NR4A3-Rearranged Soft-Tissue Sarcoma
- EXTRASKELETAL MYXOID CHONDROSARCOMA (EMC) is a RARE soft-tissue SARCOMA that, DESPITE its name, does NOT show true cartilaginous (hyaline-cartilage) differentiation - it is a distinct entity of uncertain differentiation, defined molecularly rather than by cartilage formation.
- It is characterised by NR4A3 GENE REARRANGEMENT - most commonly the EWSR1-NR4A3 fusion, with FUS-NR4A3 and other rarer variant partners (e.g. TAF15-NR4A3) - and this NR4A3 rearrangement is the molecular hallmark used to confirm the diagnosis.
- It typically presents as a DEEP soft-tissue MASS of the PROXIMAL LIMBS and limb GIRDLES (especially the THIGH) in adults, often slowly enlarging; the imaging is of a deep, often lobulated, myxoid (T2-bright) soft-tissue mass.
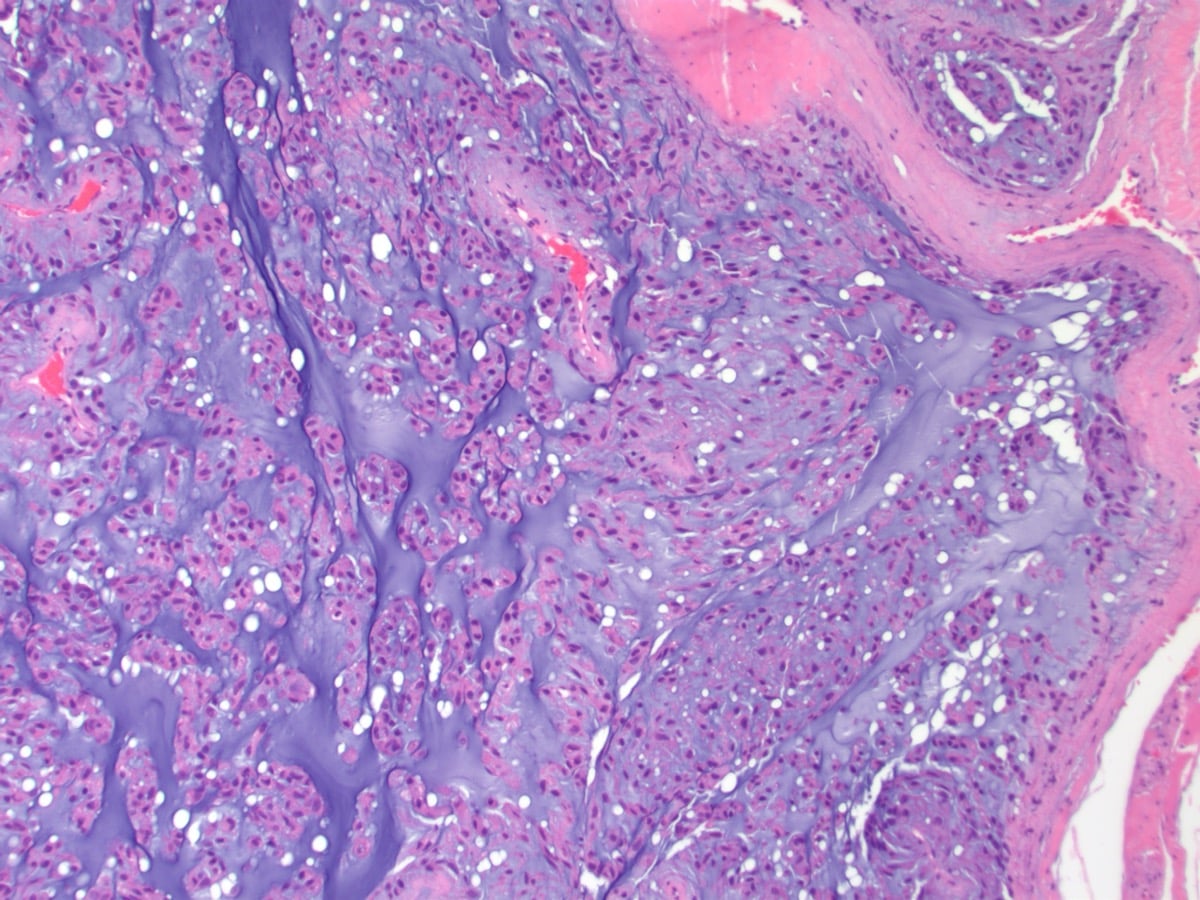
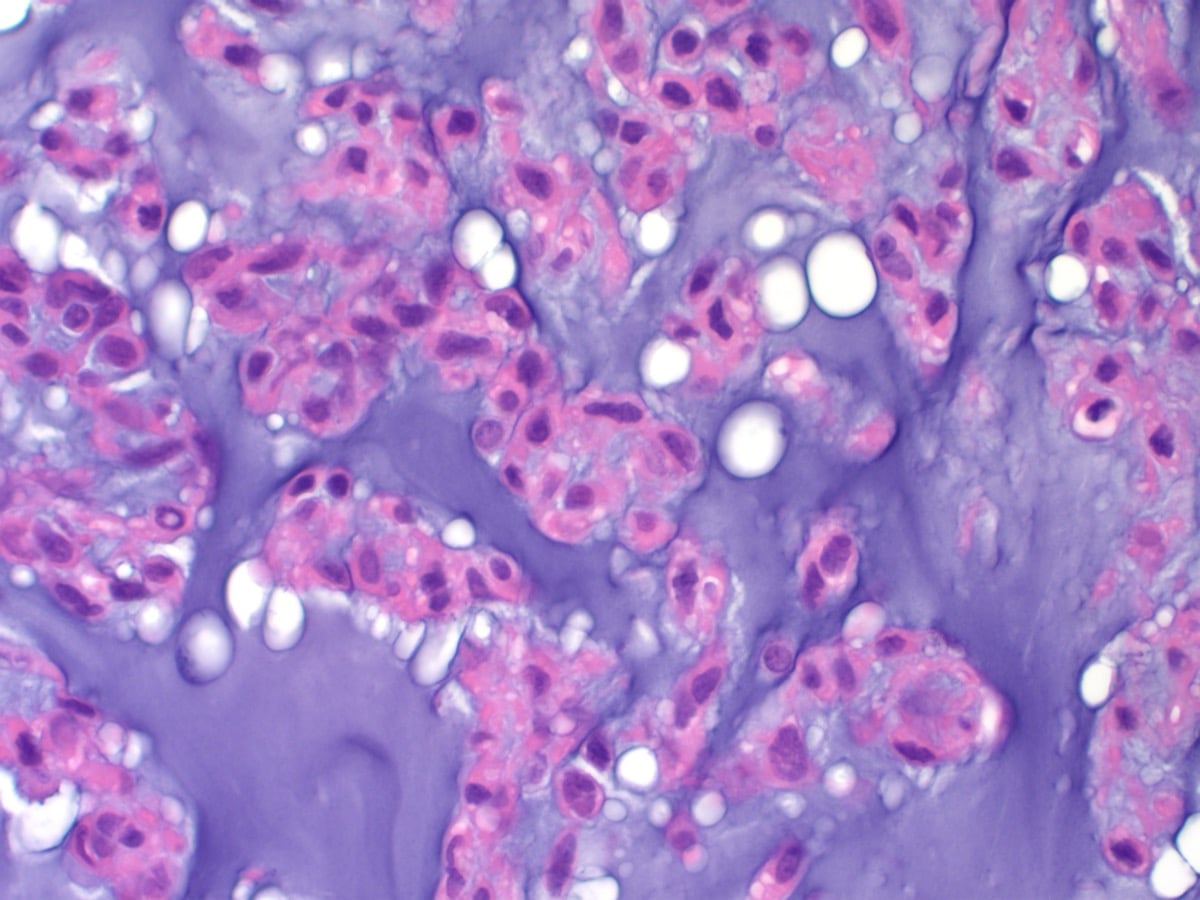
- HISTOLOGY shows a MYXOID matrix with a MULTILOBULAR architecture and CORDS, clusters or reticular arrays of relatively uniform eosinophilic OVOID-to-short-SPINDLE cells; immunohistochemistry is variable (e.g. variable CD117/S100), and morphological variants (rhabdoid, cellular/'high-grade', spindle) and rare non-EWSR1 fusions exist, so the molecular NR4A3 finding is valuable.
