Who Benefits, When, and at What Cost
- Tumours differ markedly in RADIOSENSITIVITY. RADIOSENSITIVE tumours include EWING SARCOMA, lymphoma and myeloma of bone, and METASTASES (treated palliatively); RADIORESISTANT tumours include OSTEOSARCOMA and CHONDROSARCOMA, which are managed primarily by SURGERY (RT has only a palliative/limited role for unresectable disease).
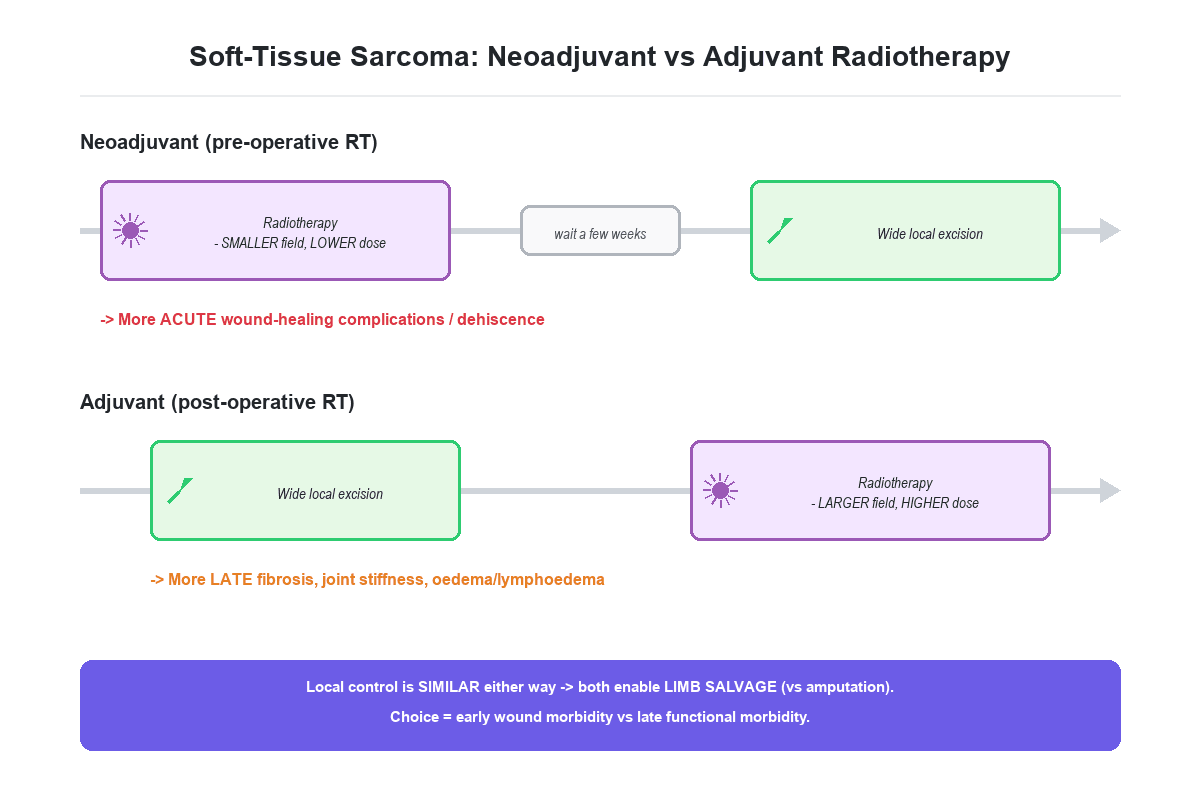
- In SOFT-TISSUE SARCOMA, radiotherapy combined with LIMB-SPARING WIDE EXCISION improves LOCAL CONTROL for high-grade, large or deep tumours and allows LIMB SALVAGE instead of amputation; it is given either NEOADJUVANT (pre-operatively) or ADJUVANT (post-operatively).
- The NEOADJUVANT vs ADJUVANT trade-off is high-yield: PRE-OPERATIVE RT uses a SMALLER field and LOWER dose (and may downsize the tumour) but causes MORE acute WOUND-HEALING complications/dehiscence; POST-OPERATIVE RT uses a LARGER field and HIGHER dose and causes MORE LATE effects (fibrosis, joint STIFFNESS, oedema/lymphoedema) - both achieve similar local control.
- RADIOSENSITIVE PRIMARY bone tumours: EWING SARCOMA is radiosensitive and RT provides local control where surgery is not feasible or margins are inadequate (alongside chemotherapy); bone LYMPHOMA and solitary plasmacytoma/MYELOMA are very radiosensitive and often treated with RT; by contrast OSTEOSARCOMA is relatively radioRESISTANT (surgery + chemotherapy).
