Nursemaid's Elbow (Pulled Elbow / Radial Head Subluxation)
Classic pull history, child 1-4 years, arm held pronated and slightly flexed, refuses to use it, but no swelling, no deformity, no focal bony tenderness. Reduce clinically - no X-ray needed.
Swelling, deformity, focal bony tenderness, a fall/direct-trauma mechanism, an atypical history (consider non-accidental injury), or failed reduction. Radiograph before manipulation and refer as needed.
PULLED
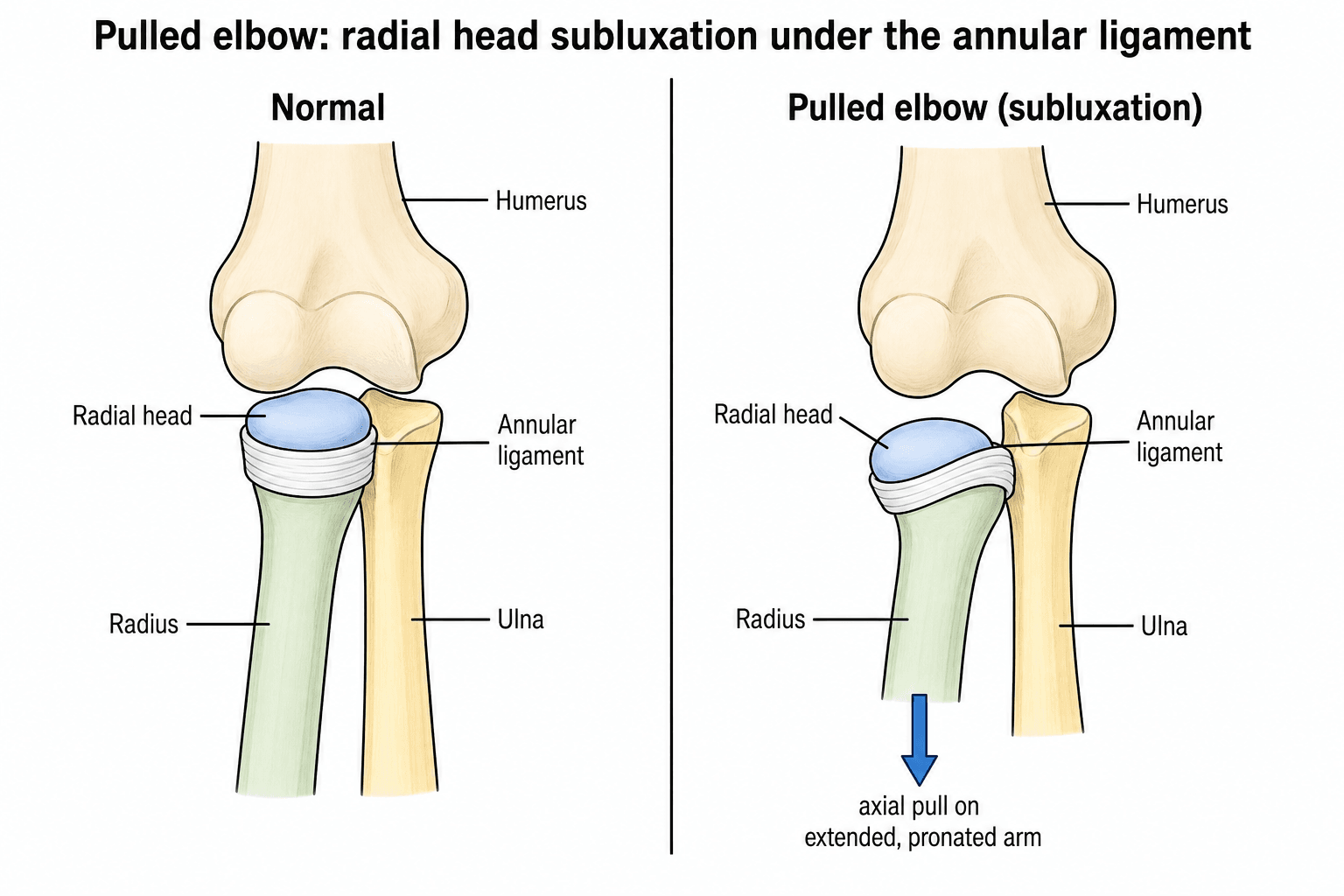
Hook:A PULLED elbow: pull on a pronated arm, radial head under the annular ligament, reduce by hyperpronation.