- PUT NUMBERS ON 'INDOLENT BUT RELAPSING' - AND NOTE THAT 'INDOLENT' UNDERSELLS IT. In a 117-case series with a median follow-up of 9 years (up to 22), estimated survival was 90 PERCENT at 5 years but 70 PERCENT at 10 and 60 PERCENT at 15; LOCAL RECURRENCE occurred in 48 percent (40 of 83), and 58 percent of those recurred MORE THAN ONCE; METASTASES occurred in 46 percent (35 of 76). The authors concluded that the high eventual death rate DISTINGUISHES EMC FROM LOW-GRADE SARCOMAS - so 'indolent' describes the tempo, not the eventual outcome, and prolonged surveillance follows from that.
- THE PROGNOSTIC FACTORS ARE CLINICAL, NOT HISTOLOGICAL. On multivariate analysis the adverse factors were OLDER AGE, LARGER TUMOUR SIZE and LOCATION IN THE PROXIMAL EXTREMITY OR LIMB GIRDLE - which is where 80 percent of these tumours arise, so the classic site is also the adverse one. METASTASIS reduced survival but LOCAL RECURRENCE did NOT. Critically, HISTOLOGIC GRADING WAS OF NO PROGNOSTIC VALUE in this series, so a report describing a 'cellular' or 'high-grade' variant should not be read as a worse prognosis; the cellular non-myxoid foci (seen in 29 percent) matter for RECOGNITION, since they mimic Ewing sarcoma, synovial sarcoma, fibrosarcoma and rhabdoid tumour.
- MANAGEMENT follows soft-tissue-sarcoma principles: MRI of the primary, a properly PLANNED BIOPSY at the treating sarcoma unit, and WIDE surgical RESECTION as the mainstay; EMC is relatively CHEMO/RADIO-RESISTANT, so radiotherapy/chemotherapy have a limited (selective) role, and LONG-TERM follow-up is essential because of late recurrence/metastasis - all within a specialist sarcoma multidisciplinary team.
- “Extraskeletal myxoid chondrosarcoma (EMC) = rare soft-tissue sarcoma; DESPITE the name it is NOT true cartilage. Defined by NR4A3 rearrangement (most often EWSR1-NR4A3; FUS/TAF15 variants).
- “Deep mass of the proximal limbs/girdles (thigh). Histology: myxoid + multilobular + cords/clusters of eosinophilic ovoid-spindle cells.
- “Indolent but RELAPSING long-term - local recurrence + LATE metastases (lung). Wide resection is the mainstay; chemo/radio-resistant; PROLONGED surveillance; sarcoma-centre care.
- “Quote the long tail: survival 90% at 5 years, 70% at 10, 60% at 15; local recurrence 48% (often repeated), metastases 46% (n=117, median follow-up 9 years). Adverse factors are older age, larger size and proximal-limb site - HISTOLOGIC GRADE has NO prognostic value, and local recurrence did not predict death.
Despite 'chondrosarcoma', EMC is not true cartilage - it is a distinct soft-tissue sarcoma defined by NR4A3 rearrangement (most often EWSR1-NR4A3).
Indolent but relapsing over the long term - local recurrence and late metastases (lung). Needs prolonged surveillance; it is chemo/radio-resistant (surgery is the mainstay).
What It Is, Genetics & Histology
EMC is a rare soft-tissue sarcoma that, despite its name, does not show true cartilage differentiation; it is a distinct entity defined by NR4A3 gene rearrangement (most often EWSR1-NR4A3, with FUS-NR4A3 and rarer variants). It presents as a deep mass of the proximal limbs/girdles (especially the thigh) in adults. Histology shows a myxoid, multilobular architecture with cords/clusters of eosinophilic ovoid-to-short-spindle cells (variable CD117/S100), and morphological/fusion variants exist - so the molecular NR4A3 finding is valuable. Its course is indolent but relapsing over the long term, with late recurrence/metastasis.