- For METASTATIC bone disease, PALLIATIVE RT relieves PAIN, treats an impending or pathological fracture (typically AFTER internal fixation/stabilisation), and is central to managing metastatic SPINAL CORD COMPRESSION (with or without surgical decompression) - a key part of the orthopaedic-oncology team's work.
- MODALITIES include external-beam RT (conventional or IMRT), BRACHYTHERAPY, stereotactic body RT (SBRT) and PROTON-BEAM therapy (useful for chordoma and spinal tumours to spare the spinal cord); COMPLICATIONS are acute (skin reaction, wound problems) and late (fibrosis, stiffness, oedema, growth arrest in children, insufficiency FRACTURE and, years later, RADIATION-INDUCED SARCOMA).
- “Radiosensitive: Ewing, lymphoma, myeloma, metastases (palliative). Radioresistant: osteosarcoma, chondrosarcoma (surgery-based).
- “Soft-tissue sarcoma + limb-sparing surgery: neoadjuvant RT (smaller field/dose, MORE wound complications) vs adjuvant RT (larger field/dose, MORE late fibrosis) - similar local control.
- “Palliative RT for bone mets (pain, post-fixation, cord compression). Late complications: fibrosis, insufficiency fracture, RADIATION-INDUCED SARCOMA.
Smaller field, lower dose; may downsize the tumour - but more acute WOUND complications/dehiscence.
Larger field, higher dose - but more LATE fibrosis, joint stiffness and oedema. Similar local control to neoadjuvant.
Radiosensitivity & the Role of RT
Radiotherapy kills tumour cells by causing DNA damage, and tumours vary greatly in how sensitive they are. RADIOSENSITIVE musculoskeletal tumours include Ewing sarcoma, lymphoma and myeloma of bone, and metastases (treated palliatively), so RT has a major therapeutic role in these. RADIORESISTANT tumours - notably osteosarcoma and chondrosarcoma - are managed primarily by surgery (with chemotherapy for osteosarcoma), and RT is reserved for unresectable or palliative situations. Understanding this spectrum determines whether RT is curative-intent, an adjunct to surgery, or palliative.
Soft-Tissue Sarcoma: Limb Salvage
For high-grade, large or deep soft-tissue sarcoma, the combination of wide local excision and radiotherapy achieves local control comparable to amputation while preserving the limb. RT can be given:
- Neoadjuvant (pre-operative): a smaller field and lower dose, which can downsize the tumour and reduce late effects, but at the cost of more acute wound-healing complications and dehiscence (so some centres delay surgery several weeks after RT).
- Adjuvant (post-operative): a larger field and higher dose, with more late fibrosis, joint stiffness and oedema/lymphoedema. Local control is similar between the two; the choice balances early wound morbidity against late functional morbidity. RT is generally indicated for high-grade or large/deep tumours and for close/positive margins.
Put a number on "more wound complications", because that is the whole decision. The randomised trial that settled it allocated 190 adults with limb soft-tissue sarcoma to pre-operative radiotherapy (50 Gy in 25) or post-operative radiotherapy (66 Gy in 33). Wound complications within 120 days occurred in 35% of the pre-operative group and 17% of the post-operative group - an absolute difference of 18% (95% CI 5 to 30, p=0.01). Roughly one in three irradiated-then-operated patients has a wound problem, against one in six operated-then-irradiated.
Two refinements matter more than the headline. Tumour size and anatomical site were themselves significant predictors, so the 35% is not uniform - a large proximal thigh sarcoma with generous soft-tissue cover is a different proposition from a distal leg or foot, where the skin is thin, the coverage poor and a wound problem is far harder to salvage. And overall survival was slightly better in the pre-operative group (p=0.0481), which is why the higher wound rate has not driven practice to post-operative treatment: the trade-off is early wound morbidity against late fibrosis, with a possible survival signal in favour of the pre-operative arm.
Dose and Fractionation for the Common Indications
- Soft-tissue sarcoma. Neoadjuvant is typically around 50 Gy in 25 fractions (with surgery classically about 4-6 weeks later to limit wound complications); adjuvant is a higher 60 to 66 Gy over a larger field with a tumour-bed boost - the higher dose and larger field explaining the greater late fibrosis. (Ultra-hypofractionated regimens, e.g. 30 or more Gy in 5 fractions, are under study - per the cited Fan cohort.)
- Palliative bone metastases. A single 8 Gy fraction relieves pain as effectively as multifraction schedules (e.g. 20 Gy in 5 or 30 Gy in 10 fractions), though single-fraction has a higher re-treatment rate; multifraction is often preferred for cord compression, post-operative fields or a large soft-tissue component.
- SBRT. High dose in a few fractions for oligometastatic disease and spinal metastases (including relatively radioresistant histologies).