REDUCE
Hook:REDUCE a pulled elbow: hyperpronate at 90 degrees; click and arm use = done.
SWIFT red flagsWhen it is NOT a simple pulled elbow (X-ray / refer)
Hook:Any SWIFT red flag (Swelling, Wrong history, Inability to use post-reduction, focal Tenderness, Two failed attempts) means radiograph and refer — exclude a fracture.
Overview & Epidemiology
Nursemaid's (pulled) elbow is one of the commonest musculoskeletal injuries of early childhood and a frequent paediatric emergency-department presentation. It clusters between about 1 and 4 years (occasionally up to 5–6, and reported even in infants), and becomes rare once the radial head enlarges and the annular ligament tightens with growth, so it is essentially not seen in adults. It is slightly more common in girls and on the left side. Importantly, roughly half of cases present without a clear "pull" history or with an unwitnessed/atypical mechanism — which is exactly when a fracture must be actively excluded. The recurring exam theme is that this is a benign, clinical diagnosis with a simple, highly effective bedside cure — the skill is recognising it, distinguishing it from a fracture, and reducing it correctly first time.
Pathophysiology & Mechanism
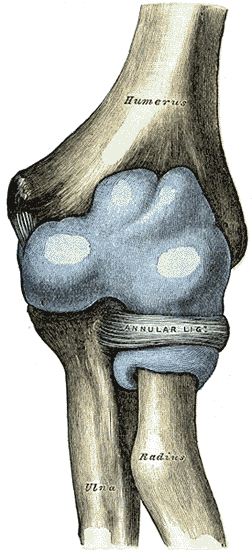
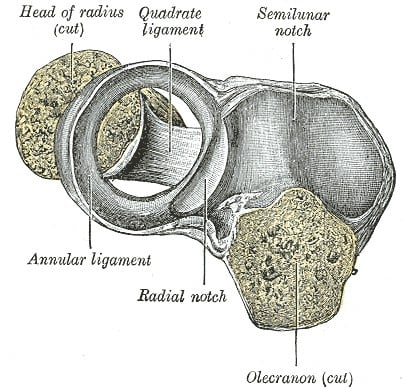
The annular ligament encircles the head and neck of the radius, securing it against the radial notch of the ulna at the proximal radio-ulnar joint while allowing rotation (pronation/supination). In young children the radial head is relatively small and incompletely ossified and the annular ligament is lax, so a sudden axial pull on an extended, pronated forearm can let the radial head slip partially out from under the annular ligament, which becomes interposed - a subluxation. This is why the typical cause is a child being lifted or swung by the hand (the practice should be discouraged), and why the injury becomes rare once the radial head enlarges with growth.
Recent ultrasonographic work has refined the mechanism: it is not only the annular ligament but also the supinator muscle (and its aponeurotic edge) that becomes interposed in the radiohumeral joint (Kimura). This explains two things examiners like — why the injury occurs with the forearm pronated (the supinator is stretched), and why both reduction manoeuvres work: hyperpronation unwinds the trapped tissue, while supination-flexion relaxes the supinator to let it slip back out.
Clinical Presentation & Diagnosis
- A young child (commonly 1-4 years) who suddenly stops using one arm after a pull
- The arm is held close to the body, slightly flexed and pronated
- Little or no pain at rest, no swelling, no deformity
- Resists supination and overhead use of the arm
- Clinical - the classic history plus this presentation is diagnostic
- Radiographs are NOT routine and are usually normal
- Image only to exclude a fracture: atypical/traumatic history, swelling, focal bony tenderness, or failed reduction
Differential diagnosis of the toddler who will not use an arm
A pulled elbow is the commonest cause, but "pseudoparalysis" of an arm in a young child has a differential that must be actively excluded before manipulating:
- Occult fracture — supracondylar, lateral humeral condyle, radial neck, or a toddler's fracture pattern; suggested by swelling, deformity, focal bony tenderness or a fall/direct-trauma mechanism.
- Septic arthritis or osteomyelitis of the elbow/forearm — the child is systemically unwell, febrile, with warmth, swelling and pain on any passive movement (true pseudoparalysis); check inflammatory markers and do not "reduce."
- Clavicle fracture / shoulder pathology — referred reluctance to use the whole limb; examine the whole arm, not just the elbow.
- Non-accidental injury — an inconsistent, changing or implausible history, or injuries of differing ages, is a safeguarding red flag.
