecture (curvilinear vessels, fatty foci, enhancing nodules) and, increasingly, the cytogenetics. Route the individual entities to their dedicated topics; the message here is that a deep, enhancing or infiltrative myxoid mass in an adult must be assumed malignant until a sarcoma unit proves otherwise.
- Typical patient / site
- Elderly (60s-80s); subcutaneous/deep extremity
- Discriminating clue
- Infiltrative fascial TAIL; curvilinear vessels + pleomorphic cells
- What it means for management
- Wide excision with margins planned on MRI to include the fascial tail - it is the tail extending beyond the palpable mass that drives the high local recurrence rate - plus radiotherapy
- Typical patient / site
- Younger adults (30s-50s); deep thigh
- Discriminating clue
- Fatty foci within a myxoid mass; t(12;16) FUS-DDIT3
- What it means for management
- Sarcoma-unit referral and wide excision, but it is radiosensitive and metastasises unusually - to other soft tissue and bone rather than lung - so staging must image the whole body, not just the chest
- Typical patient / site
- Adults; deep extremity (thigh)
- Discriminating clue
- Multinodular myxoid mass; EWSR1-NR4A3 fusion
- What it means for management
- Wide excision at a sarcoma unit, and counsel for the long haul - it is indolent but recurs and metastasises late, so surveillance runs for decades rather than the usual five years
- Typical patient / site
- Younger adults; deep soft tissue
- Discriminating clue
- Deceptively BLAND but malignant; late mets; FUS-CREB3L2
- What it means for management
- Treat as a sarcoma despite bland histology - the trap is that a pathologist without the fusion result may report something reassuring, and marginal excision of a lesion that metastasises 10-15 years later is the consequence
- Typical patient / site
- Middle-aged; intramuscular (thigh)
- Discriminating clue
- Hypocellular, NO curvilinear vessels / minimal enhancement; Mazabraud if multiple + fibrous dysplasia
- What it means for management
- Benign - marginal excision if symptomatic, and no radiotherapy. Do not subject this patient to a sarcoma resection
- Typical patient / site
- Young adults; rapid growth
- Discriminating clue
- Self-limiting; USP6 rearrangement
- What it means for management
- Benign and often self-resolving - observation or simple excision. Rapid growth and brisk mitoses here mean regeneration, not malignancy
Management
- Pre-operative MRI to define the mass AND the infiltrative tail and perilesional oedema, and to plan the resection.
- Wide local excision with generous margins that encompass the infiltrative tail - because the extent is underestimated, inadequate margins are the main cause of recurrence.
- Radiotherapy (neoadjuvant or adjuvant) for high-grade, large or deep tumours and for close/positive margins (see Radiotherapy in MSK Tumours for the neoadjuvant-versus- adjuvant trade-off).
- Chemotherapy has a limited role (selected high-grade/advanced disease).
- Multidisciplinary sarcoma care and long-term follow-up with surveillance for local recurrence and pulmonary metastases.
The recurring error with myxofibrosarcoma is to excise to the apparent edge of the mass and miss the infiltrative fascial tail, which leads to repeated local recurrence. Always assess the full extent on pre-operative MRI, plan a wide excision that includes the tail, and obtain clear histological margins; treat high-grade or large tumours within a sarcoma multidisciplinary team with radiotherapy, and follow patients long-term for both local recurrence and lung metastases. Remember that a low-grade lesion can recur at a higher grade, so recurrence should be re-staged and re-graded rather than assumed to be the same disease.
Before Any of That: the Lump That Gets Shelled Out as a Lipoma
Everything above concerns getting the margin right at a planned operation. The commonest way the margin is lost in practice is that the planned operation is the second one.
Myxofibrosarcoma is frequently subcutaneous, painless and slow-growing, in an elderly patient who has had lumps before - which is a near-perfect description of a lipoma or an epidermoid cyst. Excised as one, in a setting without pre-operative imaging, it leaves tumour in a contaminated bed with the fascial infiltration untouched. This tumour's superficial habit makes it more exposed to that error than the deep-seated sarcomas that look alarming from the outset.
The referral thresholds are the same ones used for any soft-tissue mass, and a lesion needs only one of them: greater than 5 cm, deep to the fascia, enlarging, painful, or recurrent after previous excision. Image with contrast-enhanced MRI and refer to a sarcoma unit before cutting. A small superficial lump can still be a sarcoma when the behaviour is atypical, which is exactly the situation here - so size alone must not be the deciding factor in an older patient with a growing subcutaneous mass.
If myxofibrosarcoma is diagnosed on the histology of a lump that has already been shelled out, the correct response is not surveillance, however clean the margins are reported and however normal the post-operative scan looks. After an unplanned excision with apparently negative margins and no visible residual disease on imaging, planned re-excision still finds residual sarcoma in roughly a third of patients, and this cannot be predicted from tumour size, grade or the interval since surgery.
The pathway is: restage (including CT chest), MRI of the tumour bed, refer to the sarcoma MDT, and perform a planned wide re-excision of the entire previous surgical bed - the scar, the drain sites and the contaminated planes - usually with adjuvant radiotherapy. The infiltrative biology that makes a first margin difficult makes a contaminated field worse, not easier.