- Ewing sarcoma. Definitive RT uses a moderate-to-high dose integrated with chemotherapy when surgery is not feasible or margins are inadequate.
Know the standard doses: STS neoadjuvant ~50 Gy/25 (surgery ~4-6 weeks later) vs adjuvant 60-66 Gy (the higher dose/larger field = more late fibrosis). Palliative bone metastasis = a single 8 Gy (as good as 30 Gy/10 for pain, higher re-treatment rate). SBRT for oligometastatic/spinal disease; Ewing gets a moderate-high definitive dose with chemo.
How the Field Is Planned - and Why It Matters to the Surgeon
Several of the late complications are determined by field design, and three planning rules are the surgeon's business because they constrain what the surgeon does.
- Spare a longitudinal strip of skin and subcutaneous tissue. Circumferential irradiation of a limb destroys the lymphatic channels running along its length, and the result is the intractable distal lymphoedema listed among the late effects. Modern conformal and IMRT planning deliberately leaves an unirradiated corridor, and a limb should not be irradiated circumferentially unless there is no alternative.
- The biopsy tract and any drain sites must lie within the field. They are contaminated by definition and are treated as part of the tumour. This is the reason a biopsy tract has to be in line with the future incision and a drain brought out in line with it too - a transversely placed tract or a remote drain site forces the radiotherapy field to be enlarged, or leaves contaminated tissue outside it. The biopsy principles are in Biopsy Principles and Techniques.
- Bone and joint dose are limited where possible, because irradiated bone is the substrate for the insufficiency fracture noted below, and an irradiated joint stiffens.
And the sequencing rule for the surgeon: after neoadjuvant radiotherapy, operate at around 4 to 6 weeks - long enough for the acute skin reaction to settle, not so long that fibrosis sets in. Plan the closure before starting: an irradiated bed with a large defect is a plastic-surgical problem, and involving them after the wound has broken down is worse than involving them before the incision.
Radiosensitive Primaries, Metastases & Modalities
- Ewing sarcoma: radiosensitive - RT gives local control when surgery is not feasible or margins are inadequate, integrated with chemotherapy.
- Bone lymphoma and solitary plasmacytoma/myeloma: very radiosensitive and frequently treated with RT.
- Osteosarcoma/chondrosarcoma: radioresistant - surgery is the mainstay (RT palliative/unresectable only).
- Bone metastases: palliative RT relieves pain, is given after internal fixation of an impending/ pathological fracture, and treats metastatic spinal cord compression (with or without surgery).
- Modalities: external-beam RT (conventional/IMRT), brachytherapy, SBRT, and proton-beam therapy (e.g. for chordoma and spinal tumours, to spare the spinal cord).
Radiotherapy carries acute and late costs that the orthopaedic team must anticipate. Acutely, especially with PRE-OPERATIVE RT for soft-tissue sarcoma, there are significant wound-healing complications and dehiscence (negative-pressure wound therapy and delayed closure help). Late effects include fibrosis, joint stiffness and lymphoedema, growth arrest in children, insufficiency fractures through irradiated bone, and - years to decades later - a radiation-induced sarcoma in the radiation field, which carries a poor prognosis. Giant-cell tumour is generally not irradiated where avoidable because of the malignant- transformation risk. These risks are weighed against the clear oncological benefit of improved local control, and care is delivered through a sarcoma multidisciplinary team.
Radiobiology: Why Tumours Differ in Sensitivity
- The lethal lesion. RT kills cells mainly by DNA double-strand breaks, generated partly via reactive oxygen species - hence the oxygen effect: well-oxygenated cells are more radiosensitive, while hypoxic tumour regions (and the poorly-vascularised, matrix-rich tissue of chondrosarcoma) are relatively radioresistant.
- The 4 Rs of fractionation. Dividing the dose exploits Repair of sublethal damage (normal late-responding tissue repairs between fractions better than tumour), Redistribution of cells into radiosensitive phases (mitosis/late G2), Repopulation (tumour can regrow during a course - avoid prolonged gaps), and Reoxygenation (previously hypoxic cells reoxygenate and become more sensitive) - net effect: kill tumour while sparing normal tissue.
- The alpha/beta ratio. High (around 10 Gy) for early-responding tissue and most tumours; low (around 3 Gy) for late-responding normal tissue and slow-growing tumours (chondrosarcoma, chordoma) - low-alpha/beta tissues are relatively spared by fractionation but benefit from higher dose-per-fraction (the rationale for hypofractionation/SBRT and proton therapy in chordoma).
- Intrinsic radiosensitivity. Lymphoid and Ewing cells are intrinsically sensitive; osteosarcoma and chondrosarcoma are intrinsically resistant.