- Brachial plexus / neurological causes — rare, but a flaccid arm without a clear pull warrants neurological examination.
If any of these is suspected, image and investigate before attempting reduction.
Investigations
There is no routine investigation — a typical pulled elbow is diagnosed and treated clinically. Imaging is targeted:
- Radiographs are obtained only to exclude a fracture (atypical/traumatic history, swelling, deformity, focal bony tenderness, or failed reduction). They are usually normal in a true pulled elbow; note that the inadvertent supination involved in positioning for an AP film sometimes reduces the subluxation incidentally.
- Point-of-care ultrasound (POCUS) is an emerging, radiation-free aid in the atypical case: it can confirm pulled elbow (the "hook sign" of the displaced annular ligament/supinator) and screen for fracture before reduction. In a single-centre series (McCreary) POCUS identified pulled elbow with high sensitivity and specificity and reduced unnecessary radiographs — useful precisely for the ~50% with an unclear history.
- Consider non-accidental injury whenever the history does not fit the clinical picture.

A pulled elbow is a self-reducing SUBluxation. When a film is taken (atypical/traumatic history or failed reduction), the can't-miss alternative is a true radial head DISLOCATION, and the way to catch it is the radiocapitellar line:
- A line drawn along the long axis of the radial neck/shaft must pass through the centre of the capitellum on EVERY view/projection. If it does not, the radial head is dislocated — that is not a pulled elbow.
- A dislocated radial head with a fractured or plastically bowed ulna is a MONTEGGIA lesion (in children the ulna often bows rather than breaks, so look hard). It is treated by reducing/stabilising the ulna to relocate the radial head — never by repeated "pulled-elbow" manipulation, and a missed Monteggia (chronic radial head dislocation) is a classic, function-limiting pitfall.
- A congenital radial head dislocation (often posterior, with a domed/hypoplastic radial head and a convex capitellum) is the other mimic — bilateral or painless dislocation that was never a pulled elbow.
So in the atypical case: draw the radiocapitellar line and inspect the whole ulna before ever calling it a simple pulled elbow.
Management
Reduction is a simple bedside manoeuvre. With the elbow at about 90 degrees, the two recognised techniques are:
- Hyperpronation - firmly pronate the forearm/wrist (sometimes with slight elbow flexion).
- Supination-flexion - supinate the forearm and then flex the elbow fully.
On Cochrane evidence the hyperpronation manoeuvre has fewer first-attempt failures than supination-flexion (failure ~9% vs ~26%, risk ratio ~0.35, NNT ~6), so it should be tried first. A successful reduction often produces a palpable or audible 'click' over the radial head, and the child typically resumes using the arm within minutes (the most reassuring sign). Office/ED reduction has roughly an 80% success rate with no significant complications.
Hyperpronation manoeuvre — step by step (OSCE):
- Position the child comfortably on the carer's lap; reassure and minimise distress.
- Support the elbow at about 90 degrees of flexion with one hand, placing your thumb gently over the radial head to feel for the click.
- With your other hand holding the distal forearm/wrist, firmly pronate (turn the palm down) - some add slight further flexion at the end.
- Feel/hear the click over the radial head as the subluxation reduces.
- Observe for spontaneous use of the arm over the next few minutes (offer a toy/sticker to the affected hand); this - not the click alone - confirms success.
- If it fails, repeat with the supination-flexion manoeuvre (supinate the forearm, then fully flex the elbow); after two failed attempts, splint, image and refer.
Recurrence is the commonest problem, so examiners expect a plan beyond reassurance:
- Most recurrences simply need re-reduction and reinforced carer advice (lift from under the arms / by the upper arm, not by the hand or wrist); the tendency resolves spontaneously by around five years as the radial head enlarges and the annular ligament tightens.
- For frequent recurrences, a pragmatic step after a successful reduction is a short period (around 1-2 weeks) of above-elbow immobilisation with the forearm in supination and the elbow flexed, to let the annular ligament settle/tighten and break the recurrence cycle.
- The genuinely chronic or atypically recurrent case (recurrence persisting beyond the usual age, or an elbow that will not stay reduced) is no longer a simple pulled elbow — image it (ultrasound/MRI/arthrogram), re-exclude a radial head dislocation, and in the rare refractory child consider referral for surgical annular-ligament reconstruction.