- Detail
- Uncertain - NOT true (hyaline) cartilage despite the name
- Detail
- NR4A3 rearrangement (EWSR1-NR4A3 most common; FUS/TAF15 variants)
- Detail
- Deep proximal limbs/limb girdles (especially thigh), adults
- Detail
- Myxoid, multilobular; cords/clusters of eosinophilic ovoid-spindle cells
- Detail
- Indolent but relapsing; local recurrence + late metastasis (lung)
- Detail
- Wide resection (mainstay); chemo/radio-resistant; long surveillance
The Myxoid Differential and the Immunoprofile
- The immunoprofile. EMC is characteristically CD117 (c-KIT)-positive in a proportion (about 30%), variably S100-positive, INI1 (SMARCB1)-retained, and negative for keratins/EMA and brachyury - which is the key to the differential.
- The myxoid-tumour differential. A tumour with cords/strands of cells in a myxoid matrix mimics several entities, separated by immunostains and fusion:
- Chordoma / myoepithelioma - keratin/EMA-positive (chordoma also brachyury-positive); EMC is keratin-negative.
- Myxoid liposarcoma - DDIT3 (FUS-DDIT3) fusion, "chicken-wire" vasculature and lipoblasts.
- Myxofibrosarcoma - curvilinear vessels and pleomorphism; no NR4A3.
- Low-grade fibromyxoid sarcoma - FUS-CREB3L2, MUC4-positive.
- Intramuscular myxoma / ossifying fibromyxoid tumour - benign; no NR4A3.
- The clincher. The NR4A3 rearrangement, with the keratin-/brachyury-negative, often-CD117-positive profile, confirms EMC and separates it from these mimics.
Q: How do you distinguish EMC from the other myxoid soft-tissue tumours?
A: EMC is CD117 (c-KIT)-positive in ~30%, variably S100-positive, INI1-retained, and keratin/EMA- and brachyury-NEGATIVE. That profile plus the NR4A3 rearrangement separates it from chordoma/myoepithelioma (keratin/EMA+, chordoma brachyury+), myxoid liposarcoma (DDIT3 fusion, lipoblasts, chicken-wire vessels), myxofibrosarcoma (curvilinear vessels, pleomorphism), and low-grade fibromyxoid sarcoma (FUS-CREB3L2, MUC4+).
The Long Tail, Quantified - and Why 'Indolent' Misleads
The word "indolent" describes how slowly this tumour moves, not how it ends. In a series of 117 cases with a median follow-up of 9 years (range 2 months to 22 years), estimated survival was 90 percent at 5 years, 70 percent at 10 and 60 percent at 15. Local recurrence occurred in 48 percent (40 of 83) and more than half of those patients recurred repeatedly; metastases occurred in 46 percent (35 of 76). The authors' own conclusion is the one to quote: the high rate of local recurrence, the prolonged survival even after metastasis, and the eventual high rate of death distinguish EMC from low-grade sarcomas. A five-year disease-free interval is therefore an interim result, not a discharge.
- Effect on survival
- Adverse, on multivariate analysis
- Note
- One of only three independent factors
- Effect on survival
- Adverse, on multivariate analysis
- Note
- Median size in the series was 7 cm (range 1.1 to 25)
- Effect on survival
- Adverse, on multivariate analysis
- Note
- Also the commonest site - 80 percent arose there, 20 percent in the trunk
- Effect on survival
- Adverse
- Note
- Yet survival after metastasis was prolonged in some patients
- Effect on survival
- NOT associated with worse survival
- Note
- Common (48 percent) and often repeated, but did not predict death
- Effect on survival
- NO prognostic value
- Note
- Prognosis is dictated by clinical features, not by grading
Q: The report describes a cellular, non-myxoid, 'high-grade-looking' area. Does that worsen the prognosis?
A: No - histologic grading was of no prognostic value in the largest series with long follow-up, where prognosis was dictated by age, size and site. Cellular, solid, non-myxoid foci were found in 29 percent of cases and resemble chondroblastoma, Ewing sarcoma, synovial sarcoma, fibrosarcoma and rhabdoid tumour - so their importance is diagnostic, not prognostic: recognising them prevents the tumour being misclassified as one of those mimics, which would lead to quite different treatment. Note too the demographics the name does not convey - a male-to-female ratio of 2 to 1, median age 52, median size 7 cm. The series is retrospective and predates routine NR4A3 testing, so some cases were classified morphologically.