RT kills by DNA double-strand breaks (oxygen-dependent - hypoxia = resistance). Fractionation works via the 4 Rs (Repair, Redistribution, Repopulation, Reoxygenation). The alpha/beta ratio is high (~10) for tumours/early tissue and low (~3) for late-responding/slow tumours (chondrosarcoma, chordoma) - which is why those favour few large fractions (SBRT/protons). Chondrosarcoma's avascular matrix and osteosarcoma's intrinsic resistance explain their radioresistance.
Mnemonics & Memory Aids
SENSITIVE
Hook:Radiosensitive MSK tumours: Ewing, Lymphoma, Myeloma, Metastases (osteosarcoma/chondrosarcoma are NOT).
PRE vs POST
Hook:PRE = wounds; POST = late fibrosis; similar local control.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Which musculoskeletal tumours are radiosensitive and which are radioresistant, and how does radiotherapy contribute to soft-tissue sarcoma treatment?”
“What is the role of palliative radiotherapy in metastatic bone disease, and what are the late complications of radiotherapy?”
Radiosensitivity
- Radiosensitive: Ewing sarcoma, lymphoma, myeloma, metastases (palliative)
- Radioresistant: osteosarcoma, chondrosarcoma (surgery-based)
- Proton beam for chordoma/spinal tumours (spare cord)
Soft-tissue sarcoma
- RT + wide excision -> local control + limb salvage (high-grade/large/deep)
- Neoadjuvant (pre-op): smaller field/dose; MORE wound complications
- Adjuvant (post-op): larger field/dose; MORE late fibrosis/stiffness/oedema
Metastases
- Palliative RT for pain
- After internal fixation of impending/pathological fracture
- Metastatic spinal cord compression (+/- surgery)
Complications
- Acute: skin reaction, wound complications/dehiscence (esp pre-op STS)
- Late: fibrosis, stiffness, lymphoedema, growth arrest, insufficiency fracture
- Radiation-induced sarcoma (years later); avoid RT in GCT (malignant transformation)
Evidence & Key Studies
Preoperative versus postoperative radiotherapy in soft-tissue sarcoma of the limbs: a randomised trial
- 190 adults with limb soft-tissue sarcoma randomised to preoperative radiotherapy (50 Gy in 25 fractions, n=94) or postoperative radiotherapy (66 Gy in 33 fractions, n=96), stratified by tumour size above or below 10 cm.
- Wound complications within 120 days occurred in 35% (31 of 88) of the preoperative group versus 17% (16 of 94) of the postoperative group - an absolute difference of 18% (95% CI 5 to 30, p=0.01).
- Tumour size and anatomical site were also significant independent risk factors for wound complications, so the risk is not uniform across sites.
- Overall survival was slightly better in the preoperative group (p=0.0481), which is why the higher wound rate has not moved practice decisively to postoperative treatment.
Ultra-hypofractionated versus standard preoperative radiotherapy for soft-tissue sarcoma: matched cohort
- Preoperative radiotherapy (standard or ultra-hypofractionated) before wide excision gave excellent disease (local) control for soft-tissue sarcoma.
- Major wound complications were common (about 30-44%) and more frequent/earlier with ultra-hypofractionated RT, prompting delayed surgical resection to mitigate them.
- Local control and distant metastasis did not differ between the regimens - illustrating the role and the wound-morbidity cost of pre-operative RT.
Wound healing complications after radiotherapy for limb soft-tissue sarcoma
- Radiotherapy is recommended for G2-G3 large soft-tissue sarcoma alongside radical wide excision to improve local control.
- Both neoadjuvant and adjuvant RT were significant risk factors for short- and long-term wound complications (odds ratios ~3.5-5.2) and longer hospital/outpatient care.
- The oncological benefit must be balanced against radiogenic wound morbidity; negative-pressure therapy may help prevent complications.
The role of pre-operative RT in achieving local control for soft-tissue sarcoma and its wound-complication cost come from the cited Fan study, and the increased short- and long-term wound complications with both neoadjuvant and adjuvant RT from the cited Dal Pos study. The radiosensitive-versus- radioresistant tumour spectrum, the palliative role for metastases, and the late complications (fibrosis, insufficiency fracture, radiation-induced sarcoma) are standard, well-established oncology teaching. The 35% versus 17% wound-complication figures, the 50 Gy/25 and 66 Gy/33 arms, the size-and-site effect and the survival signal come from the cited O'Sullivan randomised trial. The field-planning rules - sparing a longitudinal strip to protect lymphatic drainage, and including the biopsy tract and drain sites - follow Biopsy Principles and Techniques, which is where the requirement to site a tract in line with the future incision is set out. (See also Soft Tissue Masses and Sarcoma Referral, Ewing Sarcoma, Osteosarcoma, Chondrosarcoma and Metastatic Bone Disease.)