Complications
Pulled elbow is benign with an excellent prognosis. A correctly reduced subluxation leaves no growth disturbance, instability or lasting loss of function, and the tendency to recur resolves spontaneously once the radial head enlarges and the annular ligament tightens (around five years of age), so no long-term treatment or activity restriction is required. A few problems are nonetheless examinable:
- Note
- The commonest issue — recurs in a substantial minority until the child grows; advise carers against pulling/swinging by the hand
- Note
- The important pitfall — a supracondylar, lateral condyle or other elbow fracture mistaken for a pulled elbow and inappropriately manipulated; image when the picture is atypical
- Note
- Failure of two reduction attempts, or persistent non-use, mandates splinting, radiographs and referral; a small number need a period of rest before later successful reduction
- Note
- An atypical or inconsistent history is a safeguarding red flag, not just a fracture flag
- Note
- A correctly reduced pulled elbow leaves no growth disturbance or lasting dysfunction
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 2-year-old is brought in refusing to use the right arm after the parent lifted her by the hand. There is no swelling or deformity and she holds the arm pronated. What is the diagnosis, how do you confirm it, and how do you treat it?”
“The reduction fails after two attempts and the child still will not use the arm. What now, and why does pulled elbow happen in young children but not adults?”
What & why
- Radial head subluxation under the annular ligament (not a dislocation)
- Axial traction on an extended, pronated arm (lifting/swinging by the hand)
- Ages ~1-4; rare after ~5 (radial head enlarges)
Presentation
- Won't use the arm; held close, slightly flexed and pronated
- No swelling, deformity or focal bony tenderness; little pain at rest
- Resists supination/overhead use
Diagnosis
- Clinical - no routine radiographs (usually normal)
- X-ray only to exclude a fracture (atypical/traumatic, swelling, tenderness, failed reduction)
- Consider NAI if the history does not fit
Treatment
- Hyperpronation first (Cochrane: failure ~9% vs ~26%, RR 0.35, NNT ~6)
- Then supination-flexion if needed; success = click + arm use within minutes (~80%)
- If two attempts fail: splint, X-ray, refer; advise against pulling by the hand (recurrence common)
Evidence & Key Studies
The practice-defining study is the Krul Cochrane review (9 trials, 906 children): hyperpronation has fewer first-attempt failures than supination-flexion (9.2% vs 26.4%, RR 0.35, NNT 6) — though the authors stress the evidence is low-quality and a definitive RCT is still needed, so quote it as "probably superior at first attempt." Yamanach (clinical review) gives the bedside picture and the ~80% office success. Kimura adds the pathophysiology (ultrasound shows the supinator, not just the annular ligament, is interposed). McCreary illustrates the modern diagnostic adjunct (POCUS for the atypical case). The exam essentials — the mechanism, the clinical diagnosis, and hyperpronation-first — rest on this base.
Manipulative interventions for reducing pulled elbow in young children
- Across 9 trials (906 children), hyperpronation had fewer first-attempt failures than supination-flexion: 9.2% versus 26.4% (RR 0.35, 95% CI 0.25-0.50).
- Estimated number needed to treat of 6 (95% CI 5-8) to avoid one additional first-attempt failure using hyperpronation.
- Evidence is low-quality and a high-quality RCT is still needed, but pronation appears more effective at first attempt.
Pulled elbow in children
- Pulled elbow is a radial head subluxation from axial traction or a sudden pull of the extended, pronated arm; the practice of swinging children by the hands should be abandoned.
- The child holds the affected arm close to the body without considerable pain, swelling or deformity; once a fracture is excluded it is a clinical diagnosis.
- Office reduction has ~80% success with no complications; the hyperpronation manoeuvre is better than supination-flexion and should be tried first.
Role of the supinator muscle in the pathophysiological mechanism of a pulled elbow
- Reviews ultrasonographic evidence that BOTH the annular ligament and the supinator muscle become interposed in the radiohumeral joint in a pulled elbow
- Explains why the injury occurs with the forearm pronated (the supinator is stretched)
- Provides a mechanistic basis for why both hyperpronation and supination-flexion can reduce the subluxation
What is the utility of point-of-care ultrasound for suspected pulled elbow? A single-centre case series
- Retrospective series of 37 children (0-5 years) with suspected pulled elbow assessed with point-of-care ultrasound (POCUS)
- All 29 with a typical history had a positive POCUS; POCUS correctly identified pulled elbow with 100% sensitivity and specificity in this small series
- POCUS clarified the ~50% with an atypical/unwitnessed history and reduced unnecessary radiographs
- Proposed as an extension of clinical examination to confirm pulled elbow and lower radiation exposure