Biopsy, when it is done properly. An unknown mass meeting any red flag is diagnosed by image-guided core needle biopsy, not by excision. The tract must be placed in line with the future resection incision by, or in discussion with, the surgeon who will perform the definitive operation, so that the tract can be excised en bloc. A transversely placed or casually sited tract contaminates compartments that were not involved and can convert a limb-salvage resection into a much larger one. (The full principles, including the residual-disease data above, are in Biopsy Principles and Techniques and Soft Tissue Masses and Sarcoma Referral.)
How Myxofibrosarcoma Is Graded (FNCLCC) and Why It Matters
Prognosis hangs on grade - metastatic risk rises with it, and a low-grade lesion can recur at a higher grade - so you need to know how a soft-tissue sarcoma like myxofibrosarcoma is graded. The standard histological system is the FNCLCC grade (Federation Nationale des Centres de Lutte Contre le Cancer), which scores three parameters and sums them into a three-tier grade. Surgical/anatomical staging (the Enneking and AJCC systems) is a separate axis - see Enneking Staging - whereas FNCLCC is the histopathological grade that prognosis here depends on.
- Tumour differentiation (scored one to three: the closer the tumour resembles normal mesenchymal tissue, the lower the score).
- Mitotic count per ten high-power fields (one for fewer than 10; two for 10 to 19; three for 20 or more).
- Tumour necrosis (zero for none; one for up to half the tumour; two for more than half).
The three scores are summed: a total of two to three is grade 1, four to five is grade 2, and six to eight is grade 3. Higher grade means greater risk of distant (lung) metastasis and a stronger case for adjuvant radiotherapy and/or chemotherapy within the sarcoma MDT.
FNCLCC grade = differentiation + mitoses + necrosis, summed into grade 1 to 3. Because a myxofibrosarcoma can recur at a higher grade, a recurrence should be re-biopsied and re-graded rather than assumed to be the same disease - the grade, not just the diagnosis, drives the metastatic-surveillance and adjuvant plan.
Mnemonics & Memory Aids
TAIL
Hook:Myxofibrosarcoma = the TAIL sarcoma of the elderly.
MYXOID
Hook:MYXOID: bright on MRI, elderly, eXtensive tail, oedema = poor prognosis.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is myxofibrosarcoma, what is the 'tail sign', and why does it have a high local recurrence rate?”
“How would you manage a high-grade myxofibrosarcoma of the thigh?”
Demographics & histology
- One of the commonest soft-tissue sarcomas of the ELDERLY (60s-80s)
- Extremities (lower more than upper) and trunk; subcutaneous/deep
- Myxoid stroma + curvilinear vessels + pleomorphic spindle cells; low-to-high grade
Imaging
- MRI: T2/STIR hyperintense (myxoid)
- 'Tail sign' = infiltrative fascial spread beyond the mass - but present in FEWER THAN HALF; absence never justifies a closer margin
- Diffuse perilesional oedema = worse survival than circumscribed oedema
Before you cut
- Often SUBCUTANEOUS in an elderly patient - the lump shelled out as a 'lipoma'
- Refer on any one of: over 5 cm, deep to fascia, enlarging, painful, recurrent
- After an unplanned excision: ~1/3 have residual tumour despite clear imaging - plan re-excision of the whole bed, do not observe
Behaviour
- Very high LOCAL recurrence (infiltrative tail underestimates extent)
- Distant metastasis (lung) increases with grade
- Low grade can recur at higher grade
Treatment
- Pre-operative MRI planning -> wide excision with generous margins (encompass tail)
- Radiotherapy (neo/adjuvant) for high-grade/large; chemo limited
- Sarcoma MDT; long-term surveillance (local + lung)
Evidence & Key Studies
Preoperative MRI evaluation of myxofibrosarcoma: prognostic value of imaging features
- Myxofibrosarcoma is characterised by an infiltrative growth pattern; the 'tail sign' was present in fewer than half of cases on MRI.
- Diffuse perilesional oedema on MRI was significantly associated with poorer overall survival (vs circumscribed oedema).
- Detailed pre-operative MRI with planning of the resection is a logical approach to achieve negative margins and recurrence-free survival.
Giant myxofibrosarcoma: infiltrative growth, wide margins and local recurrence
- Myxofibrosarcoma commonly arises in the extremities and has a high risk of local recurrence due to its infiltrative growth pattern; MRI showed the 'tail sign'.
- Wide-margin resection is essential, and insufficient margins frequently result in recurrence (this high-grade case recurred and was fatal).
- Highlights the importance of wide surgical margins given extensive infiltration, and the need for effective adjuvant therapy.
The infiltrative growth/tail sign, the prognostic value of perilesional oedema and the role of pre-operative MRI in planning margins come from the cited Muhlhofer study, and the high local recurrence with infiltrative growth and the need for wide margins from the cited Zhong case/review. The elderly/ extremity demographic, the myxoid histology, the grade-dependent metastatic risk and adjuvant radiotherapy are standard, well-established soft-tissue-sarcoma teaching. The finding that the tail sign appears in fewer than half of cases is from that same Muhlhofer study. The referral thresholds and the residual-disease rate after unplanned excision come from Soft Tissue Masses and Sarcoma Referral and Biopsy Principles and Techniques. (See also Liposarcoma, Extraskeletal Myxoid Chondrosarcoma, Intramuscular Myxoma and Enneking Staging.)