Management
- Diagnosis: MRI of the primary (deep, lobulated, myxoid/T2-bright mass); planned biopsy at the treating sarcoma unit; confirm NR4A3 rearrangement (e.g. EWSR1-NR4A3) on molecular testing.
- Surgery: wide resection with clear margins is the mainstay.
- Adjuvant therapy: EMC is relatively chemo/radio-resistant, so radiotherapy/chemotherapy have a limited/selective role.
- Surveillance: long-term follow-up (including the chest) because of late local recurrence and metastasis.
- Setting: specialist sarcoma multidisciplinary team; avoid unplanned excision of an undiagnosed deep mass. In the largest series most initial excisions were intralesional or marginal, which is precisely the pattern that produces the 48 percent local-recurrence rate.
The pathway that gets this right starts before the diagnosis is known: a deep mass larger than 5 cm should travel the route set out in soft-tissue masses and sarcoma referral, with imaging interpreted as in MRI of soft-tissue lesions and tissue obtained according to biopsy principles. The two myxoid tumours most often confused with it have their own pages - myxofibrosarcoma and, for the myxoid subtype, liposarcoma - and the bone tumour whose name it borrows is chondrosarcoma, with which it shares nothing but a word.
Two points define safe practice in extraskeletal myxoid chondrosarcoma. First, the name is misleading: despite 'chondrosarcoma', it is not a true cartilage tumour but a distinct soft-tissue sarcoma defined by NR4A3 rearrangement, so the diagnosis rests on the molecular finding (most often the EWSR1-NR4A3 fusion) together with the characteristic myxoid, multilobular histology, and morphological/fusion variants mean the molecular result is particularly useful. Second, and clinically most important, its behaviour is indolent but relapsing over a long horizon: patients may do well for years, yet local recurrence and late metastases (often pulmonary) occur, so short-term disease-free status is not reassurance - prolonged surveillance, including chest imaging, is essential. Because EMC is relatively resistant to chemotherapy and radiotherapy, wide surgical resection with clear margins is the mainstay of treatment, with adjuvant therapy playing only a limited, selective role, and management should be at a specialist sarcoma centre with a planned biopsy before any definitive surgery.
The NR4A3 Fusion: Translocation, and Why EWSR1 Alone Is Not Enough
- The gene and the translocation. NR4A3 (also called NOR1 / CHN / TEC) is a nuclear orphan-receptor transcription factor on chromosome 9q22. The commonest fusion is EWSR1-NR4A3 from t(9;22)(q22;q12) (about two-thirds of cases), which places NR4A3 under the strong EWSR1 promoter and drives aberrant transcription. Variant partners include TAF15-NR4A3 (t(9;17)), TCF12-NR4A3 (t(9;15)) and FUS-NR4A3, plus rarer novel fusions (e.g. ACTB-NR4A3, FUS-NR4A2).
- Why the NR4A3 partner matters - not just EWSR1. EWSR1 is a promiscuous fusion gene rearranged in many sarcomas - Ewing sarcoma (EWSR1-FLI1), clear cell sarcoma (EWSR1-ATF1), desmoplastic small round cell tumour (EWSR1-WT1), angiomatoid fibrous histiocytoma (EWSR1-CREB1) and others - so an EWSR1 rearrangement alone is not specific; it is the NR4A3 partner (on RT-PCR/FISH/NGS) that defines EMC.
Q: What is the defining molecular abnormality of EMC, and why must the NR4A3 partner be identified?
A: EMC is defined by NR4A3 rearrangement - most often EWSR1-NR4A3 from t(9;22)(q22;q12) (~two-thirds), with TAF15-NR4A3, TCF12-NR4A3 and FUS-NR4A3 variants. NR4A3 (NOR1) is a nuclear orphan-receptor transcription factor on 9q22; the fusion drives aberrant transcription. Because EWSR1 is a promiscuous fusion gene (Ewing, clear cell sarcoma, DSRCT, AFH), EWSR1 rearrangement alone is not specific - it is the NR4A3 partner that clinches EMC.
Mnemonics & Memory Aids
MYXOID
Hook:MYXOID: Myxoid/multilobular, Y not truly cartilage, NR4A3 (X) fusion, Often deep thigh, Indolent but relapsing, Do wide resection + surveillance.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A deep thigh sarcoma is reported as extraskeletal myxoid chondrosarcoma. What does the name actually mean, and how would you manage it?”
What it is
- Rare soft-tissue sarcoma; NOT true cartilage despite the name
- Defined by NR4A3 rearrangement (EWSR1-NR4A3 most common; FUS/TAF15 variants)
- Uncertain differentiation
Presentation & histology
- Deep mass of proximal limbs/limb girdles (thigh), adults
- Myxoid matrix, multilobular architecture
- Cords/clusters of eosinophilic ovoid-to-short-spindle cells (variants exist)
Behaviour
- Survival 90 percent at 5 years, 70 at 10, 60 at 15 (n=117, median follow-up 9 years)
- Local recurrence 48 percent (often repeated); metastases 46 percent - often late, to lung
- Adverse: older age, larger size, proximal-limb site. Grade has NO prognostic value; local recurrence did not predict death
- Short-term disease-free status is not reassurance
Management
- Planned biopsy + NR4A3 confirmation; MRI primary
- Wide resection is the mainstay (chemo/radio-resistant)
- Prolonged surveillance (incl. chest); sarcoma-centre care
Evidence & Key Studies
Extraskeletal myxoid chondrosarcoma - morphological and molecular features
- Extraskeletal myxoid chondrosarcoma is a rare soft-tissue sarcoma characterised by a myxoid matrix, multilobular architecture, and eosinophilic ovoid-to-short-spindle cells arranged in cords, clusters or reticular patterns, with NR4A3 gene rearrangement.
- Tumours occurred in adults (median ~49 years) in sites such as the buttock, thigh, paravertebral region and elbow, with a range of sizes; morphological variants (solid, rhabdoid, biphasic, spindle-cell) were seen.
- Molecular testing identified EWSR1-NR4A3 fusions and novel variant fusions (e.g. FUS-NR4A2, ACTB-NR4A3, FUS-NR4A3), expanding the genetic spectrum - underscoring the diagnostic value of NR4A3 testing.
Extraskeletal myxoid chondrosarcoma: a reappraisal of its morphologic spectrum and prognostic factors based on 117 cases
- 117 previously unreported cases from a single musculoskeletal tumour centre. Male-to-female ratio 2 to 1, median age 52 years (range 6 to 89), median size 7 cm (range 1.1 to 25). All arose in deep subcutis or deeper, 80 percent in the proximal extremities or limb girdles and 20 percent in the trunk. Most initial excisions were intralesional or marginal.
- Follow-up in 99 cases, median 9 years (2 months to 22 years): local recurrence in 40 of 83 (48 percent), 23 of whom recurred repeatedly; metastases in 35 of 76 (46 percent). Estimated survival 90 percent at 5 years, 70 percent at 10 and 60 percent at 15 - a pattern the authors say distinguishes EMC from low-grade sarcomas.
- On multivariate analysis the adverse factors were older age, larger tumour size and proximal-extremity or limb-girdle location. Metastasis reduced survival; local recurrence did not. Histologic grading had no prognostic value. Cellular non-myxoid foci mimicking chondroblastoma, Ewing sarcoma, synovial sarcoma, fibrosarcoma and rhabdoid tumour were present in 29 percent. The series is retrospective, single-centre, and predates routine NR4A3 molecular testing.
The defining features of extraskeletal myxoid chondrosarcoma - the myxoid matrix, multilobular architecture, cords/clusters of eosinophilic ovoid-to-short-spindle cells, the NR4A3 rearrangement (EWSR1-NR4A3 most common, with variant fusion partners), the adult age and deep proximal/limb-girdle sites, and the morphological variants - come from the cited Chen series. The fact that EMC does not show true cartilage differentiation despite its name, its indolent-but-relapsing long-term behaviour with late metastasis, its chemo/radio-resistance, and wide resection with prolonged surveillance as management are standard, well- established teaching. The survival rates, recurrence and metastasis proportions, demographics, prognostic factors and the finding that histologic grading carries no prognostic value come from the Meis-Kindblom series, which is retrospective, single-centre and predates routine NR4A3 testing. No randomised trial compares any adjuvant regimen in EMC, no systemic agent has an established survival benefit, and no surveillance interval or duration has been validated - so although the late-relapse pattern justifies long follow-up, no schedule is quoted here as though it were evidence